Article Text

Abstract
Objective: To review (1) the epidemiological literature on physical activity and the risk of breast cancer, examining the effect of the different parameters of activity and effect modification within different population subgroups; and (2) the biological mechanisms whereby physical activity may influence the risk of breast cancer.
Methods: A review of all published literature to September 2007 was conducted using online databases; 34 case-control and 28 cohort studies were included. The impact of the different parameters of physical activity on the association between activity and the risk of breast cancer was examined by considering the type of activity performed, the timing of activity over the life course and the intensity of activity. Effect modification of this association by menopausal status, body mass index (BMI), racial group, family history of breast cancer, hormone receptor status, energy intake and parity were also considered.
Results: Evidence for a risk reduction associated with increased physical activity was found in 47 (76%) of 62 studies included in this review with an average risk decrease of 25–30%. A dose-response effect existed in 28 of 33 studies. Stronger decreases in risk were observed for recreational activity, lifetime or later life activity, vigorous activity, among postmenopausal women, women with normal BMI, non-white racial groups, those with hormone receptor negative tumours, women without a family history of breast cancer and parous women.
Conclusions: The effect of physical activity on the risk of breast cancer is stronger in specific population subgroups and for certain parameters of activity that need to be further explored in future intervention trials.
Statistics from Altmetric.com
The aetiological role of physical activity in breast cancer is now becoming increasingly convincing and over 80 studies have been conducted worldwide that have examined some aspect of this association. Given the large number of studies that have been conducted, it is now possible to examine the effect of physical activity among subgroups of the population that have not previously been considered in other reviews of this topic.1–3 The effect of physical activity may differ within these subgroups and, hence, the public health recommendations could vary depending on the population at risk. The objectives of this paper are:
to examine the impact of activity on the risk of breast cancer according to the dose, type and timing of activity;
to examine the impact of physical activity on the risk of breast cancer within different population subgroups; and
to discuss possible hypotheses regarding the underlying biological mechanisms that may be operative between physical activity and breast cancer risk.
METHODS
A review of the epidemiological literature on physical activity and the risk of breast cancer was conducted by searching PubMed, Medline, Embase, CINAHL, BIOSIS Previews to September 2007 using the following search terms: physical activity, exercise, lifestyle, fitness, daily activity and breast cancer, breast neoplasms, breast tumour in studies done in humans with these words found in either the title or abstract. All articles published in any language were considered. To be eligible, some measure of physical activity needed to be examined with breast cancer as the main outcome of the study. Multiple publications from the same study were found and criteria were established for selecting the most appropriate paper to be included in this review. For cohort studies the most recent publication from the cohort was chosen, and for case-control studies the original publication with the main results from the study was selected.
Tables were created of the design characteristics of the studies including study sampling methods, method of physical activity assessment, results, type of control for confounding and any subgroup analyses examined. The main result from each study was selected and graphs of each of the comparisons considered were plotted. Additional graphs were created that presented the results of these studies by type, intensity and time of activity. All studies that examined the results within subgroups of the study population were identified and those results were extracted into separate tables and graphs for presentation. The subgroups considered were: menopausal status, body mass index (BMI), lifetime weight gain, racial/ethnic group, parity, hormone receptor status, family history of breast cancer, and total caloric and alcohol intakes. If five or more studies were found that had examined the effects within the same subgroups, the results were included for presentation here. The average risk reductions were estimated as the mean of the point estimates.
A literature review of the main biological mechanisms that could explain how physical activity influences the risk of breast cancer was also conducted to complement the epidemiological review presented here.
RESULTS
A total of 87 papers were found that met all the criteria specified and, of these, 28 cohort studies4–31 and 34 case-control studies1 32–63 were included in the review. The 25 studies not included were either studies that were updated later by other authors,64–76 included male breast cancers,77 78 did not provide point estimates with confidence intervals,79 80 used a different study design,81 had problems with the study methods or analysis,82–86 was a less appropriate re-analysis of other studies already included87 or was very similar to another publication on the same study.88 The analysis of Enger et al74 of the study by Bernstein et al33 was included only in the population subgroup section since it provided stratified results on hormone receptor status that were considered in this review.
Overall associations
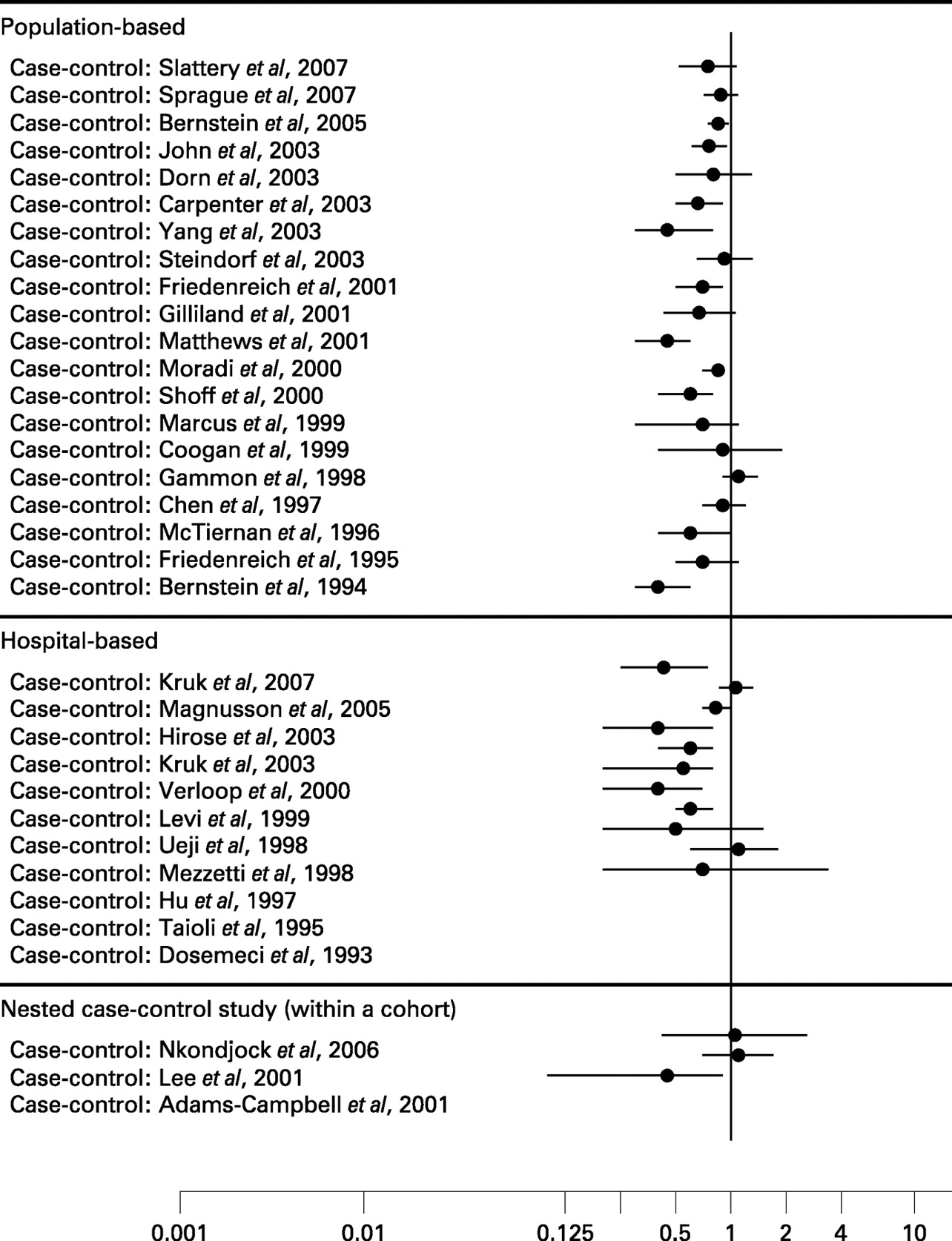
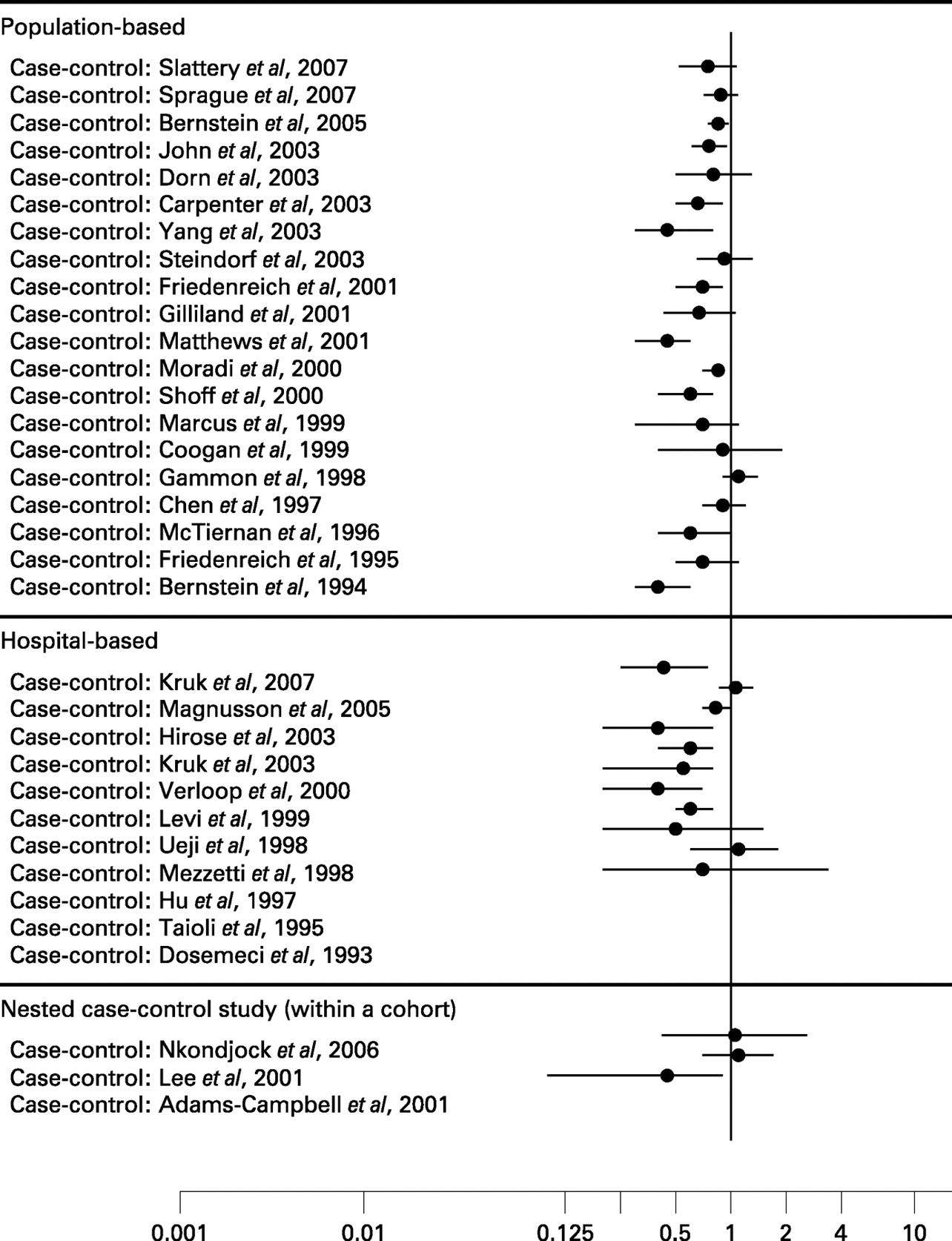
Thirty of the 62 studies included in this review found a statistically significant risk reduction among the most physically active women compared with the least physically active within their study populations.5 6 8–11 16 17 19 22 31 33 35–38 40–43 47 48 50 52 53 56 57 59 62 63 An additional 9 studies had a borderline statistically significant risk reduction,12 15 21 27–29 55–57 8 had a non-statistically significant reduction14 20 30 38 51 54 61 89 and 14 studies7 13 18 23–26 32 34 44 46 49 58 60 observed no effect of physical activity on the risk of breast cancer. Only one study4 reported an increased breast cancer risk for the most physically active and the risk was not statistically significant. Overall, there was a 25% risk reduction for all studies combined with a stronger decrease found in the case-control studies (average 30%) than in cohort studies (average 20%). For the 47 studies observing a risk reduction, regardless of the statistical significance of the reduction, the magnitude of the decrease was about 36%. Evidence for a dose-response relation was found in 286 8–12 15 19 21 27 31 33 35–37 40 41 43 45 47 48 50 53–55 59 62 63 of 34 studies6 8–12 15 16 19 21 27–29 31 33 35–38 40 41 43 45 47 48 50 53–56 59 62 63 89 that reported a decreased risk of breast cancer associated with physical activity.
These risk reductions were reported more frequently in the case-control studies than in the cohort studies (figs 1 and 2) since 18 of the 28 cohort studies (64%) and 24 of the 34 case-control studies (71%) reported risk decreases. Likewise, evidence for a dose-response effect was observed somewhat more often for the case-control studies with 16 of the 34 (47%) case-control studies and 11 of the 28 (39%) cohort studies finding evidence for decreasing risk with increasing activity levels.

Type, dose and timing of activity
A wide range of physical activity assessment methods were used to assess the type, dose and timing of activity. Hence, to evaluate whether or not specific components of physical activity are associated with greater risk reductions for breast cancer, these parameters of activity were examined separately.
Type of physical activity
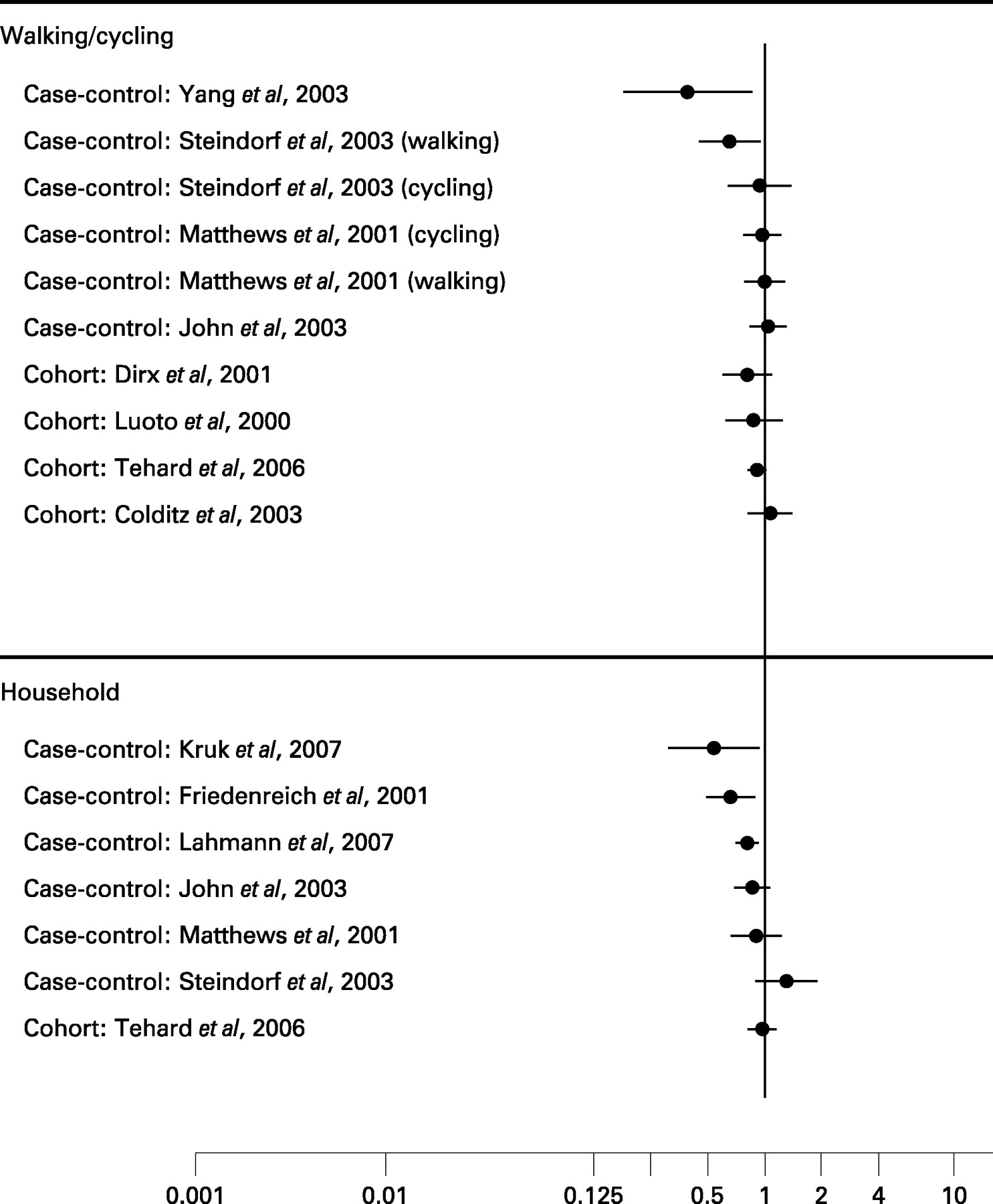
The first parameter examined was the type of physical activity: occupational, household, recreational (also sometimes referred to as leisure activity) and transportation to and from work (usually walking/cycling) (figs 3–5). Of these four types of activities, the greatest risk decreases were found for recreational activity (average 20% decrease), followed by walking/cycling for transportation (14%), household (14%) and occupational activity (13% decrease).



Dose of physical activity
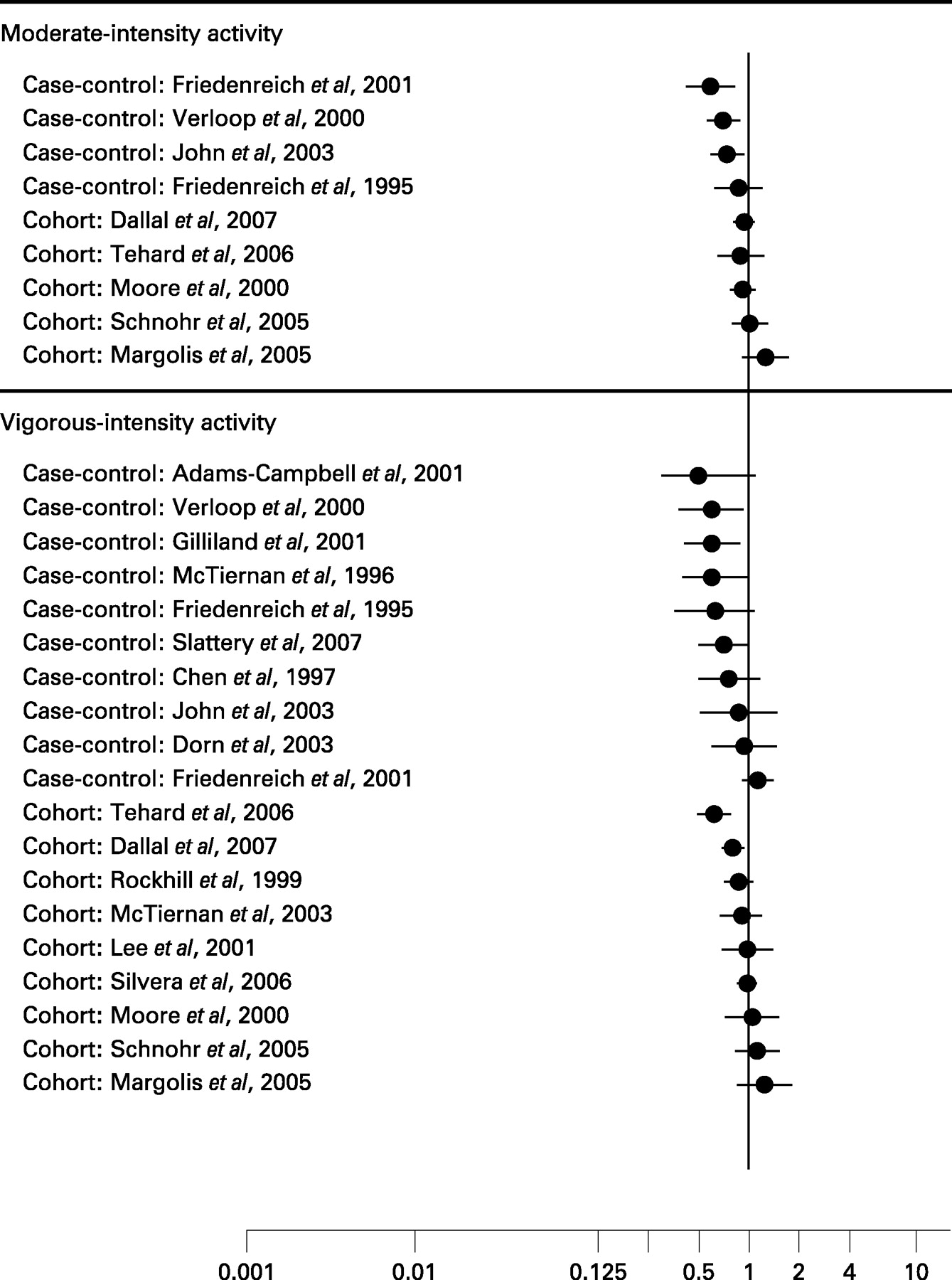
The dose of activity includes the frequency, duration and intensity of activity performed. Since several studies did not measure the frequency and duration of activity, the most easily comparable component of dose is the intensity at which it was performed. Risk reductions were observed with moderate intensity activity (average decrease 22%); however, even greater risk decreases were found when vigorous intensity activity was performed (average 26%) (fig 6).

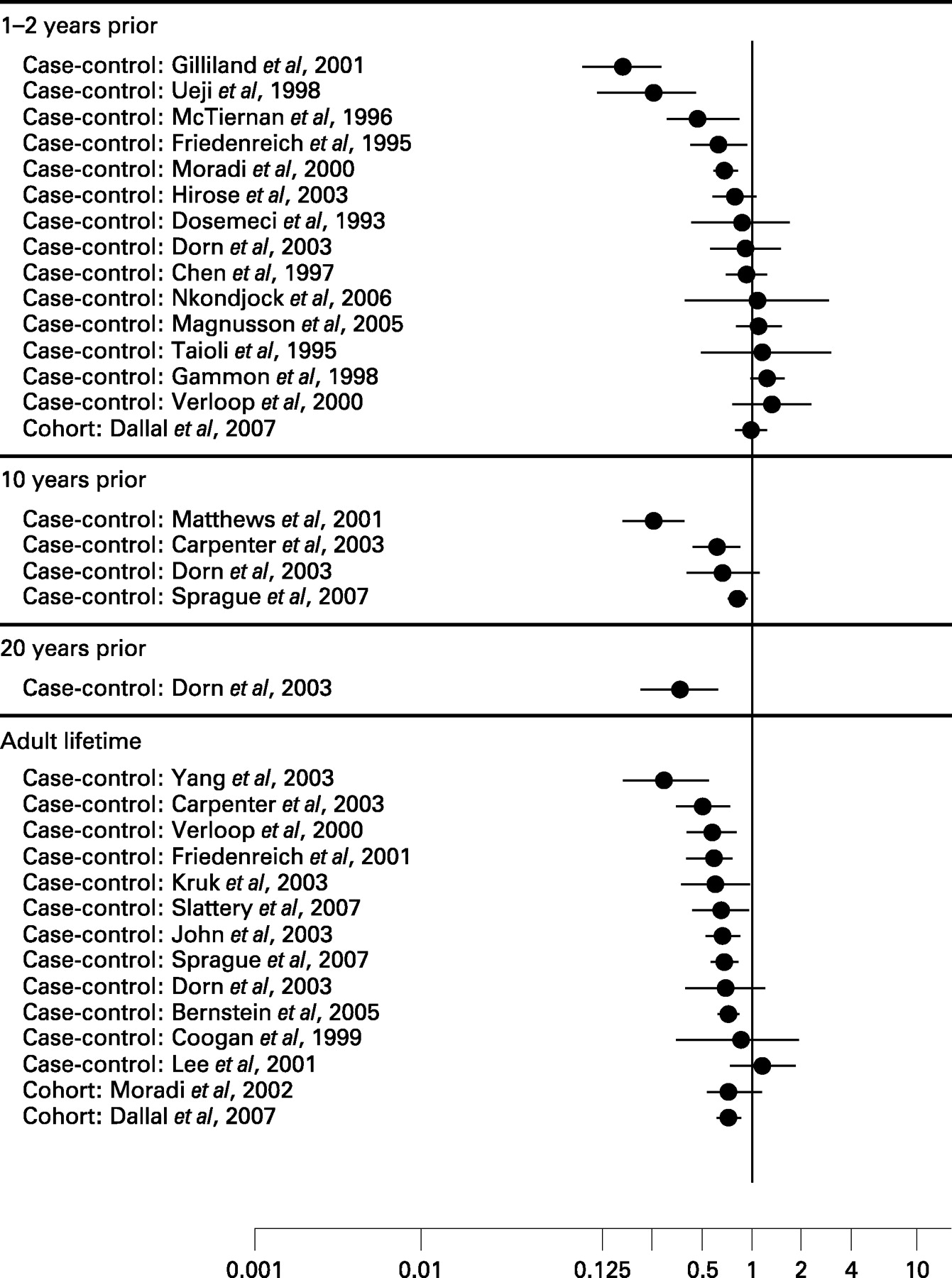
Timing of physical activity
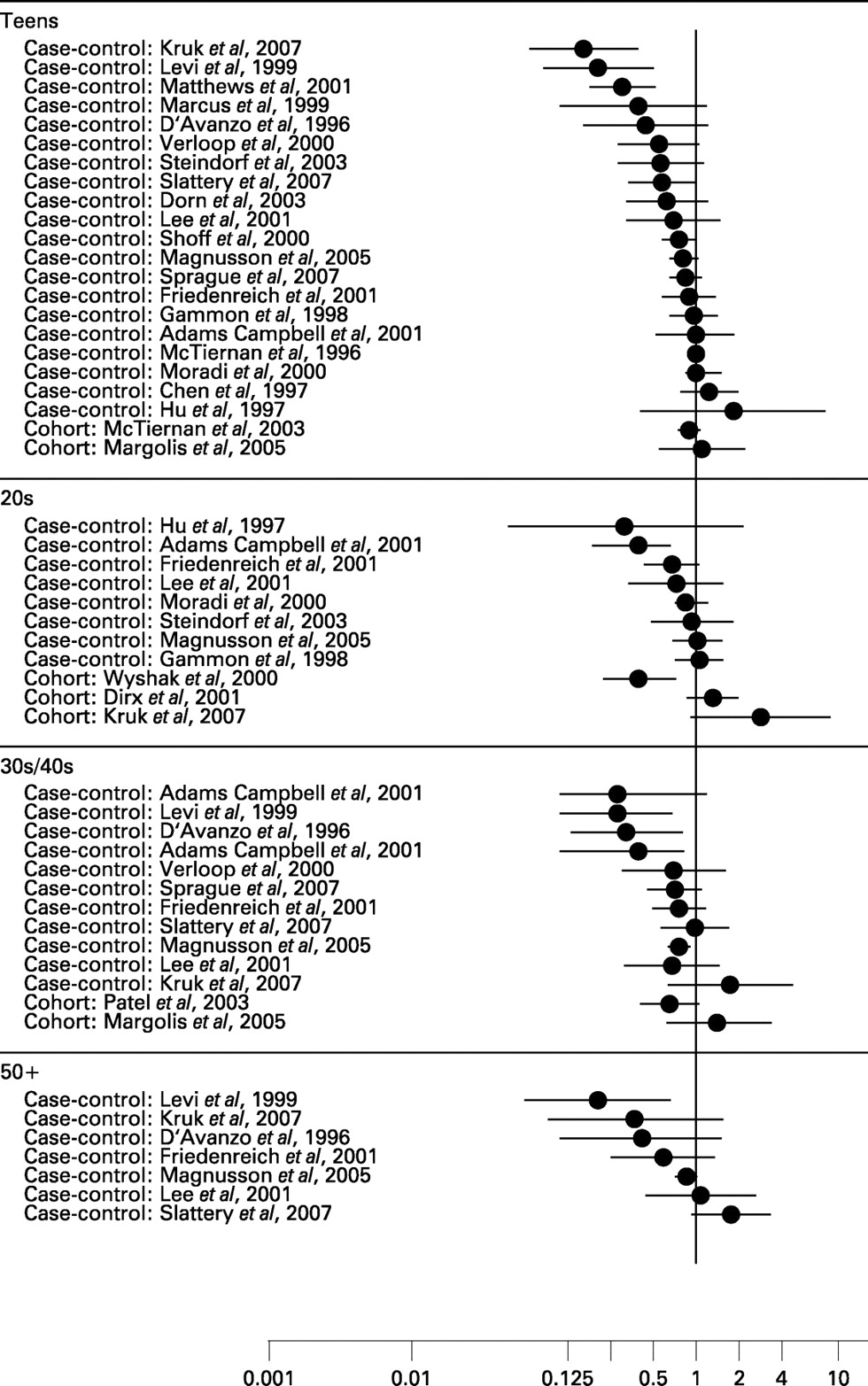
The third dimension of physical activity considered was the timing in life when the activity was performed. It was possible to categorise these studies into two main groups: those that examined the timing of activity relative to the development of breast cancer (1–2 years, 10 years or 20 years before diagnosis or full adult lifetime; fig 7) or as activity done during specific ages in life (adolescence, early adulthood (20s), middle adulthood (30–40s), later adulthood (⩾50 years); fig 8). Risk reductions were observed for activity performed at all life and age periods; however, measurements of lifetime activity were more consistently associated with a decreased risk of breast cancer than were measurements of more recent activity around the time of diagnosis. There was also a tendency for activity done after age 50 to have a stronger effect on breast cancer risk reduction than activity performed early in life (adolescence and early adulthood).

Population subgroups
Effect modification by personal characteristics was also considered by examining the risks within study population subgroups defined by menopausal status, BMI, racial/ethnic group, family history of breast cancer, hormone receptor status, parity and by other lifestyle factors including energy intake level and alcohol intake. A few studies also examined effect modification by other factors including tumour type (ie, in situ versus invasive);21 31 61 other menstrual and reproductive factors;58 exogenous hormone use;21 58 62 adult weight gain;11 21 41 alcohol intake;21 48 58 smoking habits;48 migration50 and socioeconomic status.58 However, since fewer than five studies had examined these factors, these subgroup comparisons are not presented in this review.
Menopausal status
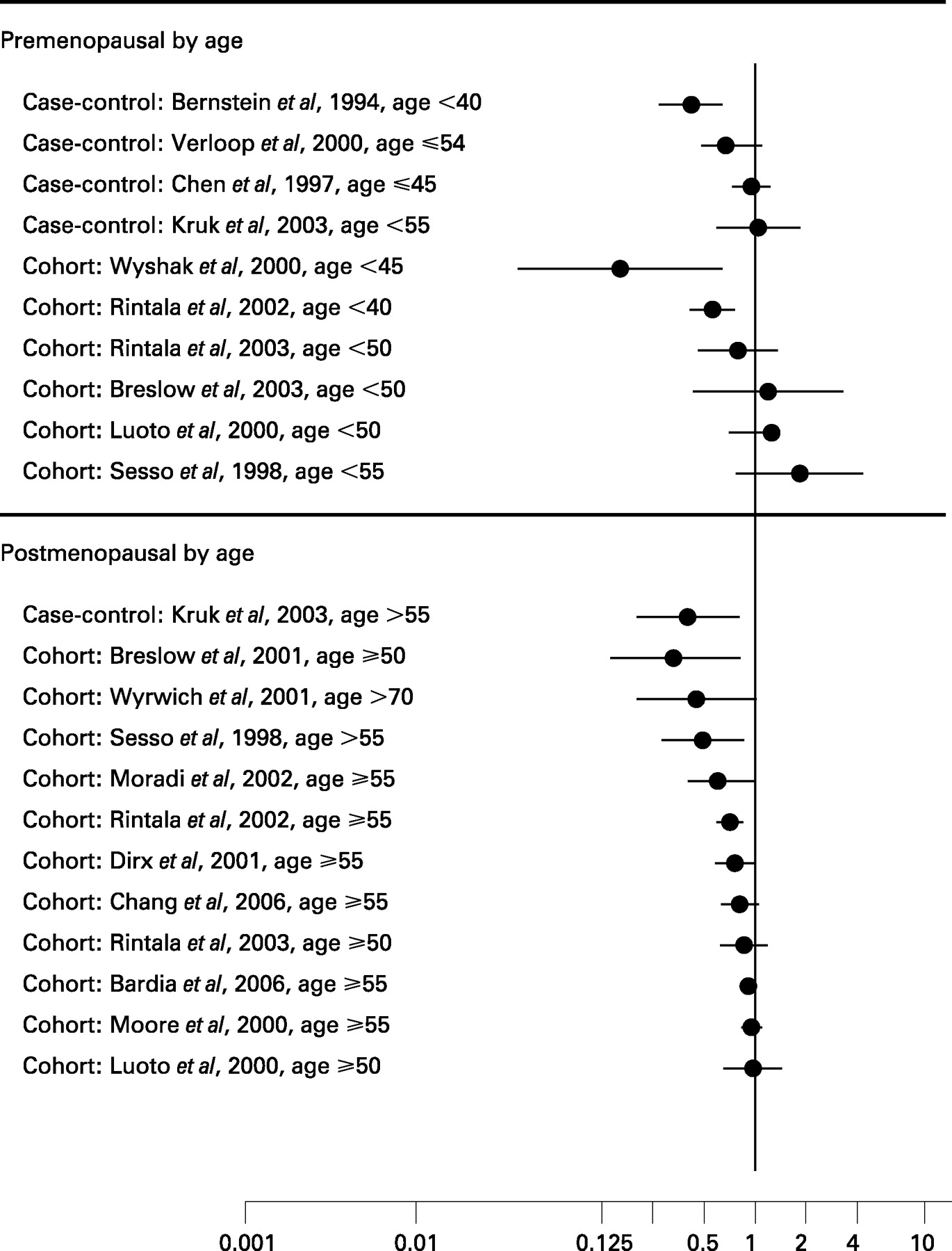
The first major population subgroup considered, menopausal status, was examined in two different ways in this review. First, for those studies that provided the results stratified by menopausal status (fig 9), the results are presented for pre- and postmenopausal women separately. An effect of physical activity on breast cancer risk is evident in both pre- and postmenopausal women, but the risk reductions are greater in magnitude and more studies observed a risk reduction in postmenopausal women than in premenopausal women. Of the 43 studies that presented results for either pre- and/or postmenopausal women, 31 studies included premenopausal women and 35 included postmenopausal women. Five of the 31 studies of premenopausal women had statistically significant risk reductions,17 22 33 42 50 14 had non-significant risk reductions,6 20 25 30 35 36 43 47 51 54 56 57 62 63 and the average risk decrease was 40%; 20 of the 35 studies that included postmenopausal women observed statistically significant decreases in risk9–12 16 19 21 22 30 36 40 41 43 45 47 48 50 53 55 63 90 and 10 had non-statistically significant reductions;6 14 20 29 35 54 56 57 62 89 the average risk decrease was 33%. Twenty-three studies presented results for both pre- and postmenopausal women in the same study population,1 6 9 10 13 20 22 26 30 35 36 43 45 47 48 50 51 54 56 57 62 63 89 14 of which observed a decreased risk in both pre- and postmenopausal women,6 20 22 30 35 36 43 47 50 54 56 57 62 63 in 10 the decrease was greater in premenopausal women6 20 22 30 35 50 54 56 57 62 and in 4 studies a greater decrease was observed in postmenopausal women.36 43 47 63 Only 2 studies observed statistically significant decreases in both pre- and postmenopausal women22 50 and 9 studies9 10 30 36 43 45 47 48 63 had a statistically significant decrease in one menopausal group only; for all of these 9 studies the effect was found in postmenopausal women only.

What is already known about this topic
Consistent and strong observational epidemiological evidence exists that physical activity reduces the risk of breast cancer with the evidence classified as “convincing”.
The magnitude of the risk reduction is about 25–30% and there is also evidence for a dose-response effect.
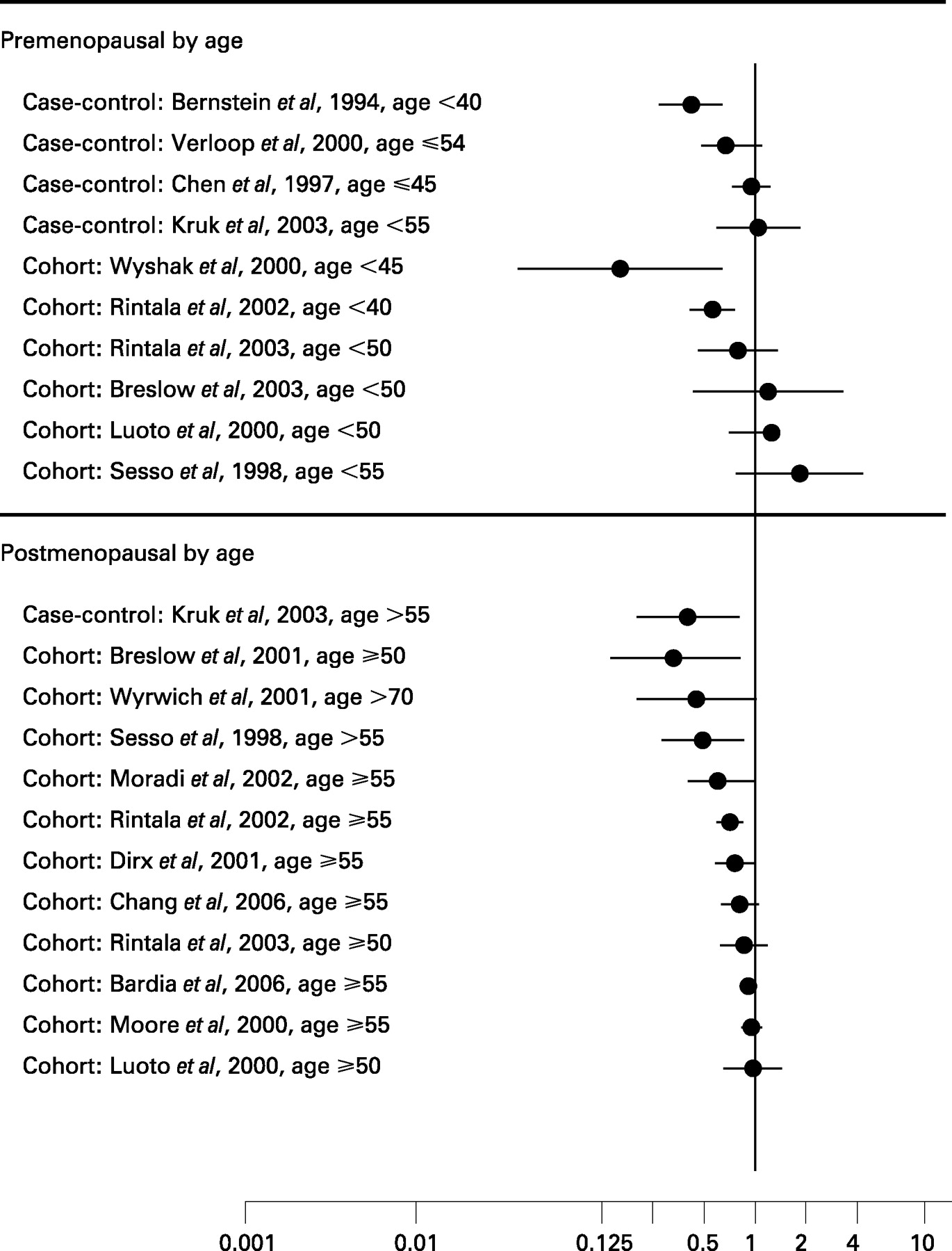
Several studies did not have menopausal status available for their study population but stratification on a proxy age for menopause (usually around age 50) was done (fig 10). Hence, for the 16 studies9–11 13 14 16 17 20 22 28 29 33 34 42 52 75 that used age at interview/diagnosis as a proxy for age at menopause, 10 presented data for women who were considered premenopausal by age. Of these studies, 5 found no effect of physical activity on breast cancer risk,9 10 13 34 52 2 reported a non-statistically significant decreased risk20 42 and 3 found a statistically significant decreased risk.17 22 33 In contrast, for the 12 studies of women determined to be postmenopausal by their provided age at interview/diagnosis, 11 showed either a statistically9–11 14 22 52 or non-statistically significant decreased risk16 20 28 29 75 and only 1 study had a null effect in the postmenopausal group.13
What this study adds
We have comprehensively examined all parameters of physical activity (duration, frequency, intensity), type of activity (occupational, household, recreational), time periods in life and possible effect modification that have not been thoroughly reviewed before.
Stronger risk decreases were found for recreational activity, lifetime or later life activity, vigorous activity, among postmenopausal women, women with normal body mass index, non-white racial groups, hormone receptor negative tumours, women without a family history of breast cancer and parous women.
Body mass index
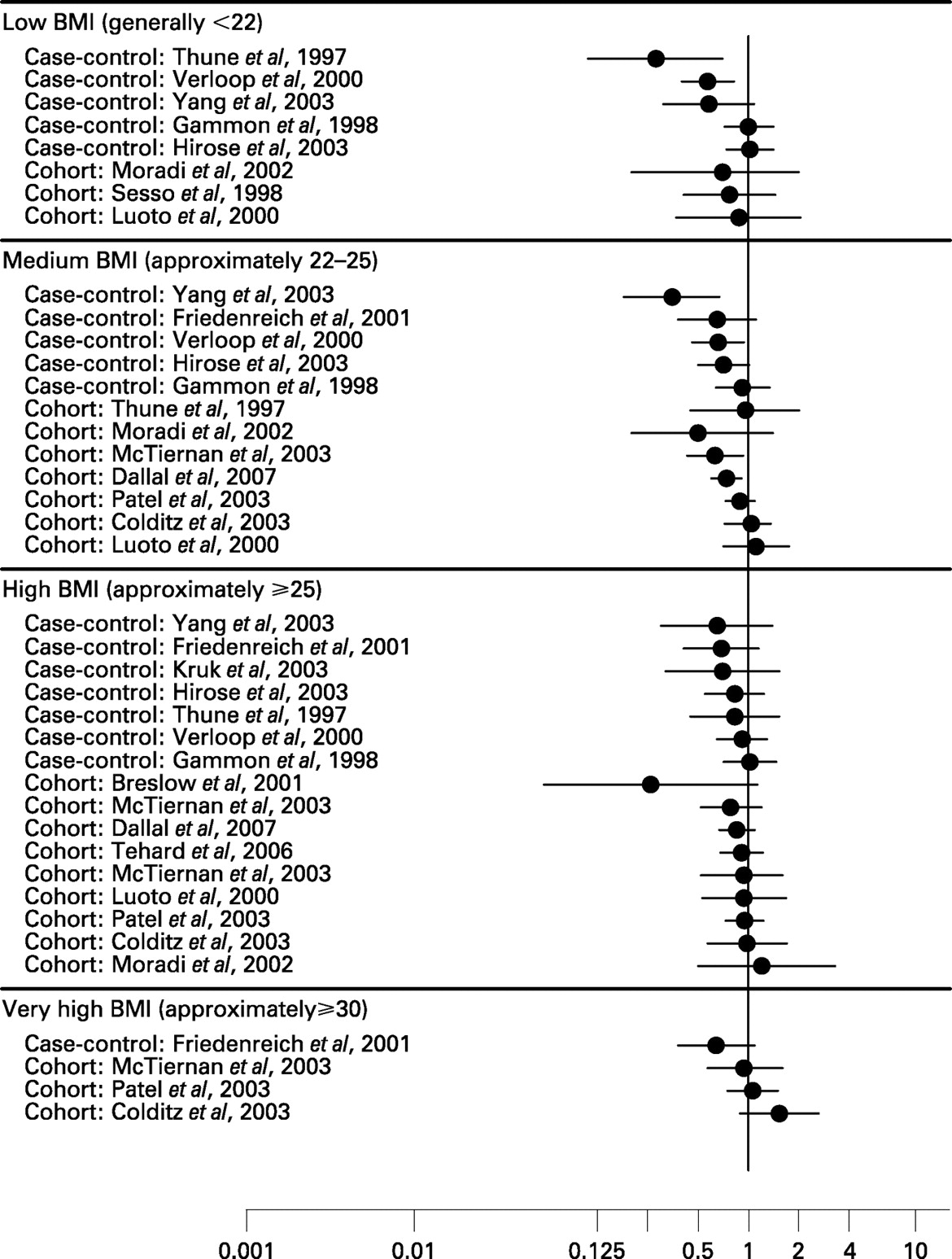
The second main effect modifier examined in 16 studies was BMI. The results could be divided into four groups: lean BMI (<22 kg/m2), normal BMI (22–25 kg/m2), high BMI (⩾25 kg/m2) and very high BMI (⩾30 kg/m2) (fig 11).1 6 9 10 13 14 18 19 21 27 31 42 48 50 52 56 A clear trend of decreasing breast cancer risk with decreasing BMI and increasing physical activity levels was observed across these studies. The average risk reductions were 0.73 for women with a lean BMI,1 6 9 13 14 42 50 56 0.76 for women with a normal BMI,1 6 13 14 18 19 21 31 42 48 50 56 0.81 for women with a high BMI1 6 10 13 14 18 19 21 27 31 42 48 50 52 56 and 1.04 for women with a very high BMI.18 19 21 48
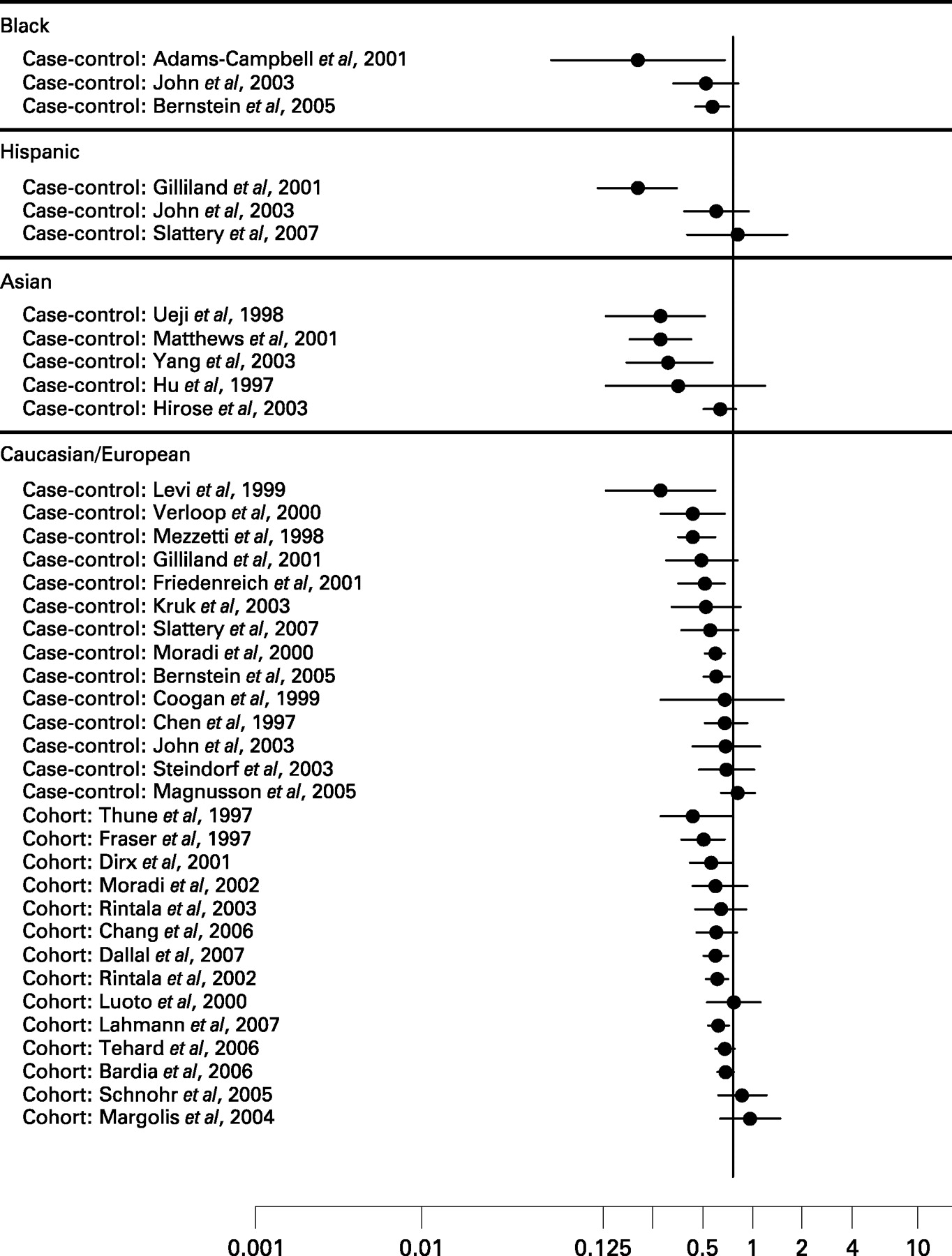
Racial group
Only four studies included separate risk estimates for the association between physical activity and breast cancer risk by racial group;45 57 59 62 however, most of the studies could be classified according to the main racial/ethnic group of their study population (fig 12). For the three studies that included black women,43 57 59 all found reduced breast cancer risks that were on average a 40% relative decrease, and two43 59 of the three studies had statistically significant risk reductions. The effect of physical activity was less evident in the Hispanic populations with only one45 of three studies45 57 62 finding a statistically significant risk reduction with an average reduction of 30%. The five studies that included Asian women35 47 50 56 89 showed the strongest risk decreases of all racial groups that averaged 50% with four studies finding either statistically significant35 47 50 or borderline significant risk reductions.56 Caucasian populations were represented in 29 studies and had an average risk decrease of 26% in the most physically active women compared with the least active women, and half (13 of the 29 studies) had statistically significant associations.5 6 11 22 30 31 36 37 40 42 48 59 81
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Family history of breast cancer
The potential effect modification of the association between physical activity and breast cancer by family history of breast cancer was presented in six separate studies,31 53 56 58 59 61 and some additional studies noted that they found no difference in their study populations by family history and did not provide the data.27 48 A greater risk reduction was observed for women without a family history of breast cancer (average risk reduction 0.94) than for those who did have such a history (average risk 1.2).
Hormone receptor status
A few studies12 29 31 59 74 have examined the influence of hormone receptor status on the association of physical activity with breast cancer. The only common comparison possible for this review was oestrogen and progesterone positive (ER+/PR+) and negative tumours (ER−/PR−). There appeared to be a greater risk reduction for the negative hormone receptor tumours (average risk reduction 0.61) than for the positive tumours (0.86).
Energy intake level
Lowest versus highest quantile of energy intake was also considered as a possible effect modifier in five studies.1 11 21 25 50 No differences were observed in the magnitude of the risk reduction in these studies for low versus high consumers of total energy, with a 21% average decrease in both groups.
Parity
Parity was examined in six studies as a potential effect modifier of the association between physical activity and the risk of breast cancer,27 31 33 40 48 58 and a slightly greater risk reduction was found for parous women (average risk decrease 28%) than for nulliparous women (average risk decrease 22%).
DISCUSSION
This review found a decrease in the risk of breast cancer of approximately 25% among the most physically active women compared with the least active women in over two-thirds of the studies and a dose-response effect in nearly half of the studies considered here. All types of activity were associated with a reduction in the risk of breast cancer, but recreational activity was somewhat more strongly associated than were occupational or household activities. Both moderate and vigorous intensity activity conferred a nearly equal benefit for a decrease in breast cancer risk. Activity done throughout lifetime had the greatest impact on the risk of breast cancer, as did activity performed after menopause; however, activity done in early and mid-life was also shown to decrease the risk in some studies. Physical activity reduced the risk for breast cancer among all categories of BMI except obese women, and a clear dose-response in the magnitude of the benefit was found with the greatest risk decreases for lean women (BMI <22 kg/m2). Having no family history of breast cancer, being parous, and oestrogen and receptor hormone negative also resulted in slightly larger risk reductions, although few studies examined these subgroups. The one factor that did not appear to modify the effect of physical activity on the risk of breast cancer was total caloric intake. It should be noted that some of the effect modification considered here did not reach statistical significance because of the small sample sizes within the population subgroups examined. Larger studies that plan to examine some of these possible effect modifiers prospectively would permit more definitive conclusions to be made regarding these possible subgroup effects.
Clarifying the precise biological mechanisms through which physical activity exerts a protective effect on the risk of breast cancer is challenging, partly because of difficulties in measuring physical activity precisely and also because the biological mechanisms may differ according to the dose (eg, intensity, duration) and timing of the activity. A further limitation in determining these mechanisms is that there are currently no suitable biomarkers of exposure or biologically effective dose of physical activity.91 Despite these methodological issues, epidemiological and experimental studies have provided some evidence for several hypotheses of biological pathways through which physical activity may reduce the risk of breast cancer.2 92–94 The proposed mechanisms can be broadly categorised into:
reduction in circulating levels of and cumulative exposure to sex steroid hormones;
changes to insulin-related factors and adipocytokines;
modulation of inflammation and the immune system; and
hormonal and cellular metabolism pathways.
Breast cancer has a complex aetiology and these diverse mechanisms could interact with different stages of carcinogenesis, including DNA damage, initiation, promotion and progression, and manifestation of clinical disease.4 91 Moreover, it is likely that no one mechanism is responsible for the reduced risk of breast cancer, and thus these mechanisms may act in combination. It is also possible that the underlying biological mechanisms may differ depending on the population subgroup(s), as presented above (eg, in premenopausal versus postmenopausal women).
Reduction in circulating levels of and cumulative exposure to sex steroid hormones
It is well established that oestrogens are implicated in breast tumour development and growth by stimulating mitosis of breast epithelial cells and regulation of cell cycle progression.95–99 Progesterone and androgens in both pre- and postmenopausal women may also be implicated in breast tumour development, although the evidence for these hormones is less consistent.96 97 100 101 Androgens may have direct effects on breast tissue in addition to providing additional substrate for conversion into oestrogens.100 101
Several studies have shown that physical activity is inversely associated with total and bioavailable oestrogen levels.102–106 There are two main pathways through which physical activity could reduce exposure to oestrogens and other endogenous hormones. First, physical activity helps to maintain energy balance and reduce body fat. Observational and intervention studies in postmenopausal women indicate that the inverse association between physical activity and oestrogen levels is partly attributable to decreased BMI.102 107 Reduced adipose tissue is likely to have a stronger effect on breast cancer risk in women who are postmenopausal than premenopausal because, after the menopause when the ovaries no longer produce oestrogens and progesterone, the conversion of androgens to oestrogens by the aromatase enzyme in adipose tissue becomes the primary source of endogenous oestrogens.108 109
In contrast to postmenopausal women, obesity appears to confer a slight protection to breast cancer during the reproductive years.110 The protective effect of obesity in premenopausal women is thought to be attributable to decreased oestradiol and progesterone levels associated with obesity-related menstrual cycle disruptions.110 Nevertheless, obesity appears to be associated with advanced disease at diagnosis and a poor prognosis in both pre- and postmenopausal women,111 so physical activity could possibly reduce breast tumour progression in both groups of women.
The second pathway by which regular moderate (and especially vigorous) intensity physical activity could reduce circulating endogenous hormone levels and cumulative hormone exposure is through alterations to menstrual function and patterns, especially when combined with reduced energy intake.112 113 Possible activity-induced changes to menstrual function include delayed onset of menarche, irregular or absent menstrual periods, abnormal luteal function, loss of the surge in luteinising hormone and a longer menstrual cycle length.105 112 114–120 Similarly, excess weight is also associated with both early menarche and delayed menopause,64 121 so physical activity could also act through this pathway by reducing body fat.
Changes to insulin-related factors and adipocytokines
Physical activity is associated with improved insulin sensitivity,122 123 lower fasting insulin levels,124–126 increased levels of sex hormone binding globulin (SHBG)127 and insulin-like growth factor (IGF) binding protein-I.124 128 129 While vigorous and moderate intensity activities are thought to have the largest impact on insulin sensitivity, even light intensity physical activity that has been objectively measured has been shown to be associated with reduced 2 h post-challenge plasma glucose levels independently of higher intensity physical activity and other confounders, whereas sedentary behaviour was positively associated with 2 h glucose levels.130
Glucose has been shown to stimulate the proliferation of cultured breast cancer cells.131 Insulin is thought to play a role in breast cancer development as it can indirectly increase bioavailable oestrogen and androgen levels by downregulating SHBG and upregulating ovarian sex steroid production.128 Insulin also increases the synthesis and bioactivity of IGF-I, and both insulin and IGF-I may act directly as mitogenic and anti-apoptotic growth factors on normal and malignant breast tissue.98 128 132 High insulin levels may also be related to breast tumour aggressiveness.133 The insulin/IGF-I pathway and leptin may also interact with oestrogen to increase transcriptional activity synergistically or to promote cell cycle progression in breast epithelial cells.98 134
Compared with in vitro studies, the epidemiological evidence for an association between insulin, glucose and breast cancer risk is less compelling as most previous prospective studies have found no strong association.135–140 However, a recent meta-analysis of studies examining type 2 diabetes and breast cancer risk suggests a modest (20%) increased risk.141
There is increasing evidence that the adipocytokines leptin and adiponectin may be involved in breast cancer development. Leptin, which is highly correlated with body fat mass, plays a key role in regulating energy intake and metabolism and has been shown to stimulate breast cancer growth.98 142 143 Leptin could increase proliferation of breast epithelial cells through activation of cellular signalling pathways, by promoting angiogenesis, or by increasing the synthesis of oestrogens in breast tissue through enhanced expression of the aromatase enzyme.98 142–146 Conversely, adiponectin is hypothesised to have inhibitory effects on breast cancer tissue through several possible pathways including insulin sensitisation, antiproliferative and apoptotic activity, and possibly modulation of levels of proinflammatory cytokines and other hormones.98 143 146–150 Findings from some epidemiological studies support an inverse association of adiponectin with breast cancer,149 151–153 although the epidemiological evidence for a positive association with leptin is less convincing.154–156 As adipocytokines are produced in adipose tissue, physical activity could modify the levels of leptin and adiponectin by reducing fat mass. In addition, although the precise regulation of adiponectin levels remains unclear, some studies have reported that both acute and chronic physical activity may influence circulating adiponectin levels and expression of adiponectin receptors,157–159 although other studies reported no effect.160 161
Modulation of inflammation and the immune system
Physical activity may influence breast cancer risk and recurrence of breast cancer through modulation of inflammation and immune function.91 162 Physical activity can affect the balance of pro- and anti-inflammatory cytokines in the systemic circulation and local tissues.163 164 Although strenuous exercise induces an increase in the concentrations of proinflammatory cytokine concentrations, the body also appears to increase the expression of anti-inflammatory cytokines and cytokine inhibitors simultaneously as a compensatory mechanism.164–166 This balance of pro- and anti-inflammatory cytokines may depend on the characteristics of the activity, particularly the intensity.162–164 167 168 Long-term, moderate or vigorous physical activity may also enhance systemic natural immunity and cytotoxic mechanisms,91 92 169–171 although this effect may be tissue and immune cell-specific.169
Hormonal and cellular metabolism pathways and other mechanisms
It is hypothesised that physical activity could promote metabolism of oestrogen via the 2-hydroxylation pathway rather than the 16α-hydroxylation or 4-hydroxylation pathways. The latter pathways are considered more oestrogenic and possibly genotoxic, whereas the 2-hydroxylation pathway can promote apoptosis, anti-inflammatory actions and inhibition of tumour growth.162 172 173 However, despite body fat playing a role,162 174 epidemiological studies have not shown physical activity to alter this pathway.175 176
More recently, studies have highlighted the possible role of physical activity in activating various intracellular signaling pathways including 5′-AMP-activated protein kinase (AMPK), phosphoinositide 3-kinase (PI3-K), mitogen-activated protein kinases (MAPK) and NF-κB.170 177 178 These cellular pathways are implicated in breast cancer development and are involved, to different degrees, in regulating transcription, insulin resistance, growth and differentiation, apoptosis and inflammation.98 170 177 178 The extent of activation of these pathways by physical activity may depend on the intensity, duration and type of exercise.170
It has been suggested that physical activity may reduce breast cancer risk through changes in mammographic density, but this putative pathway is not supported by the epidemiological literature.179–198 Recent research has also considered whether or not physical activity may influence carcinogen-DNA adduct levels199 although, to date, there is little evidence of an association between carcinogen-DNA adducts and the aetiology of breast cancer.200
CONCLUSION
Further observational epidemiological research is needed to clarify the biological mechanisms underlying the association between physical activity and reduced breast cancer risk, especially with regard to the type, duration and intensity of activity and to explain differences in population subgroup effects. We can expect continuing advances in knowledge of these mechanisms as the field is moving forward with important developments in methods, including improvements in physical activity assessment,201 animal models,202 development of suitable biomarkers and incorporation of new technologies such as microarrays that can examine gene and protein expression changes in response to physical activity.91 In addition, completed203 204 and ongoing205 206 exercise intervention trials examining how physical activity influences these biological mechanisms are providing the most direct evidence to elucidate these associations.
REFERENCES
Footnotes
Funding: CF was supported by career awards from the Canadian Institutes of Health Research and the Alberta Heritage Foundation for Medical Research and AC received a Research Scholar Award from the Cancer Institute NSW, Australia while writing this review.
Competing interests: None declared.