


Abstract
The effect of perioperatively administered buprenorphine analgesia on rats subjected to surgically induced global ischaemia was assessed. Rats supplied with buprenorphine, mixed in nut paste for voluntary ingestion, displayed significant reductions in postoperative excretions of faecal corticosterone, in both magnitude and variance. This is indicative of lowered stress levels and less inter-animal metabolic variation. Although corticosterone has been reported to modulate the extent of cerebral damage, histology of coronal sections exhibited no differences in the extent of the ischaemia in buprenorphine-treated and untreated animals. A part from a slightly higher hyperthermia immediately after surgery and typical opiate-associated behaviour, the buprenorphine treatment had no apparent adverse effects on the experimental model. In contrast, the analgesic treatment improved the model by minimizing stress-associated confounding variables in the experimental animals.
Surgical stress and the resulting corticosteroid response are unwanted confounding variables in surgically induced laboratory animal models. It is, further, a moral mandate to alleviate pain in laboratory animals subjected to invasive procedures. The model of focal ischaemia analysed in this study has through the decades been one of the most used models of cerebral ischaemia worldwide (1). The surgery associated with the creation of this induced model introduces moderate pain and distress but no severe pain or high mortality (2).
Buprenorphine is the most commonly used drug for the treatment of postoperative pain in rats (3, 4). It is most often administered subcutaneously, but oral administration by gavage has also been found effective (5), although only formulations for injections and sublingual administration are available. Flecknell and co-workers (6) observed improved postsurgical recovery with better maintenance of body weight and increased water intake in rats given buprenorphine in flavoured Jell-O® following abdominal surgery. Further evidence for the beneficial effect of voluntary ingestion of buprenorphine as a means of reducing postsurgical stress was put forward by Goldkuhl and collaborators (7) in a study where the postsurgical levels of corticosterone were repeatedly monitored. Buprenorphine has been shown to be less immunosuppressive than other opioids (8). It is therefore likely that it has a less severe effect on the rat immune system when compared to corticosterone – the immunosuppressive component of the hypothalamic–pituitary–adrenal (HPA) axis and main stress-associated glucocorticoid in rats.
Corticosterone has multiple modes of action that inhibit immune response potency. Rapid effects on the immune system are mediated through receptor interactions. Slower and more profound effects are a result of altered gene expression and as many as 20% of the genes expressed in leukocytes may be under regulatory control of glucocorticoids (9). Apart from modulating the immune response, glucocorticoids have been implicated in causing hippocampal degeneration (10) and exacerbating cerebral damage (11). It has been proposed that glucocorticoids deplete hippocampal ATP reserves, rendering certain regions unable to cope with damaging insults (12, 13).
Serum glucocorticoid levels are a widely accepted objective measure of acute stress as they reflect HPA axis activation (14, 15). However, physical restraint and blood sampling are, in themselves, stressful procedures, and thus significantly limit the usefulness of blood samples for stress assessment in animals (16). Measuring glucocorticoids, or rather glucocorticoid metabolites, in urine and faeces provides a non-invasive alternative for objective assessment of stress. It also provides a tool for measuring HPA axis activation over time, as opposed to the ‘snap-shots’ provided by blood sampling (17, 18).
In the present study, rats subjected to surgically induced global cerebral ischemia were studied with the aim of minimising adverse conditions through the use of voluntarily ingested buprenorphine for perioperative analgesia. It was hypothesised that the buprenorphine treatment would decrease the stress-induced HPA axis activation resulting from the surgical procedure. This in turn should be evident as a decrease in excretion of faecal corticosterone compared to non-treated animals subjected to the same surgical procedure. It was further hypothesised that the analgesic treatment would not interfere with the desired progress of the induced ischaemia, but would, in fact, even improve its consistency and decrease the inter-individual variance.
Materials and Methods
Animals. Thirty male Wistar rats (Taconic, Ry, Denmark) with a FELASA approved health status, aged six to seven weeks, were housed in groups of four. Polycarbonate type IV cages (Techniplast, Varese, Italy) enriched with cardboard hides, with Aspen chips (Tapvei Oy., Kortteinen, Finland) as bedding material were used. The animals were subjected to standard animal house conditions: Diurnal rhythm was regulated through a 12 h light/12 h dark cycle (lights on from 8:00), and temperature was kept at 20-22°C, with a relative humidity of 30-60%. Food pellets (Atromin 1319; Brogaarden, Gentofte, Denmark) and acidified tap water were provided ad libitum. The animals were acclimatised to housing conditions and habituated to routine handling by animal technicians for seven days prior to the experiment. All laboratory animal work was carried out in accordance with Danish legislation and was approved by the Animal Experiments Inspectorate (under the Danish Ministry of Justice).
Presurgical procedures. At the first day of the experiment, three days prior to surgery (designated ‘day −3’), the rats were single housed under the previously described animal house conditions in type III cages (Techniplast) and Nutella® (2 g× kg body weight−1× day−1; Ferrero, Pino Torinese, Italy) was introduced as part of the diet. The rats were randomly divided into three groups, and single-housed for the remainder of the experiment. The first group (n=10) acted as control, not subjected to surgery or analgesic treatment. The second group (n=10) was subjected to surgery, but the animals were not treated with analgesia before or after surgery. The third group (n=10) was subjected to surgery and was given perioperative analgesia in accordance with the method used by Goldkuhl et al. (7). Briefly, the animals were fed Temgesic® (0.6 mg/kg body weight; Schering-Plough Europe, Brussels, Belgium), ground to a fine powder with a mortar and pestle and mixed in Nutella®, on the morning of the surgery at 7:00, and two days following the surgery at 7:00 and 16:00. The experiment was conducted as a blind study; the randomised allotment of animals into groups 2 and 3 was kept from researchers and technicians working with the animals to avoid biased data collection.
Surgery. Global cerebral ischaemia was induced on day 0 by means of 2-vessel occlusion during systemic hypotension as previously described by Müller and co-workers (19). Briefly, the rats were anaesthetised with a 0.15 ml subcutaneous injection of Hypnorm (10 mg/ml Fluanisone, 0.315 mg/ml fentanyl citrate; Vetapharma, Leeds, UK) followed by a 0.3 ml subcutaneous injection of Midazolam (5 mg/ml; Hameln Pharmaceuticals GmbH, Hameln, Germany). Absence of withdrawal reflexes was tested for at regular intervals throughout the entire surgical procedure. One of the femoral arteries was catheterised for monitoring of blood pressure, sampling for blood gas readings, and the induction of hypotension. Blood gases were analysed on a Radiometer ABL 555 blood gas analyser (Radiometer, Brønshøj, Denmark). Both carotid arteries were gently exposed and systemic hypotension (50 mmHg) was induced by drawing blood with a heparinised syringe through the femoral catheter. Both carotid arteries were then fully ligated for 12 minutes to induce cerebral ischaemia. Immediately following the removal of the ligatures, a stable blood pressure of 120 mmHg was induced by reperfusion of the aspirated blood together with sterile saline. The incision wounds were treated with lidocain gel (10 mg/ml; Region Hovedstadens Apotek, Copenhagen, Denmark) during anaesthesia.
Data collection. From day -3 to day 7 postsurgery food and water intake, animal body weight and body temperature were recorded at 24-h intervals. All faecal boli produced in a 24 h period were collected and stored at −20°C for corticosterone analysis. Due to corticosterone being a fairly stable molecule, the corticosterone levels in the samples can be considered to be unaltered from the time of excretion to analysis. Royo and co-workers (20) demonstrated that corticosterone levels in faecal samples exhibit less than 10% change in concentration even when stored at room temperature for 24 h.
Postoperative monitoring. After single housing, the animals were observed twice daily – once before lights were turned on at 8:00, and once after the light had been turned on for several hours at 15:00. A functional observational battery (FOB) comprising parameters and methods well-recognised in laboratory animal literature (21, 22) was applied. These included the activity level of the animal, piloerection, lacrimation, digging, grooming, body posture, and an overall behaviour-based clinical assessment. When the animals were handled in conjunction with weighing and temperature readings, further observations of reaction to handling, and estimated degree of dehydration were recorded. After recording independent observations, two animal technicians would agree on a general recovery status for each animal. If any adverse postoperative changes to the well-being of the animal were deemed too severe, the animal was euthanased immediately and excluded from the study.
Corticosterone analysis. Corticosterone was quantified according to a modified version of the method by Pihl and Hau (23). All faecal boli from one sampling window were thawed, weighed and submerged in 40 ml of 96% ethanol. Each sample was homogenised/solubilised though vigorous vortexing and incubated on a shaking table overnight (min. 12 h). The homogenate was centrifuged at 2000 ×g in a Hermle Z 400 K centrifuge (Hermle Labortechnik GmbH, Wehingen, Germany) for 20 minutes, the supernatant was decanted and the pellet discarded. A 1 ml aliquot of the supernatant was further centrifuged at 10000 ×g for 15 minutes in an Eppendorf tabletop centrifuge (Eppendorf 5415D; Eppendorf AG, Hamburg, Germany). Two hundred microlitres of the supernatant were recovered with a pipette, while carefully avoiding aspiration of any pelleted material. The final sample was diluted in 0.15 M phosphate-buffered saline (PBS, pH 7.2, final dilutions of 1:2 to 1:10 were used) and analysed using DRG-Diagnostics corticosterone (competitive) ELISA (EIA-4164; DRG Instruments GmbH, Maburg, Germany) according to the manufacturer's instructions. The following cross reactivities are reported for the assay: Progesterone (7.4%), deoxycorticosterone (3.4%), 11-dehydrocorticosterone (1.6%), cortisol (0.3%), pregnenolone (0.3%), other steroids (<0.1%). The analytical sensitivity is reported as being less than 1.6 nmol/l. The absorbencies of the sample solutions were recorded at 450 nm (reference wavelength, 650 nm) using a Thermo Multiskan Ex microplate reader (Thermo Fisher Scientific Inc., Waltham, USA). Results are presented as concentrations of corticosterone in μg corticosterone day−1× kg body weight−1. The term ‘corticosterone and immunoreactive corticosterone metabolites’ is frequently employed and may be a more correct denomination; it is however less transparent and no more informative, hence we opted for the less formal terminology.
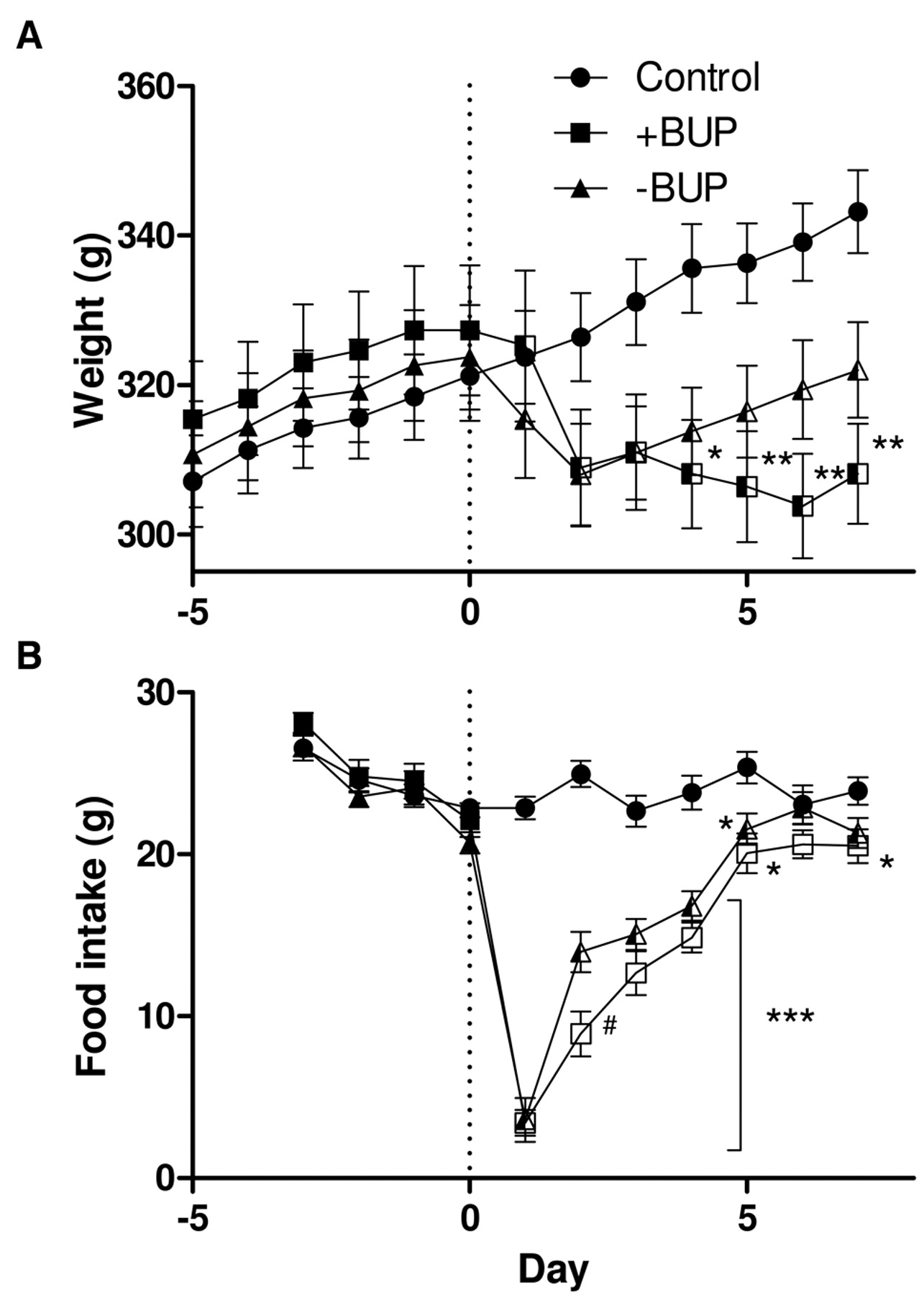
Body weight (a) and food intake (b) of animals. Bars display means±SEM. Significantly different from the control group at a level of *p<0.05, **p<0.01 and ***p<0.001, respectively, determined using one-way ANOVA with Tukey's post hoc. #Significantly different at p<0.05 from the non-treated group (-BUP). Semi-filled symbols indicate groups that differ significantly (p<0.05) in the postsurgical period from the control group using GLM, whereas non-filled symbols indicate groups that differ significantly from both other groups.
Histology. Seven days postsurgery, the animals were anaesthetised (5% isoflurane in 2:1 N2O/O2) and euthanased through exsanguination. The brains were removed, immediately frozen in iso-pentane (Merck, Darmstadt, Germany) and stored at −80°C until further examination. At 100 μm intervals, 10 μm-thick coronal slices through the dorsal hippocampus were cut (Leitz, Kryostat 1720 Digital) and stained with haematoxylin and eosin. The degree of hippocampal damage was scored independently by two researchers on the four-degree scale introduced by Bonfils et al. (24), ranging from 0 (‘no ischaemic damage’) to 3 (‘severe ischaemic damage’). Only sections found to encompass the CA1 pyramidal neurons were scored as this region is known to be most affected by short-term ischaemia (25). From a methodological viewpoint, a less affected area could have been more useful to score, in order to discern small changes. This type of induced ischaemia, however, is known to produce highly localised damage, therefore, this would not have been practically applicable. The scores were based on the degree of eosinophilia, fragmentation, and interrupted architecture of the neurons, as well as the infiltration of rodshaped macrophages. A final consensus score for each animal was calculated as an average value of the ischaemia scores.

Body temperature (a) and faecal corticosterone excretion (b) of the animals. Bars display means±SEM. Significantly different from the control group at a level of *p<0.05, **p<0.01 and ***p<0.001, respectively, determined using one-way ANOVA with Tukey's post hoc. ##Significantly different at p<0.01 from the -BUP group. Non-filled symbols indicate that the group differed significantly (p<0.05) from both other groups in the postsurgical period when analysed using GLM.
Statistical analysis. Physiological data were analysed using a one-way ANOVA with Tukey's post hoc test. Data are presented as F(df1,df2), where ‘df1’ and ‘df2’ are the degrees of freedom between and within the groups, and post hoc results are given in the form of a Student's p-value. The whole postsurgical period was further analysed using a univariate general linear model (GLM) with Tukey's post hoc test, factoring in the effect of time (as the cerebral damage progresses, the effect on pain and distress is expected to vary) and the type of treatment. Since stress responses and HPA axis activation are highly individual, the homogeneity of the corticosterone data was analysed using Levene's test in conjunction with the GLM. Data are presented as F(df1,df2) and a Student's p-value. This was followed by comparing the coefficients of variation between the two ischemic groups with a Fisher's F test. Data are again presented as F(df1,df2) and a Student's p-value. Statistical significance for all tests was set at the level of p<0.05. Statistical analyses were carried out in PASW Statistics v.18 (SPSS Inc, Chicago, IL USA).

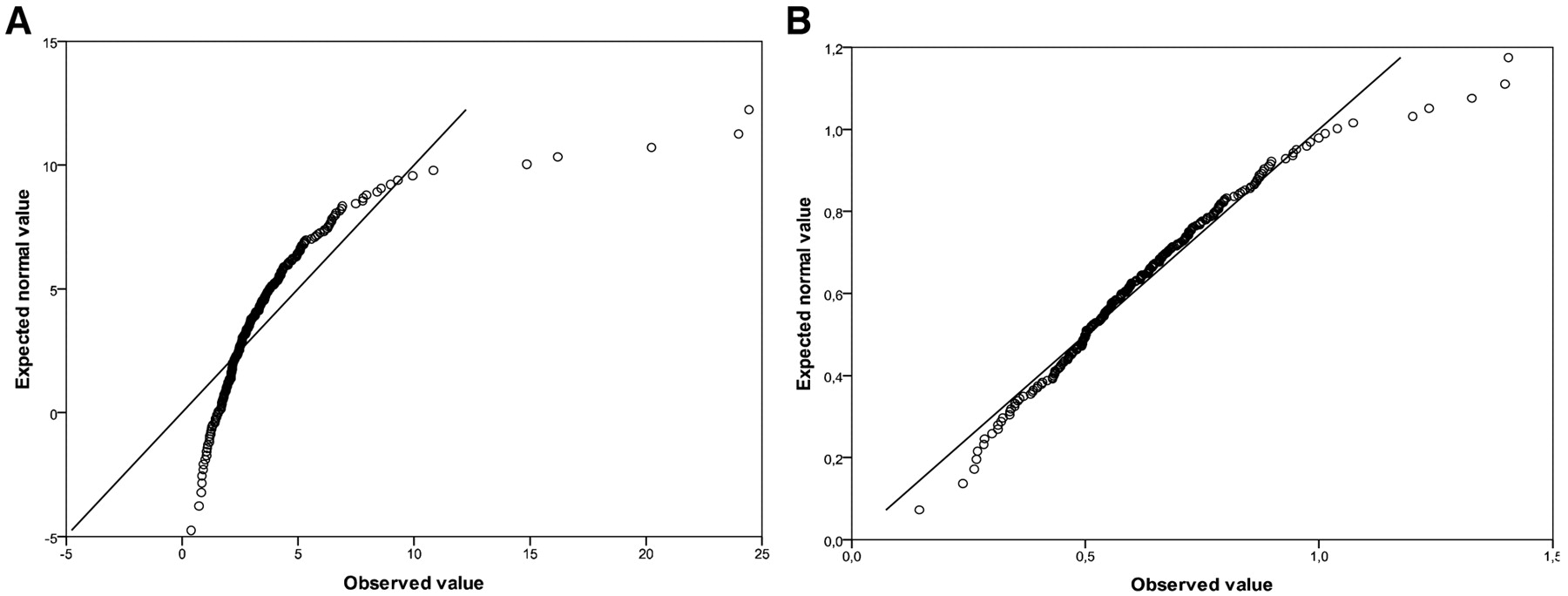
Q-Q plots of corticosterone data versus an ideal normal distribution prior to (a) and after (b) log-transformation (Y′=log10(Y+1)). Note that data from a perfectly normal distributed population will conform along the diagonal.
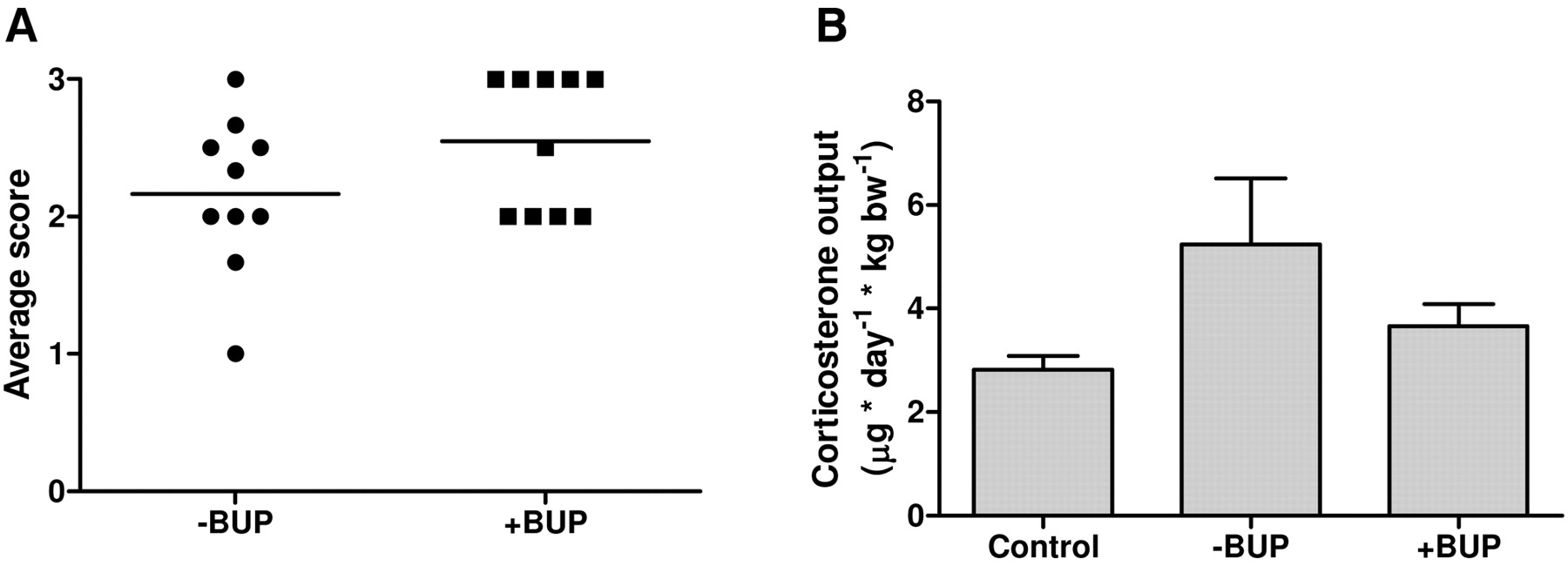
Ischaemia scores (a) and post surgical corticosterone outputs (b) in group-wise comparison. The horizontal bars in the left-hand figure represent the average scores. Scores for the control group (all 0) are not shown. The corticosterone outputs are presented as means+SEM. No significant differences were found.
Results
Physiological data. No animals were excluded from the study as none of the rats displayed morbid changes in their postoperative behaviour. Food intake and average animal body weights are shown in Figure 1. When studying the postsurgical period using univariate GLM, the rats of both ischaemic groups had a significantly lower body weight than the control rats (F(2)=23.6, p<5×10−5) but the analgesic treatment had no significant effect (p=0.36). Isolated using one-way ANOVA, however, the buprenorphine-treated animals appeared to have significantly lower body weight on days 4-7 (F(2,27)>5, p<0.05), unlike the untreated animals. The surgery had a significant negative impact on the food consumption of the rats when compared to control rats (F(2)=12.2, p<10−8). The animals treated with buprenorphine consumed less food than did the untreated animals (Tukey's post hoc: p<0.005). Water consumption remained constant for all animals throughout the experiment (data not shown).
The average body temperatures and postsurgical corticosterone outputs are shown in Figure 2. Hyperthermia was recorded for the first four days following surgery in both groups of ischaemic rats. On day 2, the body temperature of the rats treated with buprenorphine was significantly higher than that of the non-treated rats (one-way ANOVA with Tukey's post hoc: F(2,27)=25.8, p<0.005). The corticosterone data violated the criteria of normality (Levene's test: F(20,188)=1.84, p<0.05). Furthermore, the non-treated animals displayed a higher variance in their corticosterone excretion when compared to the treated animals (Fisher's test: F(69,69)=1.71, p<0.05). In order to proceed with parametric testing the corticosterone data was log-transformed (Y′=log10(Y+1)) and a conformity to log-normal distribution was confirmed (Figure 3). The corticosterone excretion was significantly higher in the rats of the non-treated group on the first day post-surgery (one-way ANOVA of log-transformed data: F(2,27)=5.48, Tukey's: p<0.05). During the entire postsurgical period, using univariate GLM, the corticosterone excretion in the non-treated animals was significantly higher than that in both control rats (F(2)=12.4, Tukey's: p<10−6) and treated animals (Tukey's: p<0.05). No significant difference was found between the treated group and the control group using Tukey's post hoc (p=0.076).
Histology. There was no significant difference between the degrees of ischaemia in the two experimental groups. While all the rats in the control group had scores of 0, i.e. no ischaemia, the rats in the two experimental groups had scores of 2 or 3, indicating moderate to severe ischaemia. No correlation was found between ischaemia scores and faecal corticosterone output for the individual animals, nor in a group-wise comparison (Figure 4).
Discussion
Assessment of pain and distress in rats subjected to surgically induced ischaemic brain damage is complicated because the animals are not only subjected to anaesthesia and surgery, but the induced model may also be associated with pain and distress. In the present study, we aimed to distinguish between symptoms and discomforts associated with the preceding anaesthesia and surgery, which can be alleviated, and those which are a consequence of the brain damage and therefore more difficult to treat. This study indicates that the stress perceived by the animals can be alleviated to some extent through perioperative analgesic treatment, without inflicting unwanted effects on the intended experimental brain damage.
Faecal glucocorticoid output provided a fairly sensitive measure for evaluating the postsurgical stress state of the animals. A significantly lower faecal corticosterone output was measured on the first day post surgery in the buprenorphine-treated group when compared to the non-treated group. Furthermore, in the entire postsurgical period, the animals given analgesia retained a significantly lower HPA axis activity than did animals not receiving analgesia. This suggests that the analgesic treatment alleviated the stress of the anaesthesia and surgical procedure. More importantly from a disease model point of view, the buprenorphine treatment reduced the between-animal variation. This is desirable as fluctuations in corticosterone have far reaching metabolic consequences. Reducing the between-animal variation in circulating corticosterone results in a closer similarity between animals in a multitude of endogenous parameters. Experimental group sizes can thus be reduced, which is desirable when working with laboratory animals.
Hyperthermia was recorded in all animals subjected to surgery. The hyperthermia of the non-treated animals was less pronounced on day 2 in the postsurgical period than in the treated animals. This is most likely a consequence of the higher corticosterone levels of these animals, corticosterone being a potent anti-inflammatory agent (26). The duration of the hyperthermia was, however, four days for both ischaemic groups.
On day 3, animals of both experimental groups exhibited a faecal corticosterone excretion on par with that of the control animals, with very little variance displayed in the groups. This is probably due to a recovery from surgery and consequently a return to baseline levels of corticosterone, which is in agreement with our earlier findings (7, 18). The subsequent rise in corticosterone output, to early postsurgical levels, in both ischaemic groups starting on day 4 coincided with the inflammatory reaction in the infarcted CA1 characterized by massive invasion of rod-shaped macrophages from the blood vessels, especially from those located in the hippocampal fissure (27, 28).
A common adverse effect of the buprenorphine treatment was recorded in food intake and body weight of the animals. The buprenorphine-treated animals consumed less diet and lost more body weight than did untreated animals. This effect is generally agreed to be the result of loss of appetite or metabolic alterations brought on by the opioid (29). The weight loss seen in this experiment was not pathological and was expected to be transient.
Since the extent of cerebral damage in two animals brought on by the same induction procedure varies widely (30), it was important to quantify the infarction of the individual animals. This should give a basis on which to distinguish the effects of the analgesic treatment from those that arise naturally from the great individual variance. No correlation could, however, be found between treatment or corticosterone levels and the degree of ischaemia, nor did the extent of ischaemia between the two experimental groups differ.
Buprenorphine treatment, as administered in the present study, thus seems to have little or no effect on the global ischaemia model itself. The slightly greater decrease in body weight and activity level and slightly higher hyperthermia on day 2 should be of little consequence to a model primarily developed to study neuronal damage. Even though cortico-sterone has been implicated in modulating the extent of ischaemic damage (11-13), no such correlation was found in the present study. For further studies using models where activation of the HPA axis is undesirable, the advantage of proper use of analgesia is obvious.
In summary, the use of appropriate analgesia administered non-invasively is to be recommended; in particular because rats treated with buprenorphine showed a significantly lower and less varied activation of the HPA axis in the period following the surgery, without interfering with the desired development of cerebral damage. Ensuring undisturbed HPA axis activity will assist in minimizing confounding stress associated variables when utilising the model, and is beneficial to the animals from an animal welfare point of view.
Acknowledgements
This study was generously supported by the Danish Research Council. The Authors thank Lisbeth Thatt, Anne-Marie Karnøe, Micael Lønstrup and Elisabeth Nyborg for their invaluable assistance.
- Received March 22, 2010.
- Revision received June 23, 2010.
- Accepted July 2, 2010.
- Copyright © 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue




{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Transdermal Fentanyl Solution Provides Long-term Analgesia in the Hind-paw Incisional Model of Postoperative Pain in Male Rats
- Implementation of a Functional Observation Battery for the Assessment of Postoperative Well-being in Rats Subjected to Fimbria-Fornix Transection
- The Utility of Fecal Corticosterone Metabolites and Animal Welfare Assessment Protocols as Predictive Parameters of Tumor Development and Animal Welfare in a Murine Xenograft Model
- Quantitative Effects of Diet on Fecal Corticosterone Metabolites in Two Strains of Laboratory Mice
- Post-operative Corticosterone Levels in Plasma and Feces of Mice Subjected to Permanent Catheterization and Automated Blood Sampling