Article Text

Abstract
Background and Aims: The aetiology for chronic fatigue syndrome (CFS) remains elusive although enteroviruses have been implicated as one of the causes by a number of studies. Since most CFS patients have persistent or intermittent gastrointestinal (GI) symptoms, the presence of viral capsid protein 1 (VP1), enterovirus (EV) RNA and culturable virus in the stomach biopsy specimens of patients with CFS was evaluated.
Methods: 165 consecutive patients with CFS underwent upper GI endoscopies and antrum biopsies. Immunoperoxidase staining was performed using EV-specific monoclonal antibody (mAb) or a control mAb specific for cytomegalovirus (CMV). RT-PCR ELISA was performed on RNA extracted from paraffin sections or samples preserved in RNA later. Biopsies from normal stomach and other gastric diseases served as controls. 75 samples were cultured for EV.
Results: 135/165 (82%) biopsies stained positive for VP1 within parietal cells, whereas 7/34 (20%) of the controls stained positive (p⩽0.001). CMV mAb failed to stain any of the biopsy specimens. Biopsies taken from six patients at the onset of the CFS/abdominal symptoms, and 2–8 years later showed positive staining in the paired specimens. EV RNA was detected in 9/24 (37%) paraffin-embedded biopsy samples; 1/21 controls had detectable EV RNA (p<0.01); 1/3 patients had detectable EV RNA from two samples taken 4 years apart; 5 patient samples showed transient growth of non-cytopathic enteroviruses.
Conclusion: Enterovirus VP1, RNA and non-cytopathic viruses were detected in the stomach biopsy specimens of CFS patients with chronic abdominal complaints. A significant subset of CFS patients may have a chronic, disseminated, non-cytolytic form of enteroviral infection, which could be diagnosed by stomach biopsy.
Statistics from Altmetric.com
Chronic fatigue syndrome (CFS) remains an elusive disease after more than two decades of research.1 In small subsets of patients, Epstein-Barr virus, cytomegalovirus (CMV), parvovirus B19, Brucella, Toxoplasma, Coxiella burnetti, Ross river virus and Chlamydia pneumoniae have been reported to cause prolonged fatigue, fevers and many other symptoms of CFS.2–5 Our recent analysis of 200 patients suggest that CFS may have a number of potentially treatable infectious aetiologies as previously reported; and enteroviruses may be the causative agents in more than half of the patients.3
Enteroviruses cause acute respiratory and gastrointestinal infections, with well-documented tropism for the central nervous system, heart and muscles.6 Earlier studies demonstrated circulating antigen of enterovirus, raised antibody titres and viral RNA in the blood and muscle biopsy specimens of patients with CFS.2 7–11 Cunningham et al showed a possible defect in control of enteroviral RNA synthesis in the muscles of patients with CFS that might permit persistence of the virus.8
Using different primers and reverse transcriptase (RT)-PCR techniques, our and two other laboratories demonstrated enteroviral RNA in the peripheral blood leucocytes of 35% of the CFS patients after obtaining multiple specimens.2 12 13 Treatment with interferon and ribavirin and the combination of α- and γ-interferon resulted in significant improvement of symptoms of CFS and suppression of viral RNA in the blood leucocytes.2 14 The relapse of symptoms and reappearance of viral RNA in the peripheral blood leucocytes after drug discontinuation supported the pathogenic role of enterovirus in CFS.
The major obstacle remains, however, that there is no reliable test to diagnose underlying chronic enterovirus infection in accessible tissues of patients with CFS. Brain, heart and muscles biopsies are unlikely to become standard tests of diagnosis. Swallowed, infected respiratory secretions or virus-contaminated food/water reach the stomach first. Enteroviruses are acid- and bile-resistant, and believed to be common causes of acute gastritis.15 Most patients with CFS have persistent or intermittent, upper and/or lower gastrointestinal (GI) symptoms, referred to as functional dyspepsia or irritable bowel syndrome.16 17 In this report, we investigate the presence of enterovirus (EV) protein, EV RNA and culturable viruses in the stomach biopsy specimens of patients with CFS.
MATERIALS AND METHODS
Patient selection
A total of 165 consecutive patients, fulfilling the CDC criteria for CFS,1 underwent upper GI endoscopies and antrum biopsies. No one was excluded from the analysis. The research project was approved by Little Company of Mary Hospital institution review board, Torrance, California.
Biopsies from stomach of normal volunteers (n = 22, blinded samples, 60% female) and other gastric diseases (n = 12, 9 female, 3 male) served as controls: Helicobacter pylori gastritis (n = 3), non-steroidal anti-inflammatory drug-induced gastritis (n = 2), inflammatory bowel disease (n = 1), eosinophilic gastritis (n = 1), gastro-oesophageal reflux disease (n = 1), MALT lymphoma (n = 2), gastric carcinoma (n = 2).
Immunoperoxidase staining of the paraffin-embedded antrum was performed using enterovirus-specific murine monoclonal antibody (5D8/1, Dako, Carpenteria, CA, USA) directed against a highly conserved, linear, non-conformational epitope of viral capsid protein 1 (VP1), or a CMV mAb with the same isotype (Chemicon, Temecula, CA, USA) as negative control. Standard staining protocol was followed as described previously.18 Briefly, the deparaffinised, hydrated biopsy specimens were treated with 3% H2O2 to remove endogenous peroxidase activity, underwent heat-induced epitope retrieval, blocked with goat serum ±3% bovine serum albumin (BSA), treated with biotin–avidin to remove endogenous biotin in gastric tissue, then incubated sequentially with murine mAb, biotinylated goat anti-mouse antibody (Vectastain ABC reagent, Vector Laboratory), before developing with DAB chromogen. Haematoxylin was used as counterstain.
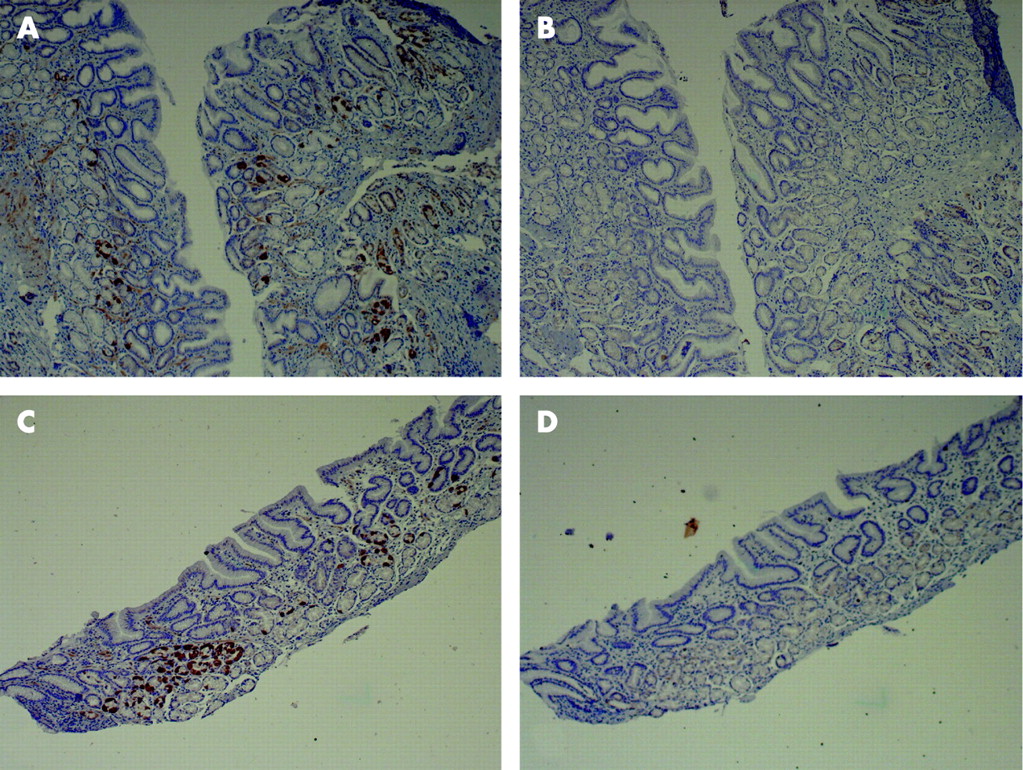
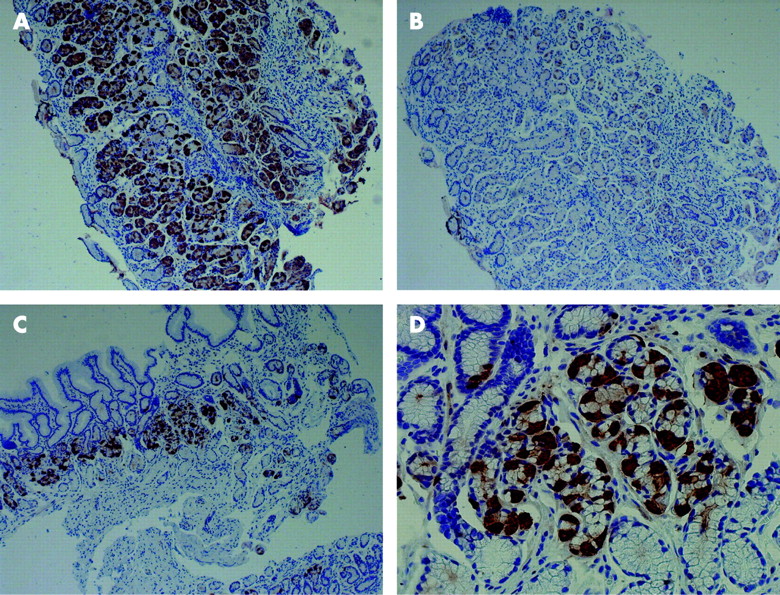
The degree of staining was classified as: 0, none or rare cell stained with 5D8/1; 1+, >10% and <50% cells stained; 2+, ⩾50% cells stained (fig 1).

Peptide inhibition study
The binding epitope for 5D8/1 has been previously defined.19 A 15 amino acid peptide with the sequence Pro-Ala-Leu-Thr-Ala-Val-Glu-Thr-Gly-Ala-Thr-Asn-Pro-Leu-Val was synthesised by Genescript (New Jersey, USA). Varying concentrations of the peptide inhibitor were preincubated with a previously titrated dose of 5D8/1 at 37°C for 30 min prior to performing the immunoperoxidase staining. Bovine serum albumin 10 mg was used as a negative control.
Enteroviral RNA testing
Two to four 10 μM paraffin sections of the antral biopsy specimens from CFS patients and controls were processed with PureLink FFPE RNA isolation kit (Invitrogen, Carlsbad, CA, USA); antrum biopsy specimens preserved in RNA-later were homogenised in 1.5 ml of TriZol LS (Invitrogen). RNA was extracted from 250 μl of the suspension according to the manufacturer’s instructions.
Extracted RNA was amplified with biotinylated primers provided by pan-enterovirus oligodetect kit (Chemicon, Temecula, CA, USA) using Qiagen one-step RT-PCR enzyme kit. The cDNA was detected by hybridising with probe-coated plates, and developed using streptavidin-conjugated with peroxidase, followed by TMB-E. The optical density was determined at 450 nm in an EIA reader. In selected samples, the RNA was re-amplified using non-biotinylated primers (sense 5′ CCT CCG GCC CCT GAA TGC GGC TAA T 3′, antisense 5′ CAA TTG TCA CCA TAA GCA GCC A 3′); the gel-purified, 151 bp cDNA products were cloned into pDrive cloning vector, transformed into E coli (PCR cloning kit, Qiagen). Plasmid-inserts were sequenced by Retrogen (San Diego, CA, USA).
Culture of the stomach tissue
BGMK cells are grown to 50% confluence in DMEM–2% fetal calf serum (FCS) before incubation in the presence of 50 μg/ml of 5-idoxyuridine (5-idu, Sigma, St Louis, MO, USA) for 48 hours.20 21 After removal of 5-idu, the cells were fed with DMEM–2% FCS, containing 10−6 M dexamethasone (dex-DMEM). Untreated BGMK cells were maintained in DMEM–2% FCS. Stomach biopsy specimens, frozen in normal saline, were ground in Opti-Pro (Invitrogen), a serum-free medium. The homogenate was frozen and thawed three times in a dry ice/ethanol bath. A 250 μl portion of the cell lysate was inoculated onto cell monolayer previously treated with dex-DMEM for at least 24–48 hours. After 1 hour of incubation at 25°C, the cell lysates were removed and the cells fed with dex-DMEM. The infected cells were re-fed weekly with dex-DMEM. After 4–6 weeks of incubation, half of the cell monolayers were scraped or trypsinised for enteroviral RNA detection using the procedure described above. The cleared lysates of scraped cells from 6-week-old cultures were passed into a new set of 5-idu, dex-treated BGMK cell cultures to demonstrate the infectivity of the virus product.
RESULTS
At the time of oesophagogastroduodenoscopy, the majority of patients had mild, focal inflammation in the antrum, a few had normal-appearing mucosa and rare patients had diffuse erythema. A total of 157/165 (95%) biopsy specimens had microscopic evidence of mild chronic inflammation, whereas only 8/165 (5%) specimens showed the presence of H pylori by special stain. A total of 135/165 (82%) biopsy specimens stained positive for VP1 within parietal cells, whereas 7/34 (20%) of the controls stained positive (p⩽0.001, χ2 test). A total of 88 (53%), 47 (29%) and 30 (18%) samples showed 2+, 1+ or 0 staining, respectively (fig 2). The sensitivity, specificity, positive and negative predictive values were 82%, 79%, 95% and 47%, respectively. Five of the eight biopsies which stained positive for H pylori were also positive for VP1 staining. Attempts to serotype the viral capsid protein using various neutralising, type-specific mAbs (Chemicon, Temecula, CA) in this immunochemical staining rarely demonstrate staining in the parietal cells. CMV mAb failed to stain any of the biopsy specimens. Specific mAbs for varicella-zoster virus, parainfluenza viruses, adenovirus and respiratory syncytial virus failed to show staining in 10 VP1-positive specimens (data not shown).

The specificity of the antibody binding was demonstrated by repeating the staining experiment with 5D8/1 mAb previously incubated with varying concentrations of epitope-specific peptide. The peptide inhibited the binding in a dose-dependent manner: 1 ng did not show significant inhibition, 10 ng partially inhibited the binding/staining and 100 ng completely blocked the binding (fig 3). BSA 10 mg did not inhibit binding of the antibody.

We attempted to correlate the degree of staining with the functional status of the CFS patients. The capability of performing sedentary work was assessed in most of the patients. Only 15/89 (27%) patients with 2+ staining were able to perform 6–8 hours/day of sedentary work, whereas 33/71 (54%) patients with no staining or 1+ staining could do the same (p = 0.016, Fisher exact test).
Eighteen specimens, containing three or more pieces, demonstrated variable staining; 1–3 of 3–5 pieces stained positive, suggesting potential sampling errors with this biopsy procedure. Biopsy specimens taken from six patients at the onset of the CFS/abdominal symptoms, and 2–8 years later showed positive staining in the paired specimens (fig 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
EV RNA was detected in 9/24 (37%) paraffin-embedded samples from CFS patients; 1/21 controls had detectable EV RNA (p<0.01, Fisher exact test). One of three patients had detectable EV RNA from two samples taken four years apart. Only 22/90 (24%) of the samples preserved in RNA-later were positive for EV RNA despite much larger size of biopsy specimens (20–50 mg wet weight). When examined simultaneously, 19/63 of the samples stained 2+ had detectable EV RNA whereas 7/37 with 0 or 1+ staining were positive (p = 0.07, Fisher exact test).
VP1 staining, RNA analysis and cultures were simultaneously performed on 75 specimens. Table 1 shows the results of VP1 staining and EV RNA detection from the first 13 patients. When incubated with normal BGMK cells for 4 weeks, none of the tissue lysates yielded detectable viral RNA. On the other hand, after 4 weeks’ incubation in BGMK cultures previously treated with 5-idu and dexamethasone, few biopsy specimens yielded detectable EV RNA. EV RNA was detected with higher frequency and intensity at 6 weeks but gradually disappeared as cultures were carried out to 8–12 weeks. No significant cytopathic effect was shown in the EV RNA-positive cultures, whereas wild type strains of enteroviruses would cause major cytopathic changes within one week. When the cleared cell lysates of the 6-week-old infected primary cultures were passed to another set of uninfected, 5-idu, dex-treated BGMK cells, EV RNA was detected in several of the cultures at 4 weeks but disappeared at 8 weeks. The EV RNA in positive cell cultures became negative after attempted expansion and storage. The 151 bp cDNA isolated from five of the positive cultures were confirmed to be EV RNA by sequencing.
DISCUSSION
CFS can be triggered by a number of treatable infections, and our previous work showed that 50% of the first 200 CFS patients had raised neutralising antibody titres for 10 of the top 20 enteroviruses isolated in the USA from 1970 to 2005.33 An estimated 80–90% of our 1400 CFS patients have recurring gastrointestinal symptoms of varying severity, and epigastric and/or lower quadrant tenderness by examination, compared to only 3/100 control subjects (author’s unpublished observations). Finding enterovirus VP1 protein in 82% of stomach biopsy samples seems to correlate with the high percentage of CFS patients with GI complaints. Whether this result represents a patient selection bias or a reflection of possibly higher rate of enterovirus infections in our region will require additional studies involving patient cohorts from different geographic areas. Our CFS patients developed their illnesses at different time points, with average duration of 5.0±4.5 years (range 1–20 years), which would suggest that major outbreaks of enterovirus infection did not cause disproportional cases in this patient cohort.
5D8/1 mAb has been used by a number of investigators to detect a common enteroviral protein in the tissues of infected animals and human tissues, and the specificity has been correlated with viral genome detection or culturable viruses.22–25 Our results showed that a high percentage of CFS patients have stainable viral proteins in the antral tissues, as compared to control subjects. The inhibition of staining by epitope-specific peptide confirms the binding specificity. CMV is a known cause of gastritis/oesophagitis in immunocompromised patients,26 27 yet the CMV mAb we used did not stain any of the specimens taken from CFS patients. Failure to stain the tissue with neutralising, type-specific mAb was not unexpected since these antibodies usually bind conformational epitopes, which are denatured during heat-induced antigen retrieval. Finding enteroviral protein in some of the control subjects could be explained by the high prevalence of enterovirus infections throughout the year, affecting as many as 50 million Americans per year, or 17–25% of the population.4 Viral shedding in stool can persist for weeks after acute infections. It is probable that the control subjects had an asymptomatic or self-limited enterovirus infection within the preceding months. More careful screening of the control subjects may increase the specificity of this test in future studies.
Enteroviral protein was detected in the initial stomach biopsy specimens taken from six patients who developed GI infection before the onset of CFS, and also in biopsy specimens taken years later when the patients had persistent GI symptoms and fatigue. This finding suggests that enterovirus infection initiated the GI symptoms and CFS, and the persistence of the virus years later likely was responsible for the patient’s symptoms. In a few patients, however, GI symptoms predated the onset of CFS but became much worse afterwards. A few patients with prior self-limited enteroviral infection developed CFS and chronic GI symptomatology after another enteroviral infection, as documented by seroconversion to the heterologous virus (author’s unpublished data). Since there are more than 70 human enteroviruses, re-infection is likely to be common; a second infection may be more severe and difficult to eradicate, as shown in animal models.28 Interestingly, the intensity of VP1 staining of the stomach biopsy correlated inversely with functional capacity. Perhaps the tissue viral load is directly related to the severity of the symptom complex.
Furthermore, EV RNA was detected in paraffin-embedded tissue as well as in larger samples preserved in RNA-later, years after the onset of GI symptoms and CFS. Thirty-seven per cent of the stomach biopsy specimens had detectable enteroviral RNA, as compared to 82% by VP1 staining, a finding comparable to the results of Li et al who studied the presence of viral protein and RNA on rheumatic valve tissues by immunochemical staining and in situ hybridisation.29 Surprisingly, stomach biopsy preserved in RNA-later did not have a higher yield of EV RNA. This paradoxical finding could be due to technical problems involved in the procedures. Some of the RNA-positive specimens had negative VP1 staining or vice versa, an observation which may be partly explained by the different pieces of biopsy tissues submitted for different tests.
The growth of non-cytopathic viruses from the stomach biopsy specimens supports persistent infection of the tissues. Interestingly, the stomach homogenate did not infect monolayers of normal BGMK cells but grew in the same cells previously treated with 5-idu and dexamethasone. Pretreatment with 5-idu before virus inoculation has shown increased virus yield and plaque efficiency.19 20 Dexamethasone was added to inhibit cytokine production in 5-idu-treated cells.30 Although the amplified cDNA product was confirmed as an enterovirus sequence, the exact nature of the infectious viral product remained undefined. Furthermore, this experimental procedure was difficult to reproduce since the next 62 samples failed to yield any viral growth even after multiple changes of culturing conditions. More work is needed in defining the optimal cell type and growth condition to isolate the virus from human tissue. Exogenous contamination would be unlikely since no positive virus control was included in the culture experiments.
Although persistent enterovirus infections have been associated with chronic myocarditis, type 1 diabetes and neuromuscular diseases (reviewed in Oberste and Pallansch6), the concept of enteroviral persistence remains controversial.34 Endomyocardial biopsy taken from patients with viral myocarditis demonstrated persistence of enteroviral genome in almost one-third of the samples 1 year after acute infection.31 Muscle biopsy specimens taken from CFS patients, and postmortem examination of brain tissues from one CFS patient, years after the initial infection, also demonstrated the persistence of enteroviral genome.6–9 32 Collectively, these findings clearly support the concept of viral persistence in human tissues, which may be accountable for diverse manifestations of CFS. Nevertheless, tissues from these organs are difficult to obtain, and furthermore, a “dilution effect” likely exists during haematogenous dissemination, which makes these sites less desirable for biopsy than the initial sites of viral replication.
Taken together, the findings of enteroviral protein, RNA and the growth of non-cytopathic viruses in the stomach tissue of CFS patients, years after initial infection, suggest a strong association between enteroviral persistence/infection and CFS. Whether reactivation of persistent enterovirus infection is only an epiphenomenon triggered by another undefined mechanism responsible for CFS could not be answered by our study, but our earlier studies, demonstrating improvement of symptoms with antiviral therapy, suggest that active, persistent viral infection is still of paramount importance.2 14 Although finding a chronic infection of the stomach may not directly prove a similar infection in the brain, muscle or heart, it opens up a new direction in the research for this elusive disease. By inference, a significant subset of CFS patients may have a chronic, disseminated, non-cytolytic form of enteroviral infection, which can lead to diffuse symptomatology without true organ damage. If confirmed, stomach biopsies could be used as a test to document viral persistence, and serve as an objective means to follow the response to antiviral therapy, in addition to quantitation of subjective complaints.
Take-home messages
Enteroviruses cause acute respiratory and gastrointestinal infections, with well-documented tropism for the central nervous system, heart and muscles.
Most patients with chronic fatigue syndrome (CFS) have persistent or intermittent, upper and/or lower gastrointestinal symptoms, referred to as functional dyspepsia or irritable bowel syndrome.
Enteroviral capsid protein 1, RNA and non-cytopathic viruses were detected in the stomach biopsy specimens of CFS patients with chronic abdominal complaints.
A significant subset of patients with CFS may have a chronic, disseminated, non-cytolytic form of enteroviral infection, which could be diagnosed by stomach biopsy.
Acknowledgments
We are indebted to many gastroenterologists in the Torrance area for performing UGI endoscopies and biopsies.
REFERENCES
Footnotes
Funding: This research is supported in part by an unrestricted research grant from Gilead Sciences.
Competing interests: None declared