Article Text

Abstract
Background and aims Molecular target therapy against L-type amino acid transporter 1 (LAT1) is unique and expected to be developed soon. LAT1 expression was investigated in pancreatic cancer as a prognostic predictor.
Methods Surgically resected pancreatic ductal adenocarcinomas (PDAC, n=66) were investigated using immunohistochemistry. For reference, intraductal papillary mucinous carcinomas (IPMC, including intraductal papillary mucinous neoplasm (IPMN) with high-grade dysplasia or with an associated invasive carcinoma, n=13) and adenomas (IPMA, including IPMN with low- and intermediate-grade dysplasia, n=5) were also examined.
Results LAT1 expression scores increased from PDAC to IPMA to IPMC. Kaplan–Meier analysis showed significant differences between LAT1-high and -low scores in PDAC. Even in each Ki-67-labelling index (LI) low and high PDAC group (cut off 40%), high LAT1 expression could also predict poor prognosis. Multivariable analysis showed that LAT1 expression, Ki-67 LI, tumour differentiation and size were individual prognostic factors.
Conclusions LAT1 aberrant overexpression in PDAC predicts poor prognosis, independent of Ki-67 LI, and offers a potential target for future anticancer therapy with its inhibitors.
Statistics from Altmetric.com
Introduction
Pancreatic cancer has long been well known as having one of the worst prognoses of human malignancies, and its prognosis remains poor.1 ,2 Five-year survival for pancreatic cancer is much less than 20%; for true pancreatic ductal adenocarcinoma (PDAC) it is around 0–5% based on the large published series.1 In addition, it has not improved substantially over the past 30 years.2 Therefore, a new innovative therapy for pancreatic cancer is urgently required.
The L-amino acid transporter system responsible for the transport of large neutral amino acids such as leucine, largely depends on the L-type amino acid transporter 1 (LAT1, solute carrier family 7A5), which was originally cloned by Kanai et al.3 LAT1 is expressed in some normal human cells, as well as carcinoma cells such as prostatic, oesophageal, gastric and pulmonary carcinoma.4–7 Previously, we demonstrated that LAT1 expression could be a reliable prognostic marker in prostatic carcinoma, in agreement with the Gleason histological grading system.4 We also showed a correlation between prognosis and LAT1 expression in non-scirrhous gastric carcinoma.7 Therefore, LAT1 overexpression was strongly suggested to be associated with the aggressive phenotype of malignant tumour. In the present study, we examined a series of pancreatic cancers to determine whether altered LAT1 expression related to malignant behaviour independently of cellular proliferation activity such as Ki-67 labelling index (LI), in order to suggest a new possibility of treatment for pancreatic cancer.
Methods
Patients and tissue samples
Sixty-six cases of PDAC and 13 cases of intraductal papillary mucinous carcinomas (IPMC, including intraductal papillary mucinous neoplasm (IPMN) with high-grade dysplasia and with an associated invasive carcinoma) and five adenomas (IPMA, including IPMN with low- and intermediate-grade dysplasia), surgically and consecutively resected at Kitasato University East Hospital from 2001 to 2010, were investigated. All of the resected specimens were fixed in 10% buffered formalin, and the tumour lesions were step-sliced at 5 mm thickness and processed for embedding in paraffin. The largest tumour section of each case was selected and used for H&E staining and immunohistochemical analyses. The WHO histological typing and the International Union Against Cancer pT classification for invasion were applied to all 79 carcinoma cases.8 ,9
Immunohistochemistry
Immunohistochemical staining was performed using 4 μm-thick sections according to the methods previously described.4 Briefly, endogenous peroxidase was blocked with 1% hydrogen peroxide in methanol for 30 min. After retrieving antigenic reactivity, the sections were incubated with primary antibodies, anti-LAT1 (2 µg/ml, J-Pharma, Tokyo, Japan) and anti-Ki-67 (1:100 diluted, Dako, Glostrup, Denmark) at 4°C overnight. After incubation with peroxidase-labelled polymer (ChemMate EnVision kit, Dako) for 30 min, 3,3′-diaminobenzidine (DAB) was applied as the chromogen. Nuclei were counter-stained with Mayer's haematoxylin or 0.3% methyl green.
In selected cases, LAT1 and Ki-67 double immunostaining was performed in order to compare their expression in the same cells. After LAT1 staining with DAB, sections were treated to facilitate antigen retrieval using a microwave oven for 5 min. Ki-67 antibody (1:50 diluted) was then reacted with a mixture of NiCl2-DAB as a different chromogen-blue.
Evaluation of immunohistochemical staining
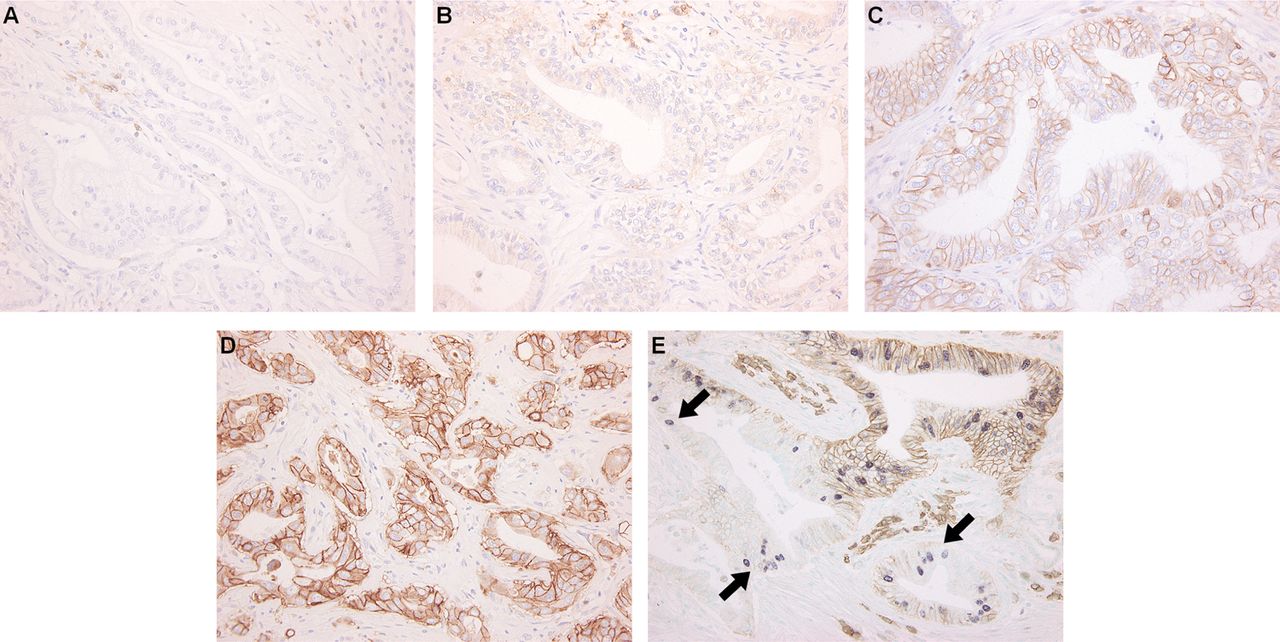
Evaluation of immunoreactivity for LAT1 was performed according to Sinicrope's method10 with minor modifications.4 Based on the immunointensity of the tumour cell membranes, four categories were defined: 0, no staining; 1, weak; 2, moderate; and 3, intense complete membrane staining (figure 1A–D). The stained area was also evaluated, expressed as a percentage of the whole tumour area, and classified: 0, none; 1, 1–10%; 2, 11–30%; and 3, >30%. Immunoreactive LAT1 scores were then calculated by multiplying the values of the two parameters, highest intensity of positivity and area in each case. Two pathologists (NY and IO) scored each case independently without any clinical information. When scores estimated by them were different, exact scores were determined after further review and consensus. LAT1 scores of 6–9 were classified as high and those of 0–4 as low. Ki-67 positive cells were counted in at least 1000 cells of a mainly invasive area, and Ki-67 LI were calculated as percentage values. Less than 40% of the Ki-67 LI was categorised as a Ki-67-low and ≥40% as a Ki-67-high group, according to our results (the average value of Ki-67 LI in PDAC was 35.8%) and other previous reports.11 ,12

L-type amino acid transporter 1 (LAT1) expression in pancreatic ductal adenocarcinoma (PDAC) cells analysed with immunohistochemistry. Based on the immunointensity of the carcinoma cell membrane, four categories were defined: (A) 0, no staining; (B) 1, weak or patchy positive; (C) 2, moderate complete cell membrane staining; and (D) 3, intense complete membrane staining. Lymphocytes also showed LAT1 expression. Nuclear counter staining was done with Mayer's haematoxylin. (E) Double staining with LAT1 and Ki-67 in a representative PDAC case. Several carcinoma cells with Ki-67 expression (nuclear staining with NiCl2-diaminobenzidine (DAB), blue) do not express LAT1 (membranous staining with DAB, brown) (arrows). Nuclear counterstaining was done with methyl green solution. Original magnification, ×100.
Statistical analysis
Data were expressed as mean±SD. Comparisons between groups were conducted using Fisher's protected least significant difference test as a post-hoc test. The statistical significance of differences between Kaplan–Meier survival curves was tested by the log-rank test. Relations between LAT1 score and Ki-67 LI were analysed using Spearman's rank correlation coefficient test. The χ2 test was applied for relations between LAT1 expression and clinicopathological factors. Cox proportional hazard analysis was used for the survival data. The factors significant by univariable analyses were examined in multivariable analysis. StatView software V.5.0 was used for all statistical analyses. All p values <0.05 were considered statistically significant.
Results
Patient characteristics
The 66 PDAC patients (mean age 66 years, range 50–86; 31 women, 35 men) comprised 2 (3%) pT1, 2 (3%) pT2, 49 (74%) pT3 and 13 (20%) pT4 cases. Thirty-seven (56%) were classified as well, 25 (38%) as moderately and 4 (6%) as poorly differentiated adenocarcinomas.8 The thirteen IPMC patients (mean age 65, range 42–78; 2 women, 11 men) comprised 1 (8%) pT1, 8 (61%) pT2, 3 (23%) pT3 and 1 (8%) pT4 cases. The degree of invasion in the IPMC was 5 no stromal, 3 minimal (≤5 mm) and 5 massive (>5 mm). Of the 79 carcinoma cases, 53 patients (PDAC, 51 (77%); IPMC, 2 (15%)) died of the disease after the operation.
LAT1 expression
Normal epithelia of the pancreatic duct and acinus did not express LAT1. However, endocrine cells in the islets of Langerhans showed moderate to strong LAT1 membranous expressions. In addition, lymphocytes also showed moderate immunoreactivity for LAT1 expression, which were used as an internal control. Pancreatic intraepithelial neoplasia sometimes showed mild to moderate expression. Regarding pancreatic tumours, almost all cases showed aberrantly increased LAT1 expression. No significant correlation was found between LAT1 expression and differentiated types of PDAC. Compared to PDAC, IPMC demonstrated significantly higher LAT1 scores (PDAC, 3.5±2.3; IPMC, 6.8±2.3, p<0.0001; figure 2). LAT1 scores of IPMA (4.4±3.2) were between PDAC and IPMC. PDAC showed no difference of LAT1 expressions between invasive and non-invasive areas. However, non-invasive components of IPMC tended to show strong LAT1 expression compared with that of invasive areas (data not shown). No significant correlations were found between LAT1 expression and clinicopathological factors, such as lymphatic and vascular invasion or metastasis (data not shown).
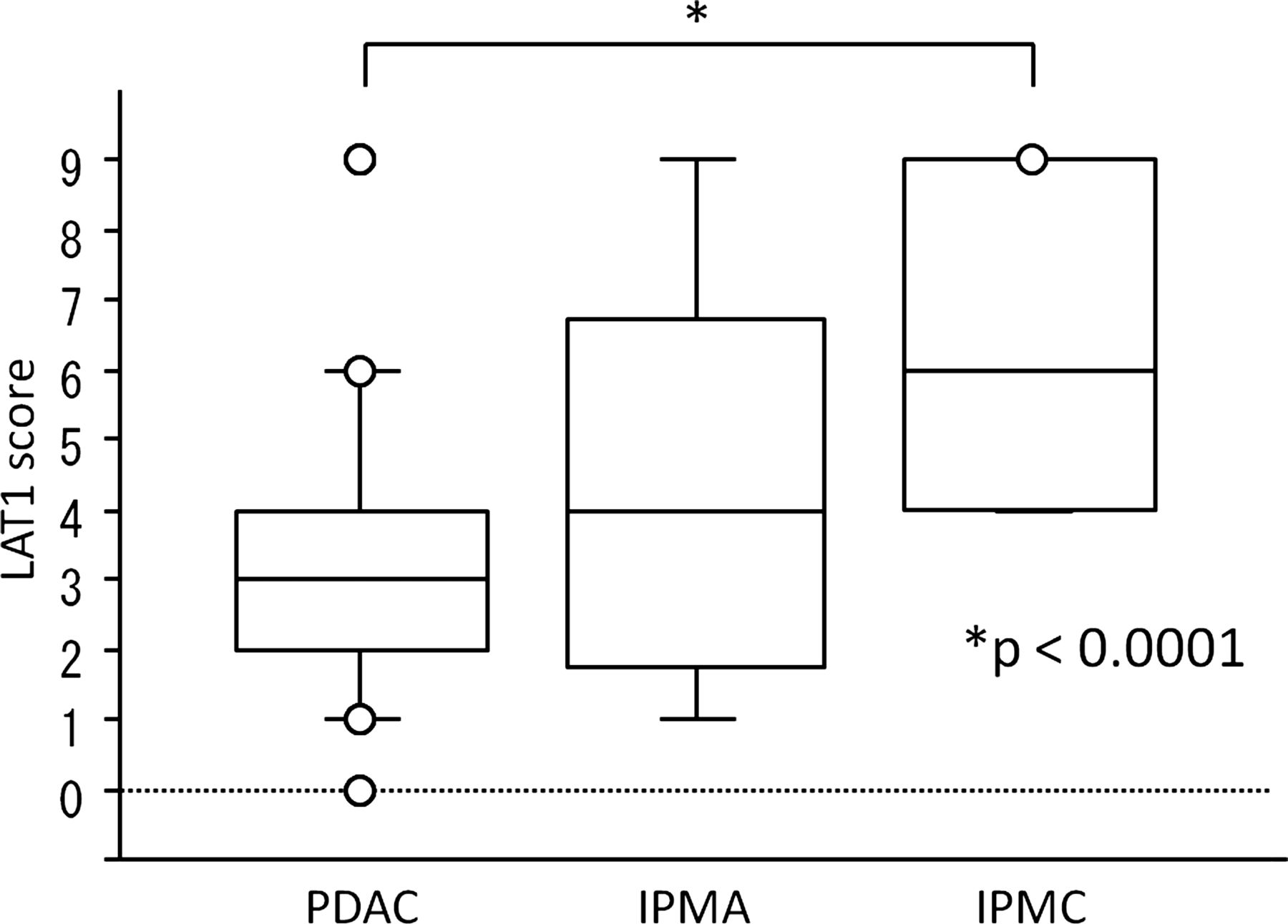
Comparison of L-type amino acid transporter 1 (LAT1) scores of pancreatic tumours. Intraductal papillary mucinous carcinoma showed a significantly higher LAT1 score compared with pancreatic ductal adenocarcinoma (PDAC). IPMA, intraductal papillary mucinous adenoma. *p<0.0001.
Correlation between LAT1 and Ki-67 expression
The IPMA showed low Ki-67 LI (mean 1.7%, range 0.3–4.0%). On the other hand, the Ki-67 LI averaged 35.8% (range 8.4–89.4%) in PDAC and 34.2% (8.9–67.6%) in IPMC with no significant difference. No correlation was found between Ki-67 LI and LAT1 expression in either PDAC or IPMC cases (r=0.145, p=0.200). In the double-stained sections, the cancer cells did not always co-express LAT1 and Ki-67 (figure 1E). There were 59.6±57.3 (range 5–207) per 1000 tumour cells Ki-67-positive cells without LAT1 expression.
Relationship to postoperative cause-specific survival
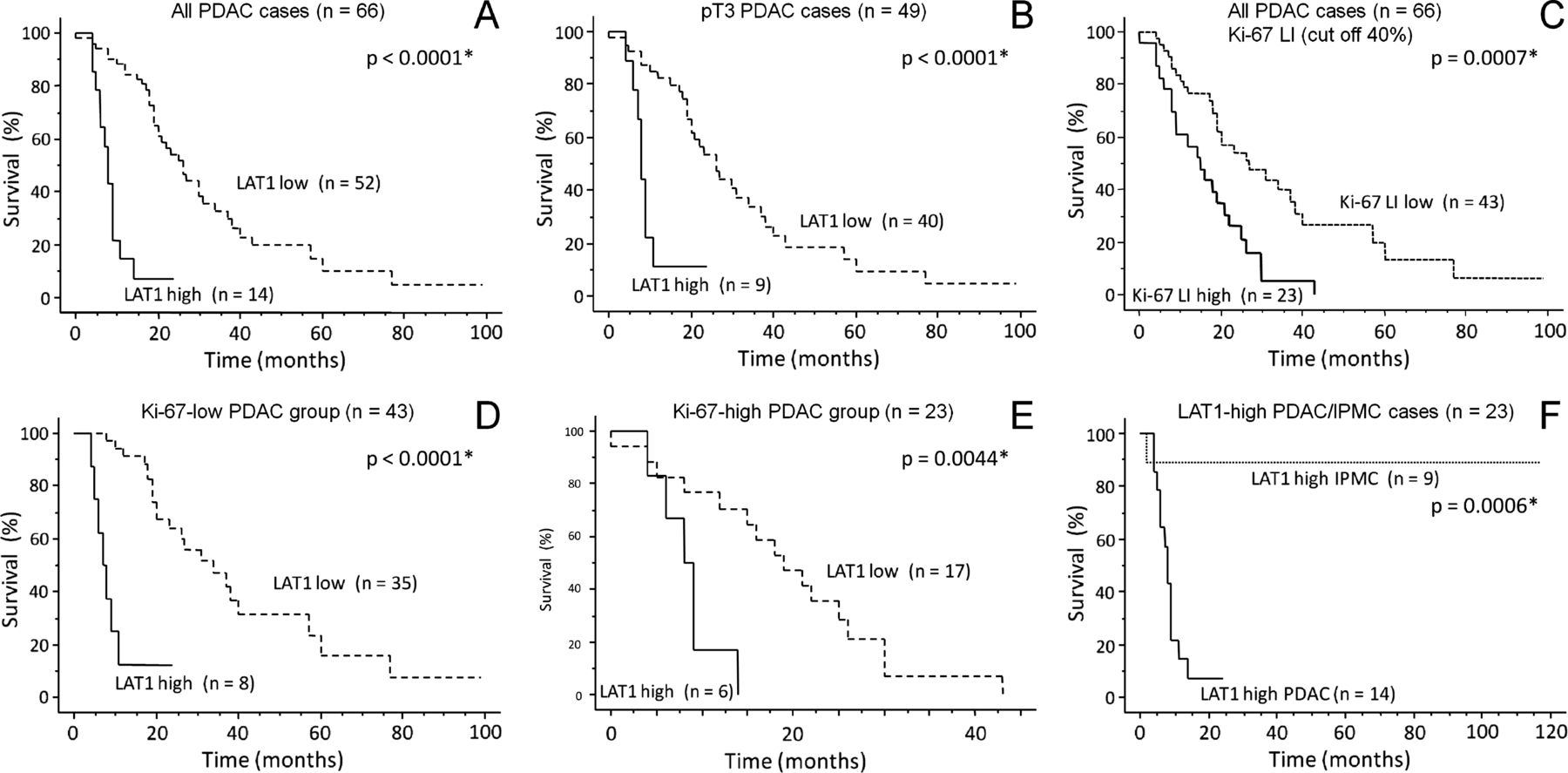
The follow-up period of 79 carcinoma cases after surgery was 24.9±22.4 months (range 0–117). According to the LAT1 scores (average 3.3), PDAC were divided into two groups, 52 cases as low (0–4) and 14 as high (6–9). Kaplan–Meier analysis produced a significant difference between LAT1 high and low scores in all PDAC (p<0.0001, figure 3A). Furthermore, the LAT1-high PDAC group also showed statistically significant poorer prognosis when cases were limited in the pT3 stages (n=49, p<0.0001, figure 3B). On the other hand, the high (≥40%, 23 cases) Ki-67-LI group of PDAC had statistically significant poorer survival than did the low group (43 cases) (p=0.0007, figure 3C). Thus, we also analysed the correlation between LAT1 expression and prognosis in each Ki-67-LI PDAC group. Even in each Ki-67-LI PDAC group, high LAT1 scores were related to poor prognosis (p<0.0001, figure 3D; p=0.0044, figure 3E). Similarly, in each group divided by other significant prognostic factors, such as tumour differentiation (well and moderately differentiated, p<0.0001), size (< 3 cm, p=0.0006; ≥3 cm, p=0.0001) and surgical margin status (negative, p<0.0001; positive, p=0.0081), high LAT1 expression could also predict poor prognosis using the log-rank test. Finally, LAT1-high PDAC (14 cases) showed significantly poorer prognosis than LAT1-high IPMC (9 cases) (p=0.0006, figure 3F).
{kind=link}
{kind=link}
{kind=link}
Cause-specific postoperative survival for patients with pancreatic ductal adenocarcinoma (PDAC) categorised by L-type amino acid transporter 1 (LAT1) expression. (A) overall survival curves of PDAC cases divided by the LAT1 score. (B) survival curve of PDAC cases limited to pT3 stage. (C) overall survival of PDAC divided by Ki-67 labelling index (cut off 40%). The Ki-67-high (≥40%) PDAC group showed a significantly poorer prognosis than did the Ki-67-low group (<40%). (D) Ki-67-low (<40%) PDAC group (n=43) and (E) Ki-67-high (≥40%) PDAC group (n=23) divided by LAT1 score. In all log-rank tests, the LAT1-high (score 6–9) groups showed significantly poorer outcomes than did the LAT1-low (score 0–4) groups. (F) Survival curve of LAT1-high PDAC and intraductal papillary mucinous carcinoma (IPMC) cases. LAT1-high PDAC showed a significantly poorer prognosis than did LAT1-high IPMC. *Indicates a significant difference.
Cox hazard analyses of postoperative cause-specific survival
For PDAC, tumour differentiation and maximum diameter, LAT1 expression, Ki-67 LI, surgical margin status (pancreatic or retroperitoneal margin) and pT stage were judged as prognostic factors using univariable analysis (table 1). Subsequently, multivariable analysis revealed that tumour differentiation, LAT1 expression, Ki-67 LI and maximum diameter were significant individual prognostic factors (table 1).
Cox hazard analyses of cause-specific survival in surgically treated pancreatic ductal adenocarcinomas (n=66)
Discussion
LAT1 has been reported to be expressed in cell membranes of cancer cells of many organs,3–7 ,13 being thought to actively take up some essential amino acids. In contrast, many normal cells ubiquitously express LAT2, the second system L isoform.14 LAT1 transports both large and small neutral amino acids, which is partially different from the LAT2 function. With immunohistochemistry using our monoclonal antibody of LAT1,4 we found that the high-LAT1 expression cases of PDAC showed poor prognosis (figure 3), in line with other cancers.4 ,6 Recently, some LAT1 inhibitors actually demonstrated growth inhibition against cancer cell lines. KYT-0353, one of the LAT1 inhibitors, showed significant growth inhibitory effects on human colon cancer cells both in vitro and in vivo.15 Inhibition of LAT1 by 2-aminobicyclo-(2,2,1)-heptane-2-carboxylic acid reduced cell viability in lung cancer cells.16 Therefore, LAT1 inhibitors might be useful as a new cancer chemotherapy, especially against high-LAT1 expression cases.
Prognostic factors of PDAC have been reported, such as tumour size, lymph node metastasis and surgical margin status.17 Previous report demonstrated that Ki-67 expression in pancreatic cancer was the most important determinant of long-term survival.18 Additionally, we found tumour differentiation and LAT1 expression were thought to be individual prognostic factors (table 1). We also confirmed that LAT1 overexpression was related to poor prognosis in each group divided by tumour differentiation, size and surgical margin status. In addition, p53 overexpression, p16 mutation or hypermethylation, loss of p27 protein expression, growth factors such as vascular endothelial growth factor or vascular endothelial growth factor receptor, and human epidermal growth factor receptor 2 overexpression have also been reported to be correlated with decreased survival in pancreatic cancer.19 ,20 Although we did not examine these molecular markers, we propose LAT1 as a new prognostic factor.
Contrary to our expectations, we could not find a significant correlation between LAT1 expression and Ki-67 LI. In contrast, some authors have demonstrated significant correlations between those factors in lung and gastric cancers.6 ,7 ,21 It is generally thought that proliferating cells require many amino acids. However, the double immunostaining of LAT1 and Ki-67 did not always show co-expression in the same tumour cells (figure 1E), which was consistent with our statistical analysis. In addition, we pointed out the correlation between LAT1 expression and prognosis in each Ki-67-low and -high PDAC group. Furthermore, even benign IPMA showing very low Ki-67 LI expressed LAT1 as did PDAC. These data suggested that there seemed to be no direct correlation between LAT1 expression and proliferative activity. Although it is difficult to discuss the discrepancy with the histological analysis, our results indicate that LAT1 expression in PDAC cases could be a new prognostic marker independent of Ki-67 LI.
In conclusion, we propose that elevated LAT1 expression in PDAC is a novel biomarker for high-grade malignancy independent of Ki-67 LI. Some LAT1 inhibitors have demonstrated repression of cancer cell proliferation. Therefore, inhibition of LAT1 function could be a potential therapeutic strategy for pancreatic cancer and other human cancers.
Take-home message
LAT1 expression is useful as a significant prognostic marker independent of the Ki-67 labelling index in pancreatic ductal carcinoma.
References
Footnotes
-
Contributors NY participated in the study design, evaluated immunoreactivity, performed statistical analyses, and wrote the manuscript. MI, TM and NN advised about the evaluation of immunoreactivity. KH performed laboratory work. WK provided the clinical information. HE supplied the antibody for immunohistochemistry. IO supervised the study design and evaluated immunoreactivity.
-
Funding This study was partly supported by a Grant-in-Aid from the New Energy and Industrial Technology Development Organization, Ministry of Economy, Trade and Industry, Japan.
-
Ethics approval Tissue samples were used with written informed consent of the patients. The study was approved by the Kitasato University School of Medicine and Kitasato University Hospital Ethics Committee.
-
Provenance and peer review Not commissioned; externally peer reviewed.