Article Text

Abstract
Objective To assess the potential clinical and economic impact of introducing an electronic audit and feedback system into current practice to improve hand hygiene compliance in a hypothetical general hospital in England, to reduce the incidence of healthcare-associated infections (HCAIs).
Methods Decision analysis estimated the impact of introducing an electronic audit and feedback system into current practice to improve hand hygiene compliance among front-line healthcare practitioners (HCPs).
Results The model assumed 4.7% of adult inpatients (ie, ≥18 years of age) and 1.72% of front-line HCPs acquire a HCAI in current practice. The model estimated that if use of the electronic audit and feedback system could lead to a reduction in the incidence of HCAIs of between 5% and 25%, then the annual number of HCAIs avoided could range between 184 and 921 infections per hospital and HCAI-related mortality could range between 6 and 31 deaths per annum per hospital. Additionally, up to 86 days of absence among front-line HCPs could be avoided and up to 7794 hospital bed days could be released for alternative use. Accordingly, the total annual hospital cost attributable to HCAIs could be reduced by between 3% and 23%, depending on the effectiveness of the electronic audit and feedback system. If introduction of the electronic audit and feedback system into current practice could lead to a reduction in the incidence of HCAIs by at least 15%, it would have a ≥0.75 probability of affording the National Health Service (NHS) a cost-effective intervention.
Conclusion If the introduction of the electronic audit and feedback system into current practice in a hypothetical general hospital in England can improve hand hygiene compliance among front-line HCPs leading to a reduction in the incidence of HCAIs by ≥15%, it would potentially afford the NHS a cost-effective intervention.
- cost
- healthcare associated infections
- HCAI
- England, NHS, nosocomial infection
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
This is the first published study to evaluate the potential clinical and economic impact of reducing the incidence of healthcare-associated infections (HCAIs) in a hypothetical general hospital in England.
This was a modelling study based on disparate sources of published evidence.
The costs and consequences of introducing an electronic audit and feedback system into current practice to improve hand hygiene compliance among front-line healthcare professionals (HCPs) in an average general hospital in England were estimated from a model depicting the pathways and associated management of adult inpatients and front-line HCPs who acquire a HCAI in the hospital environment over a period of 1 year.
The relationship between HCPs improving compliance with hand hygiene and reducing the background incidence of HCAIs is uncertain.
The model does not consider HCPs’ adaptation to the electronic audit and feedback system and subsequent decline in compliance nor does it distinguish between different types of pathogens causing HCAIs and the definition of HCAI would appear to vary between clinicians.
Introduction
Healthcare-associated infections (HCAIs) are those occurring in a healthcare setting that were not present prior to a patient entering that care setting.1 HCAIs can develop either as a direct result of healthcare interventions or from being in contact with a healthcare setting.2 The epidemiological evidence indicates that hand-mediated transmission is a major contributing factor in the acquisition and spread of infection in hospitals, and such transmission can occur directly via hands, or indirectly via an environmental source (eg, commodes, wash bowls, blood pressure monitors, mobile phones).3 4 HCAIs can be caused by a range of pathogens including meticillin-resistant Staphylococcus aureus (MRSA), meticillin-sensitive Staphylococcus aureus, Clostridium difficile (C. difficile) and Escherichia coli (E. coli).5 Antibiotics are the mainstay of HCAI management,6 although their use can increase the likelihood of infection from drug-resistant organisms and C. difficile.6 7
HCAIs pose a serious risk to patients, healthcare practitioners (HCPs) and visitors in a healthcare setting. Within a general hospital, HCAIs are more likely to occur among patients who become vulnerable to infection due to several factors, such as extended and inappropriate use of invasive devices and antibiotics, undergoing a high-risk and sophisticated procedure, being immunocompromised and other severe underlying conditions.8 Inadequate infection control expertise and insufficient hygiene levels can also be contributing factors.8
Public Health England monitors the epidemiology of certain HCAIs through routine surveillance programmes, and also advises on how to prevent and control infection in establishments, such as hospitals.9 All National Health Service (NHS) hospitals must have an infection prevention service in place. Evidence-based guidelines for preventing HCAIs in NHS hospitals in England state that HCPs need to apply standard infection control precautions to the care of all patients.10 The guidelines also affirm that one aspect of infection control is the consistent adherence to a hygiene protocol comprising: hospital environmental hygiene; hand hygiene; use of personal protective equipment; safe use and disposal of sharps; and principles of asepsis.10
These guidelines specify that a hand hygiene protocol requires HCPs to decontaminate their hands: (1) immediately before each episode of direct patient contact or care, including clean/aseptic procedures; (2) immediately after each episode of direct patient contact or care; (3) immediately after contact with body fluids, mucous membranes and non-intact skin; (4) immediately after other activities or contact with objects and equipment in the immediate patient environment that may result in the hands becoming contaminated; and (5) immediately after the removal of gloves.10 This hand hygiene protocol is consistent with the World Health Organization’s (WHO) ‘My 5 Moments of Hand Hygiene’.11
Audit with performance feedback is an important component of the WHO’s hand hygiene guidelines4 and is undertaken routinely in many high and low income countries. Audit with feedback can improve the uptake of healthcare interventions generally12 and is an important component of many hand hygiene interventions.13 High levels of hand hygiene adherence are frequently overestimated14 as a result of the Hawthorne effect15 and other sources of bias.14 Awareness of being watched encourages HCPs to cleanse their hands more often14 16 17 while audit periods are typically brief (15–20 min) giving an incomplete picture of usual practice, especially if intricate procedures with high risk of hand contamination are postponed until the audit is over.17
There have been numerous systematic reviews assessing the risks and impact of HCAIs (too many to quote) in both high and low income countries. In particular, two systematic reviews explored the effectiveness of automated hand hygiene monitoring systems, and both included electronic devices. Both reviews concluded that such systems may be of benefit, but acknowledged that the primary studies were poorly controlled (pre/post test designs) and both recommended an economic analysis.18 19 There is minimal published evidence on the association between HCAIs and hand hygiene,13 so it is hard to quantify the effect of improving hand hygiene on the rate of acquiring HCAIs. However, one study in Geneva between 1994 and 1998 saw hand hygiene compliance increase from 48% to 66%, resulting in a reduction in the annual HCAI prevalence, from 16.9% in 1994 to 9.9% in 1998.20 Against this background, this study considers the potential cost-effectiveness of reducing the incidence of HCAIs by varying amounts following the introduction of a ‘hand hygiene electronic audit and feedback system’ into current practice to improve hand hygiene compliance among front-line HCPs in a hypothetical general hospital in England.
Methods
Study design
This was a modelling study which estimated the potential clinical and economic impact of reducing the incidence of HCAIs in a hypothetical general hospital in England, by improving compliance with hand hygiene protocols among front-line HCPs.
Patient and public involvement
Patients and members of the public were not directly involved in this study.
Data sources
A systematic literature review was performed by searching PubMed, the Kings Fund, House of Commons library, NHS digital (Hospital Episode Statistics, workforce statistics and bed occupancy data) and the Office for National Statistics for relevant publications on HCAIs published between January 2008 and June 2018. The search focused on epidemiology, clinical and health outcomes, management, resource use, costs and productivity and the search strings used to identify publications contained terms such as: ‘Hospital acquired infection’ OR ‘Nosocomial infection’ OR ‘Healthcare associated infection’ OR ‘HAI’ OR ‘HCAI’ AND ‘epidemiology’ OR ‘prevalence’ OR ‘incidence’ OR ‘mortality’ OR ‘Cost’ OR ‘Cost-effectiveness’. The search was limited to publications in the English language and only studies concerning humans. If multiple sets of the same data were found over the 10 year period then the most recent published data set was used. Manual searches were also performed based on citations in the published articles and suggestions from the clinical co-authors.
The searches yielded 1104 different publications, of which 905 were excluded because of duplication or lack of relevance generating 199 publications to review in full. Of the 199 publications which were reviewed, a further 100 were excluded as they did not meet the study criteria. This left 99 articles for data extraction of which 44 contained relevant data which were used to inform this modelling study.
Health economic modelling
A decision model was constructed depicting the pathways and associated management of adult inpatients and front-line HCPs who acquire a HCAI in the hospital environment over a period of 1 year (figure 1). The model considers the costs and consequences of current practice compared with introducing an electronic audit and feedback system to improve hand hygiene compliance among front-line HCPs in an average general hospital in England. The model considers the impact of these two strategies on HCAI prophylaxis among both adult inpatients and front-line HCPs.

Decision model depicting the management of HCAIs in an average NHS general hospital. The number below each branch depicts the probability of following a particular pathway, and is based on a 25% reduction in the incidence of HCAIs following the introduction of an electronic audit and feedback system into current practice to improve hand hygiene compliance among front-line HCPs. HCAI, healthcare-associated infection; HCP, healthcare practitioner; NHS, National Health Service.
Healthcare resource use
The model incorporated the following assumptions (table 1):
Model inputs
In an average year in an average NHS hospital in England, there would be 76 053 adult admissions,21 510 adult inpatient beds22 and 4473 front-line HCPs.23
4.7% of adult inpatients would acquire a HCAI.24
3.5% of patients who acquire a HCAI would die from their infection.25
1.72% of front-line HCPs would acquire a HCAI (an estimated mean from two different sources).26 27
Every adult inpatient who acquires a HCAI would have an increased length of stay.
Once an adult inpatient acquires a HCAI, 90% would remain on the ward to which they were admitted, 10% would be isolated28 and 0.04% would be transferred into intensive care (ICU).21 29 30
Patients would remain on the ward or in an isolation unit for a mean of 9.1 days.29
Patients who are transferred to ICU would remain there for a mean of 4.0 days before returning to the ward.30
Healthcare resource use and corresponding costs pertaining to bed occupancy and outpatient visits are detailed in tables 1 and 2. The daily cost of bed occupancy at 2016/2017 prices (table 2) was applied to the additional length of hospital stay to estimate the cost of hospital stay attributable to HCAIs. The costs of diagnostic tests, prescribed medication and clinician time were assumed to be included in the daily cost of hospital stay.
Hospital resource costs at 2016/2017 prices
HCPs absenteeism from work
According to the clinical authors, it is NHS Hospital Trust policy that HCPs who develop an infection should not attend work. The model assumed that 90% of front-line HCPs who acquire a HCAI would not attend work for a mean of 5 days, while the other 10% would attend.
The cost of front-line HCPs being absent from work due to HCAIs comprises the cost of replacing HCPs who acquire a HCAI with either bank or agency staff (table 2). The cost of replacing front-line HCPs with bank staff was calculated using a weighted average of the cost per day per staff type weighted by the proportion of the different types/grades of front-line staff that work in NHS hospitals in England.23 The cost of agency staff was assumed to be the maximum 55% above the daily cost of NHS employees, excluding any administrative fees.31 The model assumed that 14% of absent HCPs would be replaced by agency or bank staff, of which 70% would be bank staff and the other 30% would be agency staff.
Hand hygiene electronic audit and feedback system
The model assumed the electronic audit and feedback system comprises a technology (such as ‘Tork Vision Hand Hygiene’) which monitors compliance with hand hygiene practices according to the WHO’s five moments for hand hygiene (ie, moments 1,4 and 5).11 This is accomplished by tracking HCPs’ movements with high precision in real time and by combining their use of hand sanitisers (USAGE events) with their physical movements in relation to patients’ beds (OPPORTUNITY events). The compliance results are fed back to the HCPs both at a group and individual level. The system incorporates the use of antennae mounted in the ceilings in hospital wards, tags worn by HCPs and hand hygiene product dispenser tags that record dispensing actions.
One feasibility study showed that the electronic audit and feedback system led to a 20% increase in compliance with hand hygiene practices (ie, cleaning hands before patient contact, cleaning hands after patient contact and cleaning hands after contact with patient surroundings (WHO’s Hand Hygiene moments 1, 4 and 5).32 The base case model assumes that introducing the electronic audit and feedback system into current practice to improve compliance with hand hygiene protocols would lead to a reduction in the incidence of HCAIs by 25%. However, the effect of reducing the incidence of HCAIs by 20%, 15%, 10% and 5% has also been evaluated. The model assumes that the electronic audit and feedback system would cost an average hospital in England £1.50 per inpatient bed per day.
Model outputs
The model outputs for an average NHS hospital with 76 053 adult admissions,21 510 adult inpatient beds22 and 4473 front-line HCPs23 were:
The annual number of HCAIs avoided.
The annual number of HCAI-related patient deaths avoided.
The annual number of HCAI-related days of avoided absence by HCPs.
The annual number of HCAI-related occupied bed days.
The total annual hospital cost attributable to HCAIs comprising:
The annual cost of patient management.
The annual cost of HCP management.
The annual cost of agency staff.
The annual cost of the electronic audit and feedback system to improve hand hygiene compliance.
Economic evaluation
The cost-effectiveness of introducing the electronic audit and feedback system into current practice was calculated by dividing the cost difference between the two hand hygiene strategies by the difference in health outcomes of the two strategies. If use of the electronic audit and feedback system leads to an improvement in outcome for less cost, it was considered a dominant (cost-effective) strategy.
The cost–benefit (return on investment) of introducing the electronic audit and feedback system into current practice was also calculated by dividing the net financial benefit of the strategy by the cost of implementing the electronic audit and feedback system.
Sensitivity analysis
Probabilistic sensitivity analysis was undertaken to evaluate uncertainty within the model by applying a distribution to all the model inputs. A beta distribution was assigned to the probabilities and a gamma distribution to resource use and costs, by assuming a 10% SE around the mean values. This enabled the generation of 10 000 iterations of the model by randomly selecting a value from all the different inputs simultaneously. The outputs from these iterations was a distribution of costs and outcomes over 1 year for each strategy. The analysis also estimated the probability of implementing the electronic audit and feedback system to improve hand hygiene compliance among front-line HCPs being cost-effective when compared with current practice.
Deterministic sensitivity analysis was also performed to examine the effect of individually decreasing and increasing by 25% the value of each of the key model inputs and assumptions.
Results
HCAI-related outcomes
The base case model estimated that in an average NHS hospital with 76 053 adult admissions per annum,21 510 adult inpatient beds22 and 4473 front-line HCPs23 there are 3683 HCAIs per annum. Introduction of the electronic audit and feedback system into current practice was estimated to potentially reduce this to 2762 HCAIs per annum (table 3). The model also estimated that there are 126 HCAI-related patient deaths per annum in an average NHS hospital and this could potentially be reduced to 95 deaths following introduction of the electronic audit and feedback system into current practice. Hence, introduction of the electronic audit and feedback system into current practice could potentially lead to the avoidance of 921 HCAIs and 31 HCAI-related patient deaths and free-up 7794 hospital bed days for alternative use, equivalent to 4% of the annual number of hospital bed days. Additionally, 86 days of front-line HCPs being absent from work could be avoided (table 3). These estimates can vary according to the percentage reduction in HCAIs following introduction of the electronic audit and feedback system into current practice (table 3).
Expected HCAI-related outcomes in an average general NHS hospital stratified by percentage reduction in HCAIs
HCAI-related hospital costs
The base case model estimated that an average NHS general hospital with 76 053 adult admissions per annum,21 510 adult inpatient beds22 and 4473 front-line HCPs23 incurs an annual cost of £11.9 million attributable to HCAIs, of which >99% is attributable to patient management (table 4). This could potentially be reduced by 23% (£2.7 million) following introduction of the electronic audit and feedback system into current practice (table 4). These estimates can vary according to the percentage reduction in HCAIs following introduction of the electronic audit and feedback system into current practice (table 5).
Expected costs in an average general NHS hospital attributable to HCAIs (assumes the electronic audit and feedback system protocol leads to a 25% reduction in HCAIs)
Expected costs in an average general NHS hospital attributable to HCAIs stratified by percentage reduction in HCAIs
Cost-effectiveness analysis
Outputs from the model showed that introduction of the electronic audit and feedback system into current practice is expected to lead to a cost decrease and a corresponding increase in outcomes for an average hospital with 76 053 adult admissions per annum,21 510 adult inpatient beds22 and 4473 front-line HCPs.23 Thus, use of the electronic audit and feedback system potentially affords the NHS a cost-effective intervention, since it could lead to an improvement in outcomes for less cost.
Cost–benefit analysis
The net benefit of introducing the electronic audit and feedback system into current practice varied between £33 800 and £2.4 million, depending on the percentage reduction in the incidence of HCAIs (table 6). The analyses showed that if the percentage reduction in the incidence of HCAIs is ≥3%, then the cost of introducing the electronic audit and feedback system into current practice in an average general hospital would be offset by the ensuing cost-reductions. The cost-benefit ratio showed that for every £1 spent by an average general hospital on the electronic audit and feedback system, it could benefit from a reduction in costs of ≥£1.10 attributable to HCAIs (table 6).
Cost–benefit analysis
Sensitivity analyses
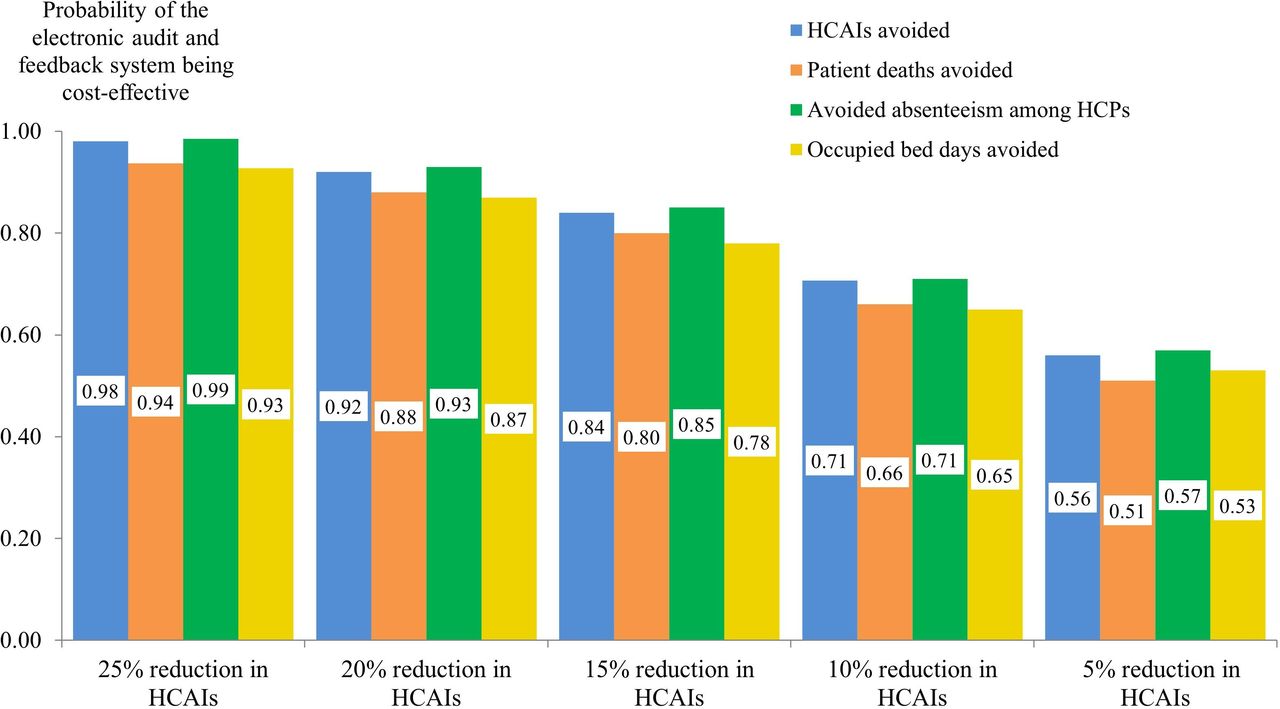
Probabilistic sensitivity analysis highlighted the distribution in the incremental costs and outcomes at 12 months between the two hand hygiene strategies (figure 2). Outputs from the analysis suggest that use of the electronic audit and feedback system has to lead to a reduction in the incidence of HCAIs by at least 15% in order to afford the NHS an intervention which has a sufficiently high probability of being cost-effective (ie, ≥0.75) (figure 3). In the base case model, the probability of the electronic audit and feedback system being cost-effective was ≥0.90 (figure 3).

Scatterplot of the incremental costs and outcomes between the two strategies in 1 year in an average general hospital following 10 000 iterations of the model, stratified by reduction in HCAI incidence associated with the electronic audit and feedback system. (A) HCAIs avoided. (B) Patient deaths avoided. (C) Days HCPs are absent from work. (D) Occupied hospital bed days. HCAI, healthcare-associated infection; HCP, healthcare practitioner.
{kind=link}
{kind=link}
{kind=link}
Probability of the electronic audit and feedback system being cost-effective compared with current practice, stratified by reduction in HCAI incidence. HCAI, healthcare-associated infection; HCP, healthcare practitioner.
Deterministic sensitivity analysis (table 7) was performed on the base case model (ie, by assuming the electronic audit and feedback system leads to a 25% reduction in the incidence of HCAIs). The analysis suggests that the probability of the electronic audit and feedback system affording the NHS a cost-effective intervention is primarily sensitive to:
Deterministic sensitivity analysis (assumes the electronic audit and feedback system leads to a 25% reduction in the incidence of HCAIs)
Its ability to reduce the incidence of HCAIs.
Probability of patients acquiring a HCAI.
Annual number of adult admissions into an average hospital.
Average additional length of hospital stay after acquiring a HCAI.
The probability of the electronic audit and feedback system affording the NHS a cost-effective intervention was found to be less sensitive to changes in the other model inputs. In particular, increasing the cost of the electronic audit and feedback system has negligible effect on the results since it accounts for only 3% of the total cost attributable to HCAIs incurred by an average NHS general hospital in the base case model.
Discussion
This study estimated that in an average NHS hospital with 76 053 adult admissions per annum,12 510 adult inpatient beds13 and 4473 front-line HCPs,14 there are 3683 HCAIs per annum, and as a consequence 31 176 bed days are occupied by patients with these infections. This equates to 17% of the annual number of all bed days in an average NHS hospital. Furthermore, if the mean additional length of hospital stay as a result of a HCAI was reduced by half (from 9.1 days19 to 4.5 days), 8% of all bed days would still be occupied by patients with a HCAI. There is an opportunity cost to this HCAI-related bed occupancy. There has been an increase in hospital bed occupancy in England in recent years, due in part to the increased levels of hospital activity.33 Consequently, this impacts on the speed with which patients can be admitted into hospital. It has also been shown to be a significant factor in the deterioration in performance against the 4-hour standard for admitting or discharging patients from hospital accident and emergency departments.33 The shortage of available beds has also contributed to patients being admitted to hospitals outside their local area, which may delay their recovery.33 Hence, this study may have underestimated the potential cost-effectiveness of the electronic audit and feedback system, when one considers its potential to result in a decrease in the number of HCAI-related occupied bed days and thereby facilitate an increase in the speed of hospital admissions.
WHO guidance highlights tuberculosis as an occupational risk factor for HCPs34; they are also at risk of acquiring bloodborne infections (eg, HIV, hepatitis B and C). While HCPs may not be at high-risk of ‘classic’ HCAIs, they are at risk of community-acquired infections brought into a hospital by patients. These include gastrointestinal infections (eg, norovirus) and respiratory infections (eg, influenza, respiratory syncitial virus). Rarely, HCPs may also develop varicella, measles or mumps through patient contact. Risks of acquiring a HCAI are higher for HCPs than for members of the public visiting a hospital because they have more patient contacts than visitors, which are sustained over a longer period of time. Poor hand hygiene plays an important role in the spread of gastrointestinal infections.35–37 Accordingly, the model estimated that 1.72% of front-line HCPs would acquire a HCAI.26 27 Sensitivity analyses showed that changing this value has negligible impact on the study’s findings.
This study is predicated on an electronic audit and feedback system which monitors compliance with hand hygiene practices according to the WHO’s Moments 1, 4 and 510 which are designed to reduce transmission of pathogens between patients. This study showed that introducing such an electronic audit and feedback system into current practice to improve hand hygiene compliance in a hypothetical general hospital in England is potentially cost-effective providing it leads to a ≥15% reduction in the incidence of HCAIs. There is substantial evidence that increasing hand hygiene compliance is associated with reducing HCAIs, although uncertainty remains about the proportion of HCAIs that can be prevented by improving hand hygiene compliance.4 Moreover, it has been suggested that estimating hand hygiene compliance with the WHO’s Moments 1, 4 and 5 by monitoring leads to reasonable estimates of overall compliance with all 5 Moments.38 39 Limitations with the published evidence are due to the fact that designing and conducting robust, ethical, randomised controlled trials in the field of hand hygiene is challenging.13 Consequently, the recommendations on hand hygiene protocols are based on evidence from non-randomised controlled studies, quasi-experimental studies, observational studies and laboratory studies with volunteers.10
There have been few studies assessing the health economic impact of hand hygiene protocols within healthcare settings. One review of economic studies on the impact of alcohol-based hand hygiene products in healthcare organisations40 concluded that, while further research is required to measure the direct impact of improved hand hygiene on infection rates, the potential benefit of providing alcohol-based handrubs is likely to outweigh costs, and their wide-scale promotion should continue. Many of the older studies are not directly comparable to our study since they have examined direct costs of alternative handrubs, whereas this study has assessed the costs of introducing an electronic audit and feedback system into current practice to improve hand hygiene compliance with the clinical consequences and associated costs as they pertain to both patients (eg, increased length of hospital stay) and HCPs (eg, absenteeism from work).
One recent study has examined the cost-effectiveness of multi-modal hospital interventions to improve hand hygiene compliance in a middle-income country.41 However, this study was restricted to assessing the relationship between hand hygiene compliance and preventing a MRSA blood stream infection in ICU settings. Other economic studies in high-income countries20 42 43 reported the potential for a hand hygiene intervention to be cost-effective if the incidence of HCAIs was reduced by at least 1%, without reporting the probability of the intervention being cost-effective. Our study also suggests that introducing an electronic audit and feedback system into current practice to improve hand hygiene compliance would be cost-saving and cost-effective if the incidence of HCAIs was reduced by at least 3%. However, the probability of it being cost-effective is ≥0.75 if it leads to a ≥15% reduction in the incidence of HCAIs. Nevertheless, it is difficult to compare these studies with our own due to different study designs and other methodological differences.
Observational studies of hand hygiene behaviour indicate an abundant risk of exogenous (cross) infection as HCPs move rapidly between patients, often without undertaking adequate hand hygiene.44 45 Additionally, the ICU environment is heavily contaminated with hospital strains of pathogenic organisms which have been shown to cause infection.46 Increased hand hygiene performance has been shown to reduce endogenous infection.47 48 Improving HCPs’ behaviour in infection prevention and control is challenging, since their behaviour is influenced, in part, by individual preferences and a degree of professional isolation.49 Clearly, for any hand hygiene protocol to be clinically effective and cost-effective, HCPs’ adherence to hand hygiene guidelines should be regularly audited, and the findings should be reported back in order to improve and sustain high levels of compliance. Additionally, healthcare organisations should provide regular training in risk assessment. A recent review concluded that the effectiveness of auditing and feedback depends on HCPs’ baseline performance and how feedback is provided to them.50 Moreover, such electronic audit and feedback can lead to small, but potentially important improvements in HCPs’ practice.50 Patients, relatives and other visitors should also be provided with information about the importance of hand hygiene and how to keep their own hands clean.
Study limitations
This health economic assessment of introducing an electronic audit and feedback system into current practice to improve hand hygiene compliance among front-line HCPs is subject to some uncertainty because it was based on indirect sources of evidence and a series of assumptions. The relationship between HCPs improving compliance with hand hygiene and reducing the background incidence of HCAIs is uncertain. Moreover, the model does not consider HCPs’ adaptation to the electronic audit and feedback system and subsequent decline in compliance. Furthermore, the model does not distinguish between different types of pathogens causing HCAIs and the definition of HCAI would appear to vary between clinicians.
The model was populated with estimates for an ‘average general hospital’ and ‘average patients’ and does not consider the impact of other factors that may affect the results, such as different ward types, patients’ age or co-morbidities, clinician specialties etc. By restricting the framework of the model to the average general hospital, the analysis does not consider the impact of improving hand hygiene compliance in specialist centres such as cancer hospitals, mental health and disability units and women’s hospitals. However, there is no reason to assume that the findings from this study would be any different in a specialist hospital. Additionally, the analysis is limited to HCAIs among adult inpatients and does not consider paediatric patients, accident and emergency or outpatient departments. Neither does the model consider that patients may acquire a HCAI and be discharged from hospital before symptoms emerge. The model assumes that patients who do not die from a HCAI are discharged, but in reality some patients may die from other reasons. The analysis excluded patients’ costs and indirect costs incurred by society as a result of employed patients or HCPs taking time off work as a result of a HCAI. Additionally, estimating the value of improving hand hygiene overall is beyond the remit of this study. Notwithstanding this, the Authors chose to focus on electronic monitoring systems because of their higher degree of accuracy and current level of interest. The evidence shows that manual audits lead to a marked Hawthorne effect and other sources of bias (eg, postponing complicated clinical procedures until the auditor has gone).16 The other method of measuring adherence is product consumption which is not very accurate and provides little information.17 Inaccuracies associated with manual hand hygiene audit are such that it is no longer considered the best approach and there is increasing interest in combining periodic manual audit with continuing electronic monitoring to give an overall picture of behaviour.51 52 Clearly, a controlled study is required to compare the introduction of an electronic audit and feedback system into current practice to improve hand hygiene compliance with current practice in order to validate the outcomes of this analysis.
Conclusion
Within the study’s limitations, the introduction of an electronic audit and feedback system into current practice to improve hand hygiene compliance among front-line HCPs in a hypothetical general hospital in England would afford the NHS a cost-effective intervention if it yielded a reduction in the incidence of HCAIs by ≥15%.
References
Footnotes
Contributors JFG designed the study, managed the analyses, performed some analyses, checked all the other analyses and wrote the manuscript. TK conducted much of the analyses. DJG and NW scrutinised the analyses, suggested further analyses and helped interpret some of the findings. All the authors were involved in revising the manuscript and gave final approval. JFG is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Funding This study was funded by Essity Hygiene and Health AB, Mölndal, Sweden. The study’s sponsors had no involvement in the study design, the collection, analysis and interpretation of the data, the writing of this manuscript and the decision to submit this article for publication. The views expressed in this article are those of the authors, and not necessarily those of Essity Hygiene and Health.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.