Article Text

Abstract
Background Primary cytoreductive surgery followed by chemotherapy has been considered standard management for patients with advanced ovarian cancer over decades. An alternative approach of interval debulking surgery following neoadjuvant chemotherapy was subsequently reported by two randomized phase III trials (EORTC‐GCG, CHORUS), which were criticized owing to important limitations, especially regarding the rate of complete resection.
Primary Objective To clarify the optimal timing of surgical therapy in advanced ovarian cancer.
Study Hypothesis Primary cytoreductive surgery is superior to interval cytoreductive surgery following neoadjuvant chemotherapy for overall survival in patients with advanced ovarian cancer.
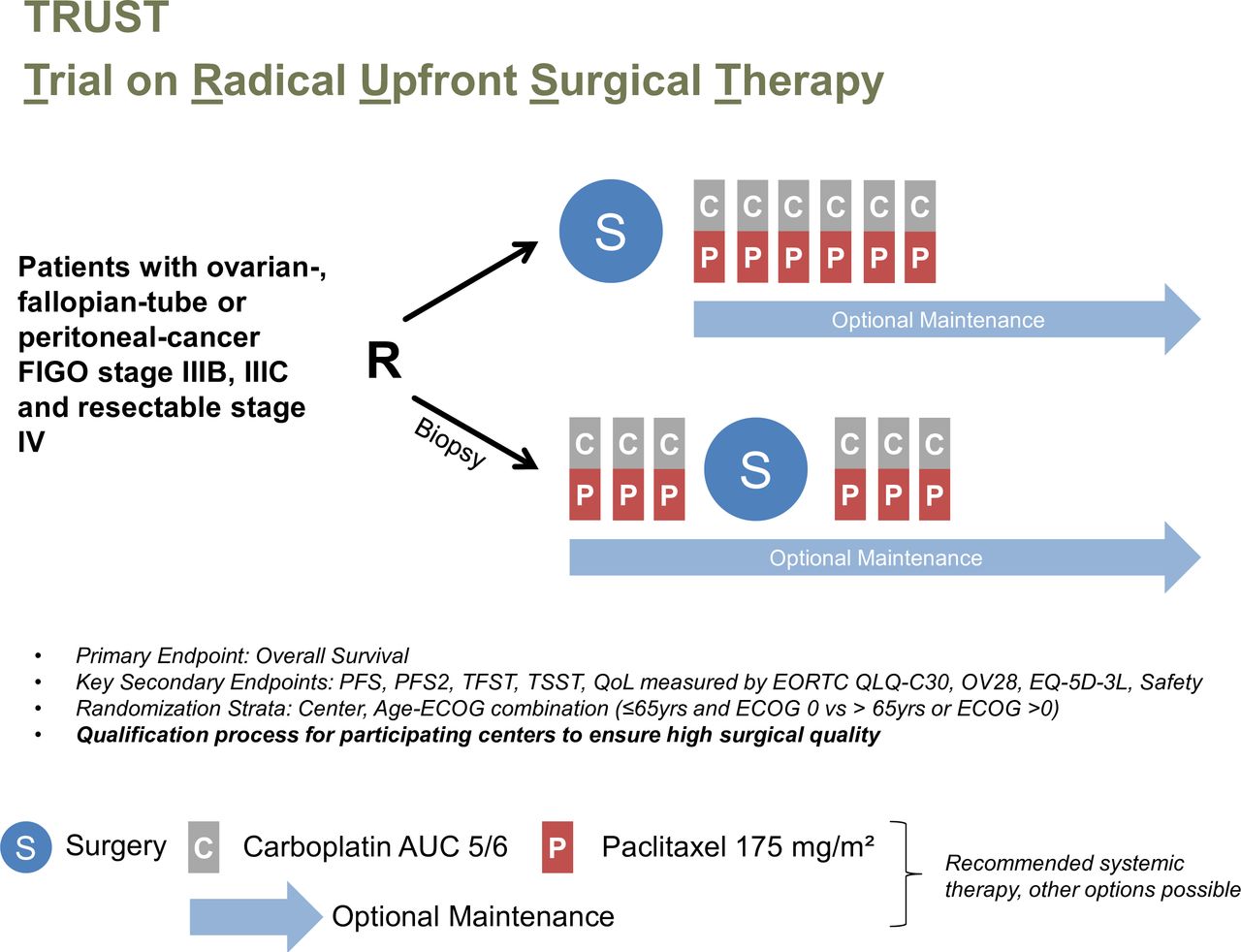
Trial Design TRUST is an international open, randomized, controlled multi-center trial investigating overall survival after primary cytoreductive surgery versus neoadjuvant chemotherapy and subsequent interval cytoreductive surgery in patients with FIGO stage IIIB–IVB ovarian, tubal, and peritoneal carcinoma. To guarantee adequate surgical quality, participating centers need to fulfill specific quality assurance criteria (eg, ≥50% complete resection rate in upfront surgery for FIGO IIIB–IVB patients, ≥36 debulking-surgeries/year) and agree to independent audits by TRUST quality committee delegates. Patients in the primary cytoreductive surgery arm undergo surgery followed by 6 cycles of platinum-based chemotherapy, whereas patients in the interval cytoreductive surgery arm undergo 3 cycles of neoadjuvant chemotherapy after histologic confirmation of the disease, followed by interval cytoreductive surgery and subsequently, 3 cycles of platinum-based chemotherapy. The intention of surgery for both groups is complete tumor resection according to guideline recommendations.
Major Inclusion/Exclusion Criteria Major inclusion criteria are suspected or histologically confirmed, newly diagnosed invasive epithelial ovarian cancer, fallopian tube carcinoma, or primary peritoneal carcinoma FIGO stage IIIB–IVB (IV only if resectable metastasis). Major exclusion criteria are non-epithelial ovarian malignancies and borderline tumors; prior chemotherapy for ovarian cancer; or abdominal/pelvic radiotherapy.
Primary Endpoint Overall survival.
Sample Size 772 patients.
Estimated Dates for Completing Accrual and Presenting Results Accrual completion approximately mid-2019, results are expected after 5 years' follow-up in 2024.
Trial Registration NCT02828618.
- interval debulking surgery
- neoadjuvant chemotherapy
- ovarian cancer
- primary debulking surgery
Statistics from Altmetric.com
INTRODUCTION
Ovarian cancer is the leading cause of death from gynecological malignancies and is in most cases diagnosed at an advanced stage. Despite optimal therapy consisting of surgery and platinum/taxane-based chemotherapy about half of the patients will die within 5 years after the first diagnosis.1 In 1934, Meigs was the first to perform cytoreductive surgery in advanced ovarian cancer to enhance the effects of post-operative radiation therapy.2 The concept of primary cytoreduction was supported when Griffiths showed that survival depends on residual disease.3 Since then, many other authors have confirmed this observation.4 5 Residual disease after surgery is (apart from the type of systemic therapy) the only prognostic factor which can be influenced by the treating physician. Cytoreductive surgery to achieve complete resection consists of at least bilateral salpingo-oophorectomy, hysterectomy, and omentectomy, but can also include additional surgical procedures like bowel surgery and upper abdominal surgery as well as lymphadenectomy depending on the dissemination patterns of the tumor.
The standard management of patients with advanced ovarian cancer has been primary cytoreductive surgery followed by chemotherapy for the past decades. Although the data in support of optimal cytoreduction are almost all from retrospective analyses, the consistency of the observation of improved patient outcome with more extensive surgical debulking has led to the primary aim of tumor cytoreduction leaving no macroscopic disease visible after surgery.
An alternative to the standard approach of attempted primary cytoreductive surgery followed by chemotherapy was reported by the European Organization for Research and Treatment of Cancer-Gynecologic Cancer Group (EORTC-GCG) and the National Cancer Institute of Canada (NCIC) Clinical Trials Group.6 In this trial, patients with stage IIIC or IV ovarian cancer were randomized to primary debulking surgery followed by platinum-based chemotherapy or to neoadjuvant platinum-based chemotherapy followed by interval debulking surgery and post-operative platinum-based chemotherapy. After debulking surgery, the rate of complete tumor resection was 19.4% in patients in the primary cytoreductive surgery arm, and 51.2% in the neoadjuvant chemotherapy arm. The progression-free and overall survival were practically the same in the two arms. Complete resection of all macroscopic disease, at primary cytoreductive surgery or after neoadjuvant chemotherapy, was the strongest independent variable in predicting overall survival. However, despite the reported 51.2% complete cytoreduction rate in the neoadjuvant chemotherapy arm, the progression-free and overall survival reported in this trial were low and similar to survival data reported in previous studies of sub-optimally debulked patients. More recently, a second randomized phase III trial comparing primary cytoreductive surgery followed by platinum-based chemotherapy with neoadjuvant chemotherapy and interval cytoreductive surgery was reported by the National Cancer Research Institute (NCRI) Gynecological Cancer Studies Group.7 This trial had a comparable design to the previous study but also included patients with stage IIIB disease. After debulking surgery, the rates of complete tumor resection were 17% in patients in the primary cytoreductive surgery arm, and 39% in the neoadjuvant chemotherapy arm. Again, progression-free and overall survival were similar between the two arms and very low compared with that of other studies.5
Owing to the limitations of these studies, the question whether primary debulking surgery or neoadjuvant therapy with interval debulking should be the standard approach for patients with advanced ovarian cancer remains open. Some gynecologic oncologists feel that the poor survival rates invalidate the findings of the two studies, but many are now changing their practice owing to these findings and are offering neoadjuvant chemotherapy in lieu of attempted primary cytoreduction. Although progression-free and overall survival for the neoadjuvant chemotherapy arm are consistent with those in other neoadjuvant studies in the literature, the survival outcomes in the primary cytoreductive surgery arm are alarmingly low. These low survival rates have three potential causes: (1) patient selection, with only the patients with most advanced disease being enrolled; (2) surgery was substandard compared with that in other trials; and/or (3) surgical cytoreduction, no matter what the residual disease, has no benefit on survival. The last possibility, that the extent of surgery was of insignificant clinical importance, is unlikely to be true given that complete resection of all macroscopic disease was the strongest independent variable in predicting overall survival in both arms. What contribution the other two possibilities made to the poor survival rates in the primary cytoreductive surgery arm cannot be adequately determined.
Both previous studies share one major problem that potentially invalidates their findings: Since it has been shown by several studies and meta-analyses that complete cytoreduction with no residual disease after surgery is most beneficial for patients with advanced ovarian cancer, comparison of upfront surgical debulking with interval debulking needs to account for this factor. More precisely, the trial needs to compare complete tumor resection at upfront debulking with complete tumor resection at interval debulking. The rate of complete gross resection at primary surgery in both trials was very low (19% and 17%). In other words, the factor necessary for the evaluation was only present in <20% of the study population. In surgically specialized gynecologic cancer centers, the rate of complete resection in unselected patients with advanced-stage ovarian cancer ranges between 50% and 70%.8 9 Furthermore, the debate about selection and identification of optimal surgical candidates is still open and no well-established factors have yet been defined.10
Therefore, we started the TRUST trial focusing on patients for whom complete resection at primary cytoreductive surgery seems feasible and who are treated in surgically qualified centers.
METHODS
Trial Design
This is an open, phase III, randomized, controlled multi-center trial. All patients will be registered on site, and eligible patients will undergo randomization to primary cytoreductive surgery or three cycles of neoadjuvant chemotherapy followed by interval cytoreductive surgery (Figure 1). Both randomized groups will be treated with surgery for complete cytoreduction according to current guideline recommendations.11 Surgery will be performed by mid-line laparotomy and will include hysterectomy, bilateral salpingo-oophorectomy, omentectomy, as well as peritonectomy, when necessary, and (partial) resection of all affected organs—for example, small or large bowel, spleen, pancreas, urinary tract, etc, as well as pelvic and para-aortic lymphadenectomy in the presence of bulky lymph nodes.12 Patients with significant pleural effusion (>500 mL in the right chest or any pleural effusion in the left chest, assessed either through ultrasound or CT) need to undergo video-assisted thoracoscopy or open assessment of the pleura before or during debulking surgery to detect and, if possible, remove any intra-thoracic disease.
{kind=link}
Study schema of TRUST.
Patients allocated to the primary debulking group will undergo surgery followed by six cycles of platinum and taxane-based chemotherapy after having recovered from surgery.13 Recommended systemic treatments are
Participation in a prospective randomized trial, as long as participation is possible in either arm of the current study.
Carboplatin area under the curve 5–6/paclitaxel 175 mg/m² every 21 days/bevacizumab 15 mg/kg every 21 days, six cycles followed by bevacizumab maintenance therapy for a total of 15 months or until disease progression.
Carboplatin area under the curve 5–6/paclitaxel 175 mg/m² every 21 days, six cycles. Substitution of paclitaxel by docetaxel (75 mg/m²) is possible in case of contraindications to paclitaxel. Maintenance/consolidation therapy inside prospective trials or according to national standard treatments is allowed, as long as both arms of the TRUST trial are eligible. Additional treatment outside prospective studies is not recommended.
Carboplatin area under the curve 5–6, every 21 days, six cycles if contraindications to combination chemotherapy.
Patients allocated to the interval debulking surgery group will undergo biopsy to confirm epithelial ovarian cancer and then three cycles of neoadjuvant pre-operative platinum and taxane-based chemotherapy. Then interval debulking surgery is performed followed by three cycles of postoperative platinum and taxane-based chemotherapy. The following treatments are recommended for neoadjuvant chemotherapy:
Participation in a prospective randomized trial, as long as participation is possible in either arm of the current study.
Carboplatin area under the curve 5–6/paclitaxel 175 mg/m² every 21 days, three cycles. Substitution of paclitaxel by docetaxel (75 mg/m²) is possible in case of contraindications to paclitaxel.
Carboplatin area under the curve 5–6, every 21 days, three cycles if contraindications to combination chemotherapy.
It is recommended that post-operative chemotherapy is started after sufficient recovery from interval debulking surgery, ideally 2–6 weeks post-operatively. The following treatments are recommended:
Participation in a prospective randomized trial, as long as randomization is possible in either arm of the current study.
Carboplatin area under the curve 5–6/paclitaxel 175 mg/m² every 21 days / bevacizumab 15 mg/KG every 21 days, 3 cycles followed by bevacizumab maintenance therapy for a total of 15 months or until disease progression.
Carboplatin area under the curve 5–6/paclitaxel 175 mg/m² every 21 days, three cycles. Substitution of paclitaxel by docetaxel (75 mg/m²) is possible in case of contraindications to paclitaxel. Maintenance/consolidation therapy inside prospective trials or according to national standard treatments is allowed. Additional treatment outside prospective studies is not recommended.
Carboplatin area under the curve 5–6, every 21 days, three cycles if contraindications to combination chemotherapy.
The investigator is responsible for the performance and completion of systemic therapy. The above-stated regimens and dosages are mainly recommendations. Other regimens are possible after consultation with the principal investigator as long as they are applied equally in both treatment arms.
The setting of the trial is tertiary gynecological cancer centers. Currently, 20 centers from Germany, Italy, the United Kingdom, France, United States of America, Sweden, Denmark, and Austria have recruited patients.
In order to establish and ascertain adequate surgical quality, participating sites must meet the following eligibility criteria: at least 50% complete resection rate in upfront surgery for International Federation of Gynecology and Obstetrics (FIGO) stage IIIB–IVB patients; at least 36 debulking surgeries/year; undergo review of 24 surgery and pathology reports from the year preceding participation (upper abdominal and retro-peritoneal surgery must be established as well as morbidity and mortality auditing); centers must consent to be visited and audited by TRUST quality committee delegates.
The trial is supported through internal resources of the AGO study group and in parts by Roche and Astra Zeneca. The trial has been registered with the ethics committee of the medical faculty at Ludwig-Maximilians-University Munich and at clinicaltrials.gov (NCT02828618).
Participants
Major inclusion criteria are suspected or histologically confirmed, newly diagnosed invasive epithelial ovarian cancer FIGO stage IIIB–IVB (IV only if potentially resectable metastases); age ≥18 years; written informed consent provided; Eastern Cooperative Oncology Group (ECOG) performance status 0 or 1; American Society of Anesthesiologists (ASA) score 1 or 2 (ASA 3 only if ECOG 0); preoperative CA125/CEA ratio ≥25 (if CA125 above twice the upper limit of normal); patients ability to tolerate the procedures necessary to achieve a complete tumor resection, as assessed by an experienced surgeon.
Major exclusion criteria are non-epithelial ovarian malignancies and borderline tumors; secondary invasive neoplasms in the past 5 years (except synchronous endometrial carcinoma, non-melanoma skin cancer, breast cancer N0M0 without any sign of relapse or activity for 5 years); recurrent ovarian cancer; prior abdominal/pelvic radiotherapy; any significant medical co-morbidities, age, or performance status that will not allow the study procedures to be performed (estimation of investigator); pregnancy; dementia or significantly altered mental status that would prohibit the understanding and giving of informed consent; any reasons interfering with regular follow-up.
All patients with histologically/cytologically confirmed advanced ovarian cancer or where there are suspicions of advanced-stage disease can undergo screening for this trial and are documented in a screening log after their informed consent has been obtained.
Outcomes
The primary study objective is to assess the efficacy for overall survival of primary surgery compared with interval debulking surgery in patients with advanced ovarian cancer. Secondary objectives are the safety of complete tumor resection at primary surgery compared with interval debulking surgery (including diagnostic procedures) and the effect of primary or interval debulking surgery on progression-free survival, quality of life, and surgical morbidity. To monitor patient safety and supervise the progress of the TRUST trial an independent data monitoring committee has been established.
Randomization and Blinding
Randomization uses list randomization with variable block lengths and is stratified by center, age–ECOG combination (ECOG 0 and age up to 65 years vs ECOG >0 or age ≥66 years). After verification of eligibility criteria, patients are randomized to primary cytoreductive surgery or neoadjuvant chemotherapy with interval cytoreductive surgery in a 1:1 proportion centrally by fax at the Co-ordinating Center for Clinical Trials (KKS) Marburg, Germany (Figure 1). The data of the patients are documented remotely with an electronic data capture system which is hosted at KKS Marburg.
Blinding is not feasible since the timing of surgical intervention cannot be withheld from the patient and treating physicians.
Statistical Methods
The primary endpoint is overall survival. Secondary endpoints are: progression-free survival; time until second progression or death; time to first and second subsequent anti-cancer therapy or death; quality of life as measured by EORTC QLQ-C30 and OV28, EQ-5D-3L, and safety. All time to event endpoints are calculated from the date of randomization until the event of interest. Progressive disease is defined as clinically or imaging-detected tumor progression or death in cases without prior documented tumor progression.
The primary analysis will use the modified intention-to-treat population, which consists of all randomized patients, excluding those with early stage or inadequate histology (benign, or non epithelial malignancy, or different primary). The full intention-to-treat population will be used for sensitivity analyses.
Overall survival will be compared between treatment groups by a two-sided stratified log rank test with significance level 0.05 after 380 events have been observed in patients eligible for the modified intention-to-treat population. Stratification will be used to adjust for randomization strata. Additionally, Kaplan-Meier estimates for the distribution of overall survival in each treatment group and a point estimate and 95% CI of the HR between treatment groups will be given.
Sample Size
For power and sample size calculation, a HR of 0.75 (corresponding to a prolongation of median survival from 45 months in the interval cytoreductive surgery arm to 60 months in the primary cytoreductive surgery arm as observed in previous trials),14 is considered clinically relevant. With an assumed accrual period of 2 years, a follow-up of at least 5 years for each patient, 380 events obtain a power of 80%. With the given accrual and follow-up periods and accounting for a 20% drop-out rate, a total of 772 evaluable patients should be randomized. The estimated drop-out rate is set at 20% as randomization will be done before histologic confirmation in the majority of patients. This reflects also the potential recruitment of patients with other tumor entities than ovarian cancer or patients with an early stage ovarian cancer. The drop-out rate also accounts for losses to follow-up.
DISCUSSION
The optimal strategy in patients with advanced ovarian cancer is still an open debate and topic of controversy worldwide, as reflected also by the strongly varying practices nationally and internationally. Previous trials of the value of interval cytoreductive surgery have mainly included patients in whom it was not possible to achieve a complete resection, either owing to patient- or tumor-related factors or owing to sub-optimal surgical effort, as shown by the limited rates of complete resection. Nevertheless, the concept of neoadjuvant chemotherapy has been transferred to many patients with advanced ovarian cancer, irrespective of their performance status and operability and also regardless of the expertise, training, and quality of the surgical team. Since neoadjuvant chemotherapy has repeatedly been applied in the past to compensate for sub-optimal surgical training, as surgical procedures at interval cytoreductive surgery are often more limited, we wanted to make sure in the present trial that this bias was eliminated. Therefore, our first important step was to include a qualification process to be sure that only centers were included in which surgical expertise was well established and hence would not represent a limiting factor. Defined surgical eligibility criteria are of high importance for surgical trials to be accepted within the gynecologic oncology community, as shown in the LION trial12 or LACC trial.15 Therefore, we hope that the results of the TRUST trial will answer important open questions about the optimal timing of debulking surgery in patients with advanced ovarian cancer.
References
Footnotes
Contributors Substantial contributions to the conception or design: all authors. Drafting the work or revising it critically for important intellectual content: all authors. Final approval of the version published: all authors. Agreement to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved: all authors.
Funding The trial is supported through internal resources of the AGO study group and in parts by Roche and Astra Zeneca.
Competing interests AdB reports personal fees from Roche, Astra Zeneca, BIOCAD, Genmab, Clovis, Tesaro, PharmaMar, Pfizer, outside the submitted work. PH reports grants and personal fees from Astra Zeneca, Roche, Tesaro, Public funding (ASCO, DKH, DFG), personal fees from Sotio, Stryker, Zai Lab, MSD, Clovis, Immunogen, grants from GSK, Boehringer Ingelheim, Medac, Genmab, outside the submitted work. CF reports personal fees from Roche, Tesaro, Astra Zeneca, Olympus, Ethicon, outside the submitted work. A Reinthaller reports research grants from Roche; honoraria as a speaker and for advisory boards from Amgen, Astra Zeneca, MSD, PharmaMar, Roche, Tesaro, Vifor Pharma; travel expenses from Amgen, Astra Zeneca, PharmaMar, Roche, Tesaro. FH reports personal fees from Astra Zeneca, Roche, PharmaMar, Tesaro, Clovis, outside the submitted work. DSC reports personal fees from Bovie Medical Co., Verthermia Inc. (now Apyx Medical Corp.), C Surgeries, Biom ‘Up, other from Intuitive Surgical, Inc., TransEnterix, Inc., outside the submitted work. SM reports grants and personal fees from AstraZeneca, Medac, MSD, PharmaMar, Roche, Tesaro, Teva, personal fees from Clovis, Novartis, Olympus Europa, Sensor Kinesis, outside the submitted work.
Patient consent for publication Not required.
Provenance and peer review Commissioned; internally peer reviewed.