


Abstract
Background/Aim: Head and neck cancer is a major malignancy worldwide. The treatment strategy for head and neck cancer usually involves radiotherapy. The main side effect of radiotherapy is radiation dermatitis. Thus, determining the most effective topical regimen for the prevention of radiation dermatitis in head and neck cancer patients is a critical issue. Patients and Methods: PRISMA-NMA guidelines were used in this network meta-analysis. We included only randomized control trials. A random effects model was used. Heterogeneity was evaluated by I2 and Cochran’s Q tests. Results: We included a total of 1,304 patients in the network meta-analysis. Among them, olive oil was the only effective regimen when compared with usual care (OR=0.18, 95%CI=0.03-0.95). The I2 value was 56%. The test of heterogeneity yielded a p-value of 0.10. Conclusion: Olive oil was the most effective regimen for the prevention of radiation dermatitis.
Head and neck cancers are a major malignancy worldwide and include nasopharyngeal, oral cavity, oropharyngeal, hypopharyngeal, and laryngeal cancers. The global burden of head and neck cancer has been increasing (1). Treatment strategies for head and neck cancer include radiotherapy, chemotherapy, targeted therapy, immunotherapy, and surgery. Following radiotherapy for head and neck cancer, the most common side effects in cancer survivors are radiation dermatitis and oral mucositis (2).
Radiation dermatitis (RD) usually appears within a few weeks after the start of radiation therapy. Despite advances in radiotherapy techniques, skin reactions are still inevitable. Specifically, approximately 85% of radiated patients with head and neck cancer develop moderate to severe skin reactions (3), the severity of which can be evaluated using the Common Terminology Criteria for Adverse Events proposed by National Cancer Institute (NCI-CTCAE) criteria (4) or the Radiation Therapy Oncology Group (RTOG) criteria (5). Early symptoms include generalized erythema, dry desquamation, pruritus, epilation, scaling, dyspigmentation, and hair loss (6). Radiation dermatitis can affect the patient’s quality of life. When symptoms are severe, radiation therapy may even need to be interrupted.
Because radiation dermatitis may interfere with the course of radiation therapy, it is common in clinical practice to adopt prophylactic interventions prior to the onset of radiation dermatitis; such prophylaxis consists of general skin care measures and topical agents (7, 8). The main topical agents used in clinical practice include topical corticosteroids, trolamine, Aloe vera, sucralfate, or hyaluronic acid. Most of the studies investigating this issue use different interventions, but the effects are still controversial, thus finding safe and effective prevention strategies is a priority for clinicians and patients.
Although few systematic reviews have reported whether each specific regimen may alleviate radiation dermatitis in patients with head and neck cancer (9, 10), there is a lack of studies demonstrating cross-intervention comparisons between different prevention strategies for radiation dermatitis. Since determining the most effective topical regimen for the prevention of radiation dermatitis in head and neck cancer patients is critical, we conducted this network meta-analysis to identify the most effective prophylactic regimen.
Patients and Methods
Study protocol. This study was conducted following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline for Network Meta-Analyses (NMA) (11). We registered this meta-analysis on the International Prospective Register of Systematic Reviews (PROSPERO) (CRD: CRD42021282759).
Literature search. Three authors (CHH, MYW, and YCW) independently queried three electronic databases, including PubMed, Cochrane, and Embase, from inception to October 2021. Inconsistency among the search results was resolved by consensus. We set the keywords as [(head and neck cancer) OR (head and neck neoplasm) OR (head and neck tumor) OR (head and neck carcinoma) OR (nasopharyngeal cancer) OR (oropharyngeal cancer) OR (oral cavity cancer) OR (laryngeal cancer) OR (hypopharyngeal cancer)] AND [(radiodermatitis) OR (radiation dermatitis) OR (radiodermatitis) OR (skin toxicity) OR (skin reaction) OR (skin damage) OR (skin reactions)) AND ((prevention) OR (prophylaxis)] (9). We also checked the references of related articles for additional studies.
Inclusion and exclusion criteria. The systematic review included: 1. studies investigating the topical prevention of radiation dermatitis in head and neck cancer patients; 2. randomized control trials; 3. human studies; 4. studies written in English. After including articles meeting the above-mentioned criteria, articles that were: 1. case reports, case series, cohort studies, case-control studies, nonrandomized clinical trials, and self-control trials; 2. studies evaluating radiodermatitis of patients with other cancer (breast cancer, skin cancer, etc.), 3. without available full text; 4. conference posters; 5. conducted on pediatric patients, were excluded.
Data extraction. Three authors (CHH, MYW, and YCW) independently extracted data from the included studies; when there was a discrepancy, a senior author (YSK) was consulted. The primary endpoint was set as grade 3 or more radiation dermatitis. Since the RTOG radiation dermatitis grading and CTCAE radiation dermatitis grading are similar, we viewed both as equivalent (4, 5). A second endpoint was set as the occurrence of grade 2 or more radiation dermatitis. We extracted the data according to the intention-to-treat analysis. The most severe radiation dermatitis grade was collected. Other information, including the author, year of publication, nation in which the study was conducted, patient number, details of treatment, cancer type, and study duration were also extracted.
Statistical analysis. Generalized linear mixed models (GLMMs) were used to conduct network meta-analysis with the restricted maximum likelihood method for estimation. The p score was used to evaluate the ranking of the included treatment modalities. We checked the evidence inconsistency if there was a closed loop in the network. The heterogeneity among the studies was evaluated by using I2 and Cochran’s Q tests.
Statistical analysis was undertaken by using statistical software R (version 3.6.1) within the R studio environment (Version 1.2.5019). A p-value less than 0.05 was considered significant. For Cochran’s Q test, the p-value threshold was set as 0.10, according to the recommendation from Cochran’s handbook (12).
Bias analysis. The risk of bias (ROB) tool was used to evaluate the quality of the included randomized controlled trials. CHH and MYW evaluated the risk of bias independently using a standardized protocol, and YCW made the final decision when disagreement occurred. The ROB figure was generated by Revman 5.4. A funnel plot and Egger’s test was used to evaluate publication bias.
Results
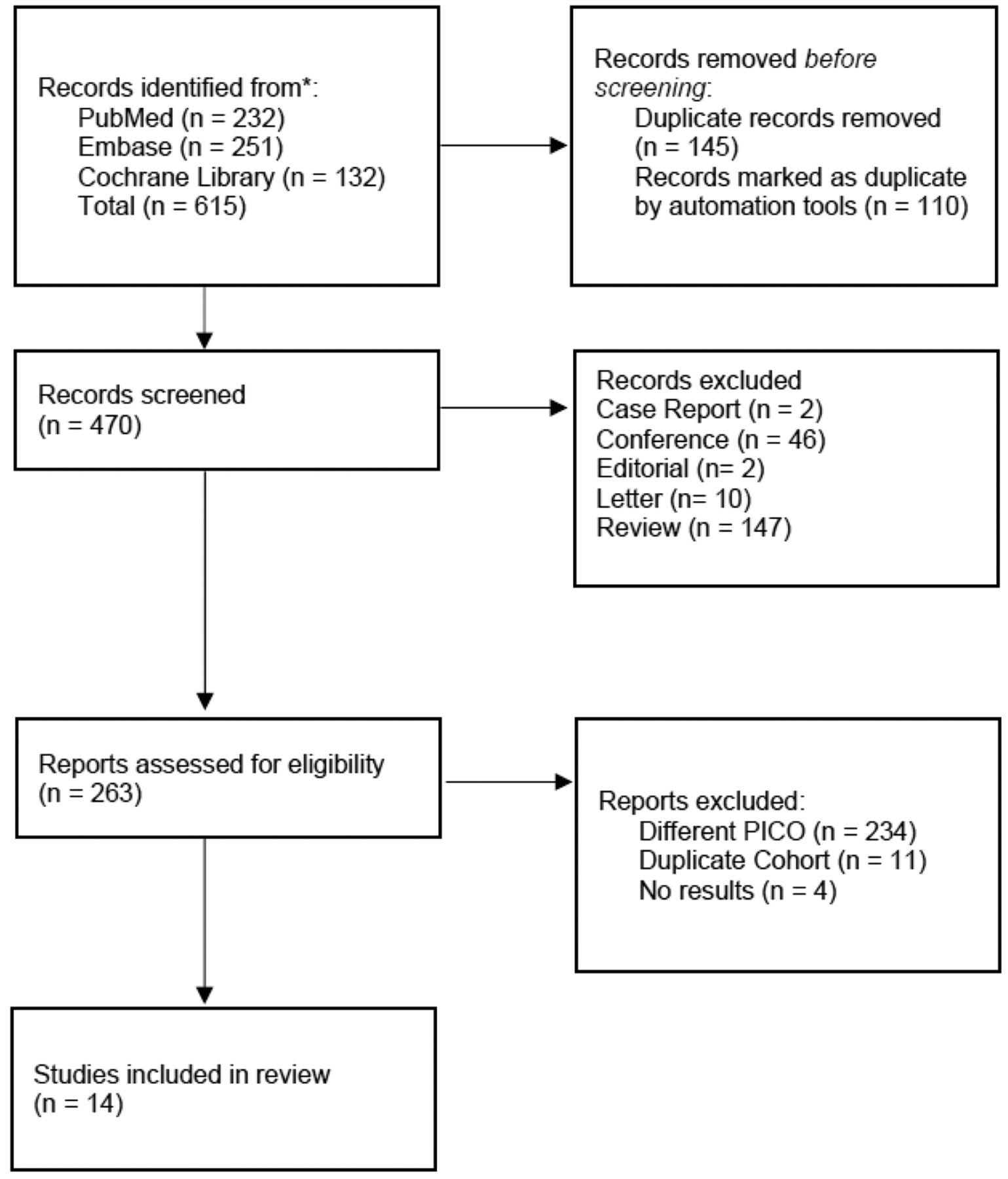
A total of 615 articles were initially identified from the three databases. A total of 145 articles were excluded as duplicates. An additional 207 articles were excluded after initial screening. A total of 249 articles were excluded after eligibility was assessed. Fourteen articles remained in the final review. The article collection flowchart is shown in Figure 1. The characteristics of the included articles are demonstrated in Table I.

PRISMA flowchart for the systematic review.
Characteristics of included studies in the systematic review.
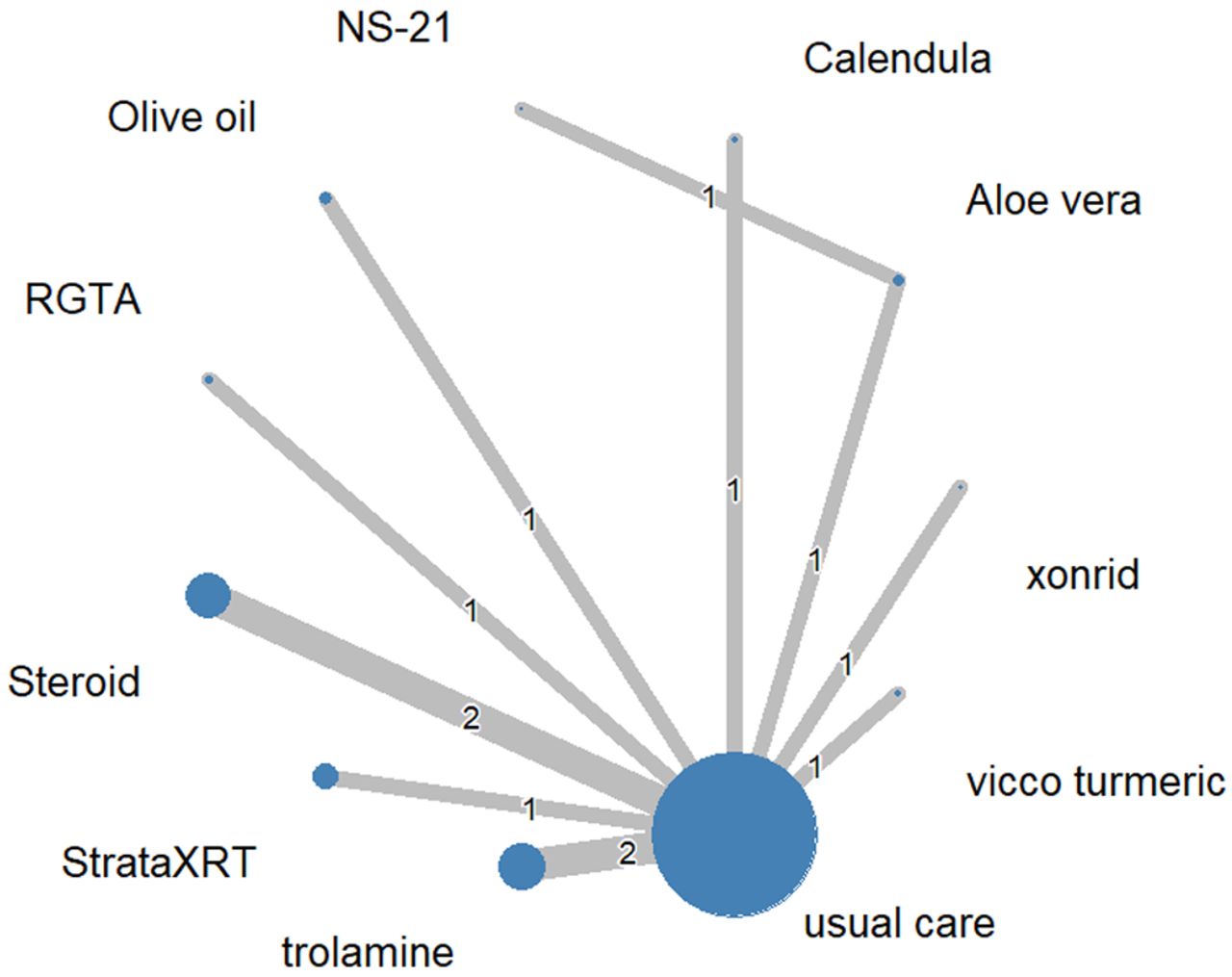
Network meta-analysis. A total of 1,304 patients were included in our network meta-analysis. The network plot is shown in Figure 2. Twelve studies were involved in the final meta-analysis. One article was excluded from the final meta-analysis due to the absence of grade 3 side effects (17). One article reported results, but the study was terminated early (22). A total of 11 treatment arms were involved in this meta-analysis. When compared with the usual care, only olive oil showed significantly better prevention ability (OR=0.18, 95%CI=0.03-0.95). The I2 was 56%, and the test of heterogeneity showed a p-value of 0.10. The statistical results are shown in Figure 3.
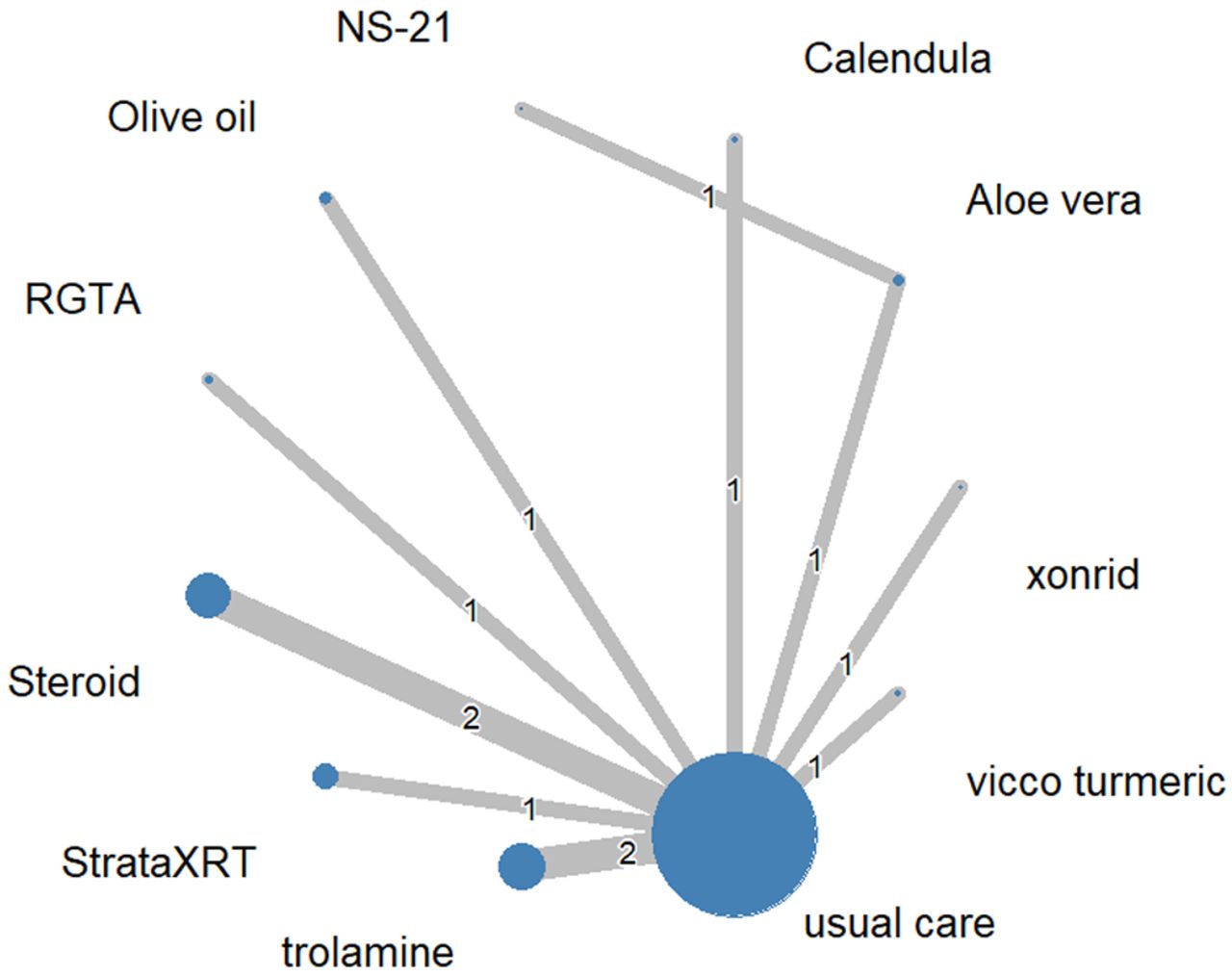
Network plot of included treatments in the network meta-analysis.

Forest plots of the network meta-analysis.
P score ranking. The p-scores of the included treatment arms were as follows: Vicco® turmeric (0.8470), calendula (0.7565), Aloe vera (0.6687), Xonrid® gel (0.6403), usual care (0.5873), RGTA® (0.5643), trolamine (0.4460), steroid (0.3617), StrataXRT® (0.2922), NS-21 (0.2384), and olive oil (0.0976). From the p score ranking, we can conclude that olive oil has the best prevention abilities among the included treatment regimens.
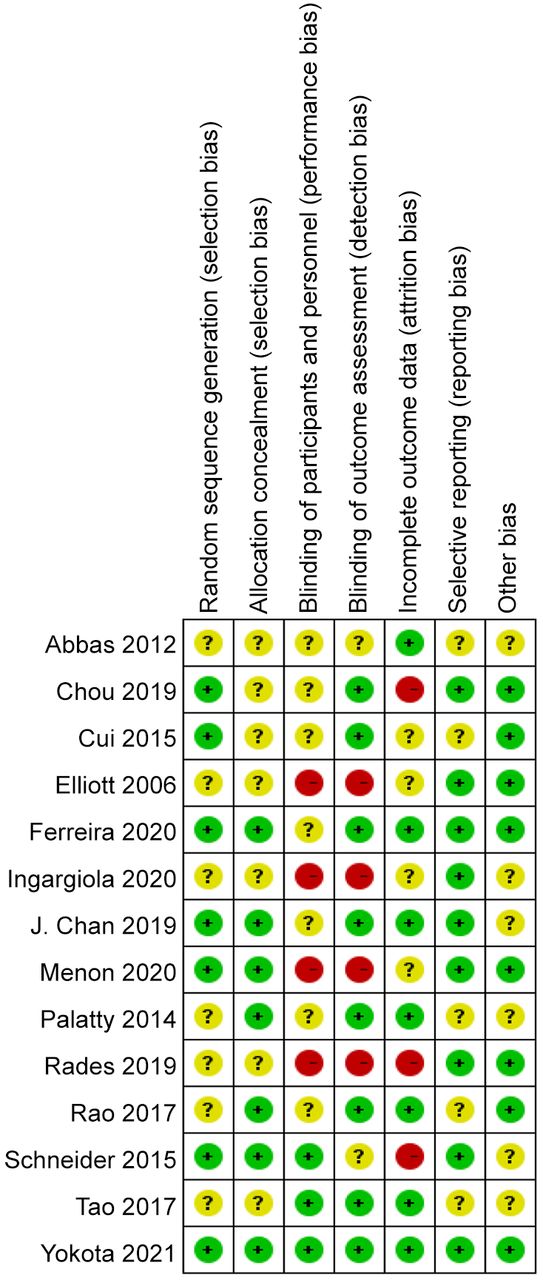
Bias analysis. The risk of bias in the included studies is summarized in Figure 4 and Figure 5. Six studies were considered at high risk of bias because one or more items were assessed as high risk. Seven studies were rated as unclear risk of bias because one or more criteria were deemed unclear. One study was considered at low risk of bias because all domains received an evaluation of low risk. The overall quality of the studies was medium. Publication bias was evaluated by a funnel plot, and the results are shown in Figure 6. From the funnel plot, we can conclude that there is no publication bias in this meta-analysis.
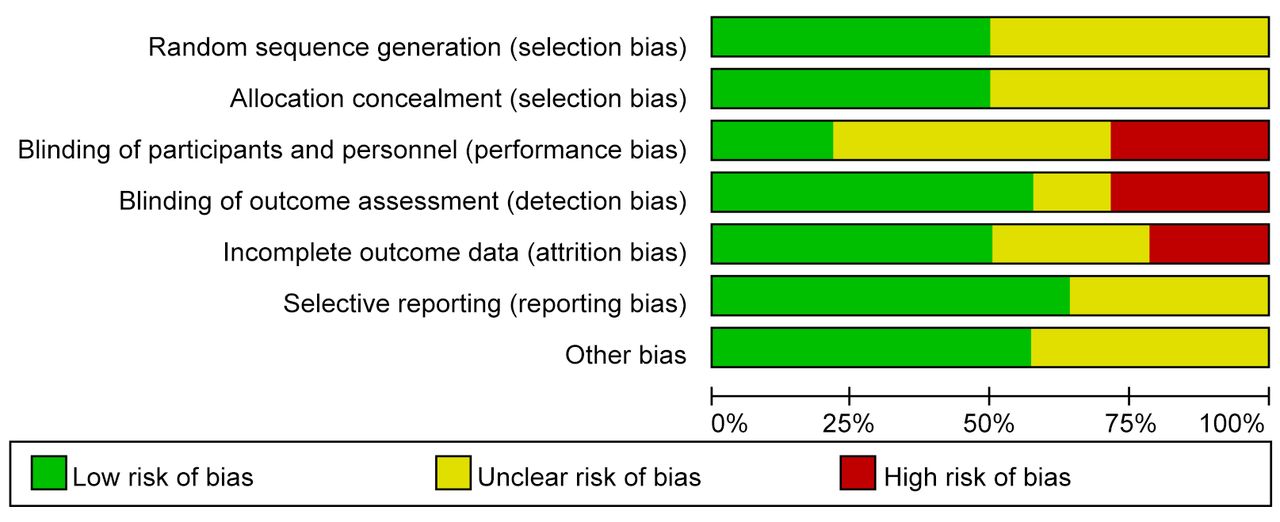
Risk of bias item presented as percentages across all included studies.

Risk of bias item for all included studies.
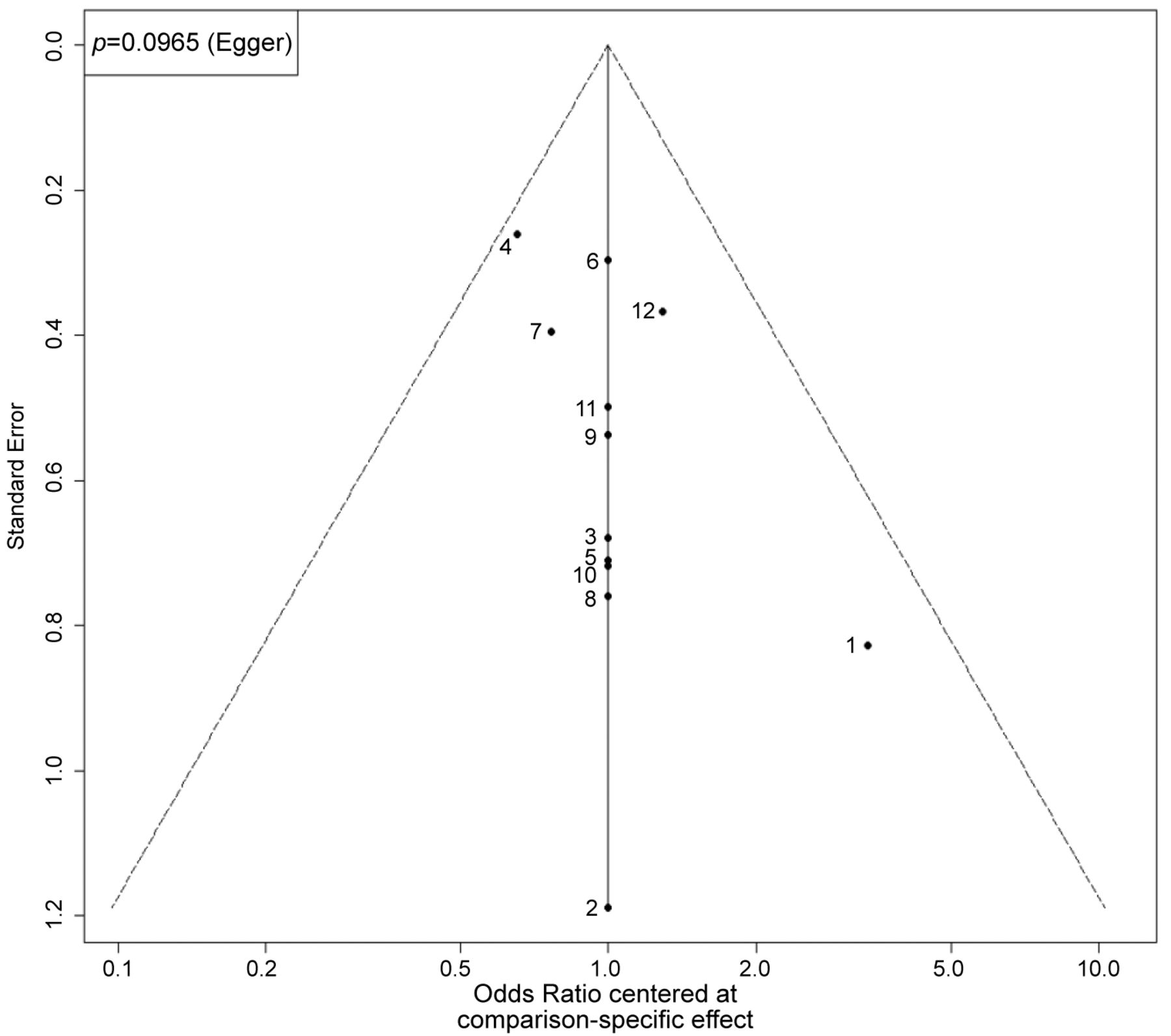
The funnel plot for the network meta-analysis.
Discussion
To our knowledge, this study is the first network meta-analysis of the topical prevention of radiation dermatitis in head and neck cancer patients. After screening for available clinical trials and observational studies, based on findings in the present systematic review and network meta-analysis, the most effective regimen for the prevention of radiotherapy-induced dermatitis is suggested to be olive oil.
Treatment strategies differ for each type of cancer, and different areas of the body have different sensitivity to radiation. The risk factors for radiation dermatitis include body site, comorbidity, lifestyle, concurrent chemotherapy, and radiation dose and duration (27). The pathology and mechanism of radiation dermatitis are not fully understood. Radiation-induced fibrosis, changes in skin lipid metabolism, apoptosis, and changes in the neovascularization process may be involved (28). To find appropriate preventive strategies, understanding the possible risk factors and pathological mechanisms is important; however, there is still a lack of research confirming which preventive strategies are the most effective.
Olive oil is a widely available treatment regimen. A previous study showed that olive oil is also effective in the prevention of radiation dermatitis in breast cancer patients (29) . Since the mechanism of radiation dermatitis is similar in nasopharyngeal cancer and breast cancer, the effect of olive oil is more convincing.
According to our network meta-analysis, NS-21, RGTA®, StragtaXRT, Vicco® turmeric, Aloe vera, calendula, Xonrid® gel, trolamine, and steroids were not statistically significant in reducing radiation dermatitis in patients with head and neck cancer, and further studies are needed to verify their effectiveness.
Aloe vera is a natural anti-inflammatory treatment that can relieve skin discomfort, but there is insufficient evidence that Aloe vera can reduce severe radiation-induced skin damage (30). Trolamine is a commonly used agent in the prevention of radiation dermatitis. However, a previous meta-analysis showed that trolamine is not effective in preventing radiation dermatitis in breast cancer and head and neck cancer patients (31). Our network meta-analysis confirms that Aloe vera and trolamine are not effective in preventing radiation dermatitis in head and neck cancer patients.
Topical steroids have anti-inflammatory effects. According to a previous meta-analysis, topical steroids are thought to improve wet desquamation and radiation dermatitis scores (32). However, in patients with head and neck cancer, topical steroids are considered to cause skin thinning and bacterial infections and are not recommended (33). In our study, the effects of topical steroids were not statistically significant in preventing moderate to severe radiation dermatitis in patients with head and neck cancer. More evidence is needed to determine whether topical steroids are effective in preventing radiation dermatitis in patients with head and neck cancer.
Mepitel Film, a soft silicone dressing, showed a reduction in the incidence of radiation dermatitis in patients with breast cancer (34), but a randomized clinical trial (RCT) on the prevention of radiation dermatitis in head and neck cancer patients was terminated early because 46.4% of the patients could not tolerate Mepitel® Film (22). Compared to urea, chamomile may have an effect in delaying grade 2 radiation dermatitis, but more studies are needed to verify its effect (17).
The strength of our study is that we only studied radiation dermatitis in patients with head and neck cancer and only included RCTs with high levels of evidence. Second, we conducted a comprehensive search of the literature with two independent reviewers to assess the quality of the studies and to reduce any potential bias.
There are some limitations to this network meta-analysis. First, the usual care in each study may have differed. However, in most of the studies, the usual care was thought to be ineffective. The clinical studies were conducted to improve the efficacy of prevention measures. As a result, viewing all usual care as the same is reasonable. Second, although all RCTs were considered reasonable in terms of quality, some studies had small sample sizes. Third, most of the comparisons in the network meta-analysis were indirect. More head-to-head studies are needed in the future to compare the effects of different treatments.
Studies of topical agents used in the prevention of radiation dermatitis in patients with head and neck cancer should include larger sample sizes and placebo controls to confirm the effectiveness and safety of the interventions in patients. Continuous evaluation of appropriate skincare and prophylaxis is important, and future studies should ensure randomization, blindness, and intention-to-treat using appropriate methods to reduce the possible risk of bias. In addition, trials should use appropriate control groups to assess outcomes. More high-quality RCTs are needed in the future to confirm these results.
Conclusion
Our results indicate that olive oil is the most effective treatment for the prevention of radiation dermatitis in head and neck cancer patients. However, there is inadequate evidence to make any recommendation about prevention strategy. Further large-scale, high-quality RCTs are needed to evaluate the efficacy of the prevention of radiation dermatitis in head and neck cancer patients.
Footnotes
Authors’ Contributions
YSK, KSM, and CHH conceived and designed the research; YSK, MYW, YCW, and CHH contributed to the data acquisition; YSK, YKT, and CHH analyzed data and interpreted the results; YSK, KSM, and CHH drafted, edited, and revised the manuscript; YSK, KSM, MYW, YCW, YKT, and CHH approved the final version of the manuscript.
Conflicts of Interest
The Authors declare no competing interests in relation to this study.
- Received February 16, 2022.
- Revision received March 11, 2022.
- Accepted March 14, 2022.
- Copyright © 2022, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Clinical Effect of Moisturized Skin Care on Radiation Dermatitis of Head and Neck Cancer
- Topical Prevention of Radiation Dermatitis in Breast Cancer Patients: A Network Meta-analysis of Randomized Controlled Trials
- Is Network Meta-analysis a Revolutionary Statistical Tool for Improving the Reliability of Clinical Trial Results? A Brief Overview and Emerging Issues Arising