Article Text

Abstract
Objectives: To evaluate the microscopic epithelial features seen with in vivo confocal microscopy (IVCM) of bulbar conjunctiva in glaucomatous patients undergoing trabeculectomy with mitomycin C in order to elucidate modifications.
Methods: Fifteen eyes of 15 consecutive Caucasian patients affected with primary open-angle glaucoma (POAG) undergoing trabeculectomy and 10 eyes of 10 glaucomatous patients (controls) under medical therapy were enrolled. Eyes were examined using a digital confocal laser-scanning microscope (HRT II Rostock Cornea Module) at baseline and after 6 weeks. The mean microcyst density (MMD: cysts/mm2) and microcyst area (MMA: μm2) were the main outcome measurements.
Results: Before surgery, the mean intraocular pressure (IOP) was 25.1 (SD 3.2) mm Hg. MMD and MMA were 22.4 (11.9) and 4696.0 (3608.1), respectively. After trabeculectomy, the mean IOP was 16.1 (1.7) mm Hg. A marked increase in both MMD and MMA, with values of 103.1 (22.6) and 29 489.3 (12 954.9), respectively, was observed. In the control group at baseline, the mean IOP was 15.7 (1.9) mm Hg, and the microcyst parameters did not differ from eyes undergoing filtering surgery. After 6 weeks, IOP and microcysts parameters did not show any significant modifications.
Conclusions: Conjunctival epithelial microcysts were demonstrable in glaucomatous eyes under medical therapy prior to trabeculectomy. The filtering procedure increased microcysts density and surface at bleb site indicating a marked postsurgical enhancement of aqueous filtration across conjunctiva.
Statistics from Altmetric.com
The basic mechanism of all filtering procedures is the creation of a fistula at the limbus which allows aqueous humour to drain from the anterior chamber, thereby circumventing pathological obstruction to outflow. The aqueous thereby flows directly or indirectly into subconjunctival spaces and subsequently removed by one or more mechanisms.1 2
Trabeculectomy is the most effective filtering surgical procedure for lowering intraocular pressure.3 The majority of successful trabeculectomy are characterised by an elevation of the conjunctiva at the surgical site, commonly referred to as a filtering bleb.
Currently, besides the standard clinical assessment,4 5 6 7 several morphological diagnostic methods such as laser scanning in vivo confocal microscopy (IVCM) and anterior segment optical coherence tomography (AS-OCT) permit a precise analysis of the filtering bleb structure and function after glaucoma surgery by analysing the conjunctival and subconjunctival features.8 9 10 11
Several studies have investigated the ability of IVCM in the microscopic evaluation of the bleb tissue, analysing the drainage capability of the filtering blebs by assessing the presence of epithelial microcysts (defined as intraepithelial and extracellular optically empty spaces), the density of subepithelial connective tissue and the presence of blood vessels.
We recently reported the presence of epithelial microcysts within the conjunctiva either on eyes affected with untreated ocular hypertension or on medically treated glaucoma eyes.12 To date, to the best of our knowledge, the assessment and comparison before and after surgery of the features of conjunctiva at the site of trabeculectomy have not been reported. The aim of our study was to evaluate the microscopic epithelial features seen with IVCM of bulbar conjunctiva of glaucomatous patients undergoing trabeculectomy in order to elucidate modifications induced by surgery. Specifically, we compared the characteristics of the bulbar conjunctiva using IVCM in patients with glaucoma prior to and 1 month after trabeculectomy with an age- and gender-matched group of glaucoma patients who continued medical treatment.
Materials and methods
A comparative case series study was performed. The study adhered to the tenets of the Declaration of Helsinki, and informed consent was obtained from all patients prior to their enrolment. Our local Ethics Board was notified, and it was determined that their approval was not necessary.We examined 15 eyes (eight right and seven left eyes) of 15 consecutive Caucasian patients referred to the Ophthalmic Clinic of University Chieti-Pescara, Italy, 10 males and five females (mean (SD) age 64.5 (5.1) years; range 54–72) referred to the Ophthalmic Clinic of University Chieti-Pescara, Italy, affected with POAG and scheduled to undergo fornix-based flap trabeculectomy, performed as previously described.3
Inclusion criteria were as follows: uncontrolled IOP (⩾22 mm Hg, mean of three measurements at 09:00, 12:00 and 16:00) under maximal tolerated medical therapy, topical hypotensive therapy started at least 12 months before the day of IVCM examination and unmodified during the last 2 months, progression of glaucomatous damage confirmed on three consecutive SITA 30–2 visual field, use of mitomycin C (MMC) 0.2 mg/ml for 2 min applied on the sclera at the site and posterior to the site where the flap was outlined. The results of surgery were classified as success when a reduction of one-third of preoperative IOP without antiglaucoma treatment was achieved.13
Ten consecutive glaucomatous patients with open-angle glaucoma but with an acceptable target pressure with medical therapy, six males and four females (mean (SD) age 63.3 (4.1) years), were used as controls. Inclusion criteria were: IOP lower than 20 mm Hg with medical therapy unmodified in the last 6 months and no history of progression on visual-field examination (Humphrey 30–2 full threshold) during the last 12 months.
All eyes enrolled in the study showed a best-corrected visual acuity ⩾8/10, a refractive error ⩽4 dioptres (spherical equivalent) and a corneal pachymetry ranging from 530 to 560 μm. Overall exclusion criteria were: a history of ocular trauma, aphakia, previous trabeculoplasty or surgical procedure for glaucoma, uveitic glaucoma, contact lens wearing, the presence of any other ocular diseases in the last 12 months except open-angle glaucoma and end-stage glaucoma.
Each glaucomatous eye scheduled to undergo trabeculectomy and one eye randomly chosen in the control group were carefully examined using a digital confocal laser-scanning microscope (LSM) (HRT II Rostok Cornea Module, Heidelberg Engineering, Heidelberg, Germany) by a single operator masked for patient status (MN).
The technical characteristics of this instrument and the details of conjunctival examination were previously described.14 The confocal assessment of bulbar conjunctiva was performed at baseline for all enrolled eyes (1 week before trabeculectomy in eyes scheduled for surgical therapy).
Patients were seated in front of the microscope, with their head steadied with the aid of a headrest and with the eye properly aligned in order to obtain a tangential optical section of the superior bulbar conjunctiva. They were asked to follow a dedicated mobile bright red light provided with the instrument with the fellow eye. A digital camera provided a lateral view of the eye and objective lens in order to check the position of the objective lens on the surface of the eye for each scan. The LSM objective was positioned gently in contact with the ocular surface separated by a polymethyl methacrylate contact cap, and a drop of 0.2% polyacrylic gel (Viscotirs Gel, CIBA Vision Ophthalmics, Marcon, Venice) served as coupling medium. Sequential images 300×300 μm in size derived from automatic scans and manual frames were acquired for the upper bulbar conjunctiva at the intermediate layer (10 to 20 μm) of each examined eye, 2 mm from the limbus at the site of the planned trabeculectomy, in downward gaze. Results were reported as the average of six images selected by the IVCM operator (MN) in a masked fashion from about 40 images. For the IVCM assessment, we microscopically evaluated the bulbar conjunctiva on identifying epithelial microcysts, such as those reported in the conjunctival wall of functioning filtering blebs.8 9 10 11 The main parameters considered in the IVCM examination were the mean microcyst density (cysts/mm2) and the mean microcyst area (μm2). The surface area of epithelial microcysts was calculated using ImageJ, open source software (http://rsb.info.nih.gov/ij) as described elsewhere.9
Additionally, in order to verify the findings obtained in the sampled fields, we extended the analysis area to the whole conjunctival superior region (1.2×3 mm, approximately) in three eyes undergoing trabeculectomy and three control eyes. A planar reconstruction was thus obtained, permitting the evaluation of the distribution of epithelial microcysts. Final maps were obtained by juxtapositional acquisition of about 100 images by moving the cornea module from the nasal to temporal region (right and left side of the images, respectively) and from the limbus to the upper lid (bottom and top of the images, respectively).
The IVCM procedure was repeated in all eyes 6 weeks later.
The eyes that underwent surgical therapy initiated unpreserved topical steroids for 4 weeks (unpreserved dexamethasone 0.15% eye-drops four times a day for 2 weeks and three times daily for the following 2 weeks) and topical antibiotic for the initial 2 weeks (ofloxacin 0.3% fourfold daily). IVCM was repeated 5 weeks after trabeculectomy, that is 1 week after cessation of any topical therapy. During the study period, control eyes continued previous topical antiglaucoma therapy.
Statistical analysis was performed using SPSS Advanced Statistical 13.0 Software (SPSS, Chicago). Differences in trabeculectomy and control groups at baseline were evaluated using the Student t test and χ2 test, where appropriate. McNemar test was performed to compare the differences of mean microcyst density and area at baseline and at the end of the study in both groups. Data prior to transformation are reported, and a logarithmic transformation of mean microcyst density and area values was applied prior to statistical analysis in order to correct the wide sample data distribution.
Results
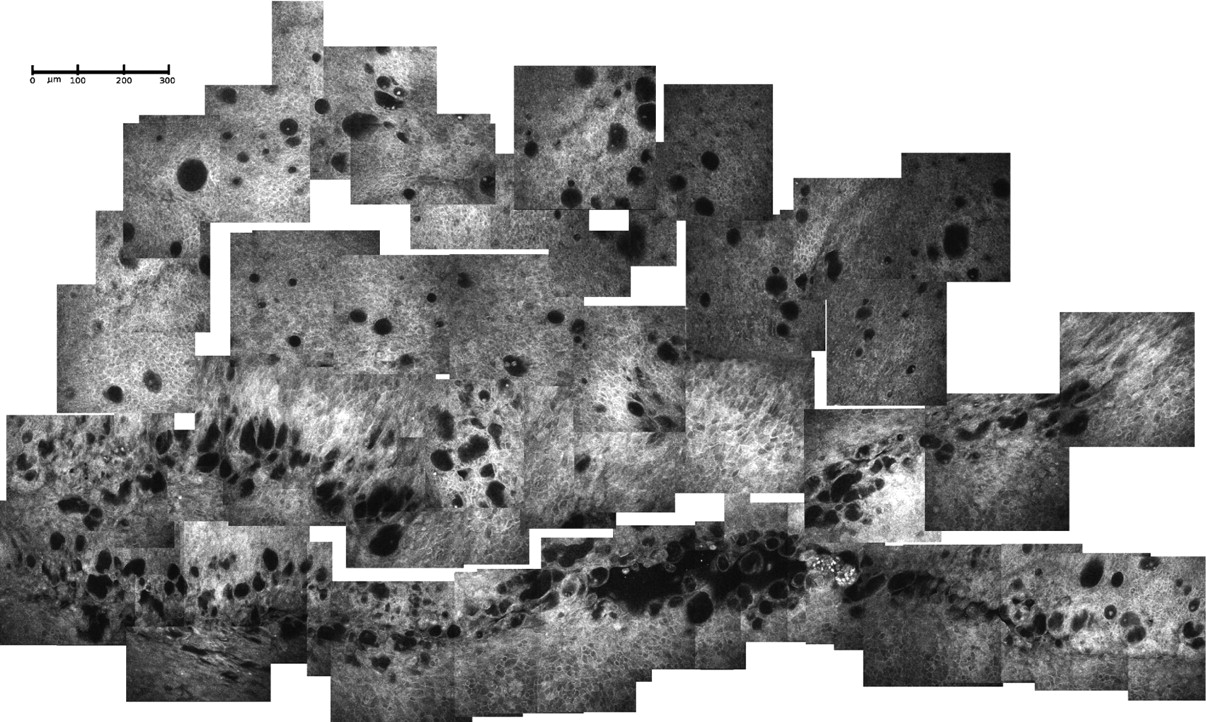
All the data are presented as mean (SD). The demographic and clinical data of each group at baseline are shown in table 1. Significant differences for age and sex were not observed. In the eyes scheduled to undergo trabeculectomy, the mean preoperative IOP was 25.1 (3.2) mm Hg with a median of three daily drugs per eye. Antiglaucomatous medication included betablockers (n = 15), prostaglandins (n = 15), brimonidine (n = 12) and carbonic anhydrase inhibitors (n = 8), in various combinations. At baseline, conjunctiva frequently showed irregular epithelial features, characterised by large and polygonal cells with low uniformity in size and shape and hyper-reflective borders. Epithelial microcysts were reported in all cases as structures optically clear, occasionally with features of round cells (presumably representing inflammatory cells) and amorphous material (probably representing proteinaceous debris)15 partially filling the inner space, often surrounded by a well-defined hyper-reflective and mildly thick wall (capsule), round or oval-shaped and differently sized. When observing the planar reconstruction of the superior bulbar conjunctiva compounded at baseline examination, we found a relatively homogeneous distribution pattern of microcysts with slight tendency towards clustering (fig 1). With regards to the main parameters analysed, we documented a mean microcyst density of 22.4 (11.9) cysts/mm2 and a mean microcyst area of 4696.0 (3608.1) μm2, expression of an evident and high interindividual variability.

Planar reconstruction of the superior bulbar conjunctiva in a glaucomatous eye undergoing trabeculectomy. Microcysts show a well-defined wall with round and hyper-reflective cells inside; the pattern of distribution appear homogeneous, with a poor clustering tendency.
Characteristics of the patients at baseline
No significant intra- and postoperative complications occurred, except for two cases of ocular hypotony and athalamia, resolved within 3 days without surgical treatment. In the postoperative period, no eyes received 5-fluororacyle injections, and topical therapy (antibiotic/steroid fixed combination) was discontinued after 4 weeks.
Five weeks after trabeculectomy and then 6 weeks after baseline, the mean IOP was 16.1 (1.7) mm Hg without medical therapy, and all the eyes were classified as a success, that is with a reduction of one-third of preoperative IOP (without medical therapy).
Clinical evaluation of the trabeculectomised eyes (Moorfields Bleb Grading System (MBGS) criteria)16 indicated a diffuse bleb pattern in all cases. IVCM examination of the conjunctiva showed different-shaped and sized microcysts, larger and less uniformly disposed than in the presurgical epithelium, surrounded by a low reflective and thinner wall, frequently with features of cohesion realising a multicluster distribution, more evident at the bleb site (fig 2). Also at this level, the inner space of the epithelial microcysts showed modifications, occasionally appearing filled with amorphous material and/or round cells, and sometimes also with amorphous material as found in the preoperative examination.

Planar reconstruction of the superior conjunctiva in a trabeculectomised eye. The bottom of the image represents the bleb site. Microcysts show a less uniform distribution, appearing oval-shaped, more abundant and clustered at bleb site, with features of a thin wall.
When analysing the microcysts characteristics, a mean density of 103.1 (22.6) cysts/mm2 and mean area of 29 489.3 (12 954.9) μm2 were observed. These parameters were statistically different and approximately fivefold higher than preoperative values (p = 0.003).
In the control group, the mean IOP was 15.7 (1.9) mm Hg, with a median of two daily drugs per eye, values statistically different (p<0.001) with respect to eyes undergoing trabeculectomy. Antiglaucomatous medication included betablockers (n = 9), prostaglandins (n = 7), brimonidine (n = 2) and carbonic anhydrase inhibitors (n = 1), in various combinations.
At baseline analysis, both epithelium or microcysts distribution and features appeared with the same characteristics described in patients undergoing filtering surgery, without any evident differences (fig 3).

Planar reconstruction of the superior bulbar conjunctiva in a glaucomatous eye under medical therapy, at baseline. Features and pattern of distribution of epithelial microcysts are similar to those reported and described in glaucomatous eyes undergoing filtering surgery, without any evident differences.
When evaluating the microcysts parameters, the mean density and mean area values were found to be 26.3 (10.6) cysts/mm2 and 5797.0 (4021.0) μm2, respectively, which were not significantly different from those reported in patients before trabeculectomy.
At 6 weeks, the mean IOP was 15.9 (1.7) mm Hg, and the epithelial and microcysts features were substantially unmodified with respect to baseline (fig 4). Also, the microcyst parameters did not show statistically significant modifications: mean microcyst density and mean microcyst area values of 26.5 (11.8) cysts/mm2 and 6096.9 (3389.1) μm2, respectively.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Planar reconstruction of the superior bulbar conjunctiva in a glaucomatous eye under medical therapy, after 6 weeks. No significant differences with respect to baseline examination were found, either in the features or in the pattern of distribution of epithelial microcysts.
In both groups of patients, we did not observe any signs of inflammatory dendritic or round cell infiltration within the epithelium.
Discussion
The main challenge of filtering surgery is to induce a decrease in preoperative IOP by increasing aqueous outflow via a new pathway, thereby reducing the progression of glaucoma. Among diagnostic methods available in the clinical practice, the slit-lamp evaluation of the site of trabeculectomy yields important information concerning the conjunctival bleb characteristics such as extension, elevation and vascularisation. Currently, this method is considered a reliable procedure to clinically assess tissue modifications induced by trabeculectomy. Recently, the use of IVCM provided additional information in filtering bleb examination because it permitted a microscopic analysis of specific conjunctival features such as the presence of epithelial microcysts and the density of subepithelial connective tissue.8 9 10 11 However, to date, these characteristics have been considered as only a sign of tissue rearrangement or modification, exclusively induced by the surgical procedure.
The results of this study showed that conjunctival modifications were pre-existent to trabeculectomy: epithelial microcysts appeared widely present and diffuse also in glaucomatous eyes under medical therapy before surgery. Therefore, surgery influenced a pre-existing phenomenon in that either the eyes scheduled for trabeculectomy or control eyes under medical therapy showed similar features with regards to characteristics and distribution of microcysts, even though the IOP was quite different between the two groups and significantly higher in eyes undergoing surgical therapy. These observations are in agreement with those reported in our previous study in which we demonstrated the absence of epithelial microcysts in healthy eyes and conversely documented their presence in all eyes with increased IOP, affected with either untreated ocular hypertension or treated open-angle glaucoma.12 Furthermore, as confirmed by the repeated analysis of conjunctival epithelium in the control group after 6 weeks, the presence and features of microcysts in glaucomatous eyes did not show any significant modifications, at least not after the short period of time evaluated in this study.
The final effect of the filtering procedure was a fivefold increase in conjunctival microcyst density and surface area on the site of the bleb with respect to preoperative values: a sign of a marked aqueous filtration enhancement through the sclera and, subsequently, the conjunctiva. One possible theory to explain these results is that an activation of trans-scleral outflow might be induced in medically treated glaucomatous eyes by the hyperbaric condition as an alternative pathway of humour aqueous drainage. But the presence of epithelial microcysts should not be considered a side effect of antiglaucoma drugs or preservatives, since these structures were also found in cases of untreated ocular hypertension.12
However, this adaptation mechanism by itself was not sufficient to re-establish a controlled IOP because, as previously reported,17 18 the potential in vitro human trans-scleral outflow capacity was 0.33 μl×min×mm Hg in the suprachoroidal space, a much higher value than in vivo (1.1–1.5 μl/min). Based on these findings, filtering surgery is successful when the trans-scleral outflow capability is substantially increased. The active role of the transcleral and trans-conjunctival aqueous percolation for the maintenance of bleb functionality in trabeculectomised eyes has been previously supposed15 19 20 and confirmed by several observations which suggested that a successful trabeculectomy yielding a strong decrease in postoperative IOP required the presence of low-density subconjunctival connectival tissue and a high density and wide surface area of intraepithelial microcysts.8 9 10 11
However, two aspects of our study require further elucidation: the role of topical therapy in the pathogenesis of preoperative conjunctival modifications and the effect of both intraoperative MMC and postoperative medications on postsurgical findings. To date, as previously mentioned, clear evidence that topical antiglaucoma drugs or preservatives are involved in the microcysts formation and persistence has not been reported.12 In order to define the real influence of antiglaucoma drugs on reported conjuncival features, a prospective study evaluating the conjunctiva of native glaucomatous eyes before and after medical therapy is mandatory. We propose that MMC and steroids could have only a limited role in the development of the conjunctival modifications seen in our study, probably leading, with greater frequency, to higher microcyst diameters, to thinning of the microcysts wall, and to clustering and reduction in postoperative scarring. In accordance with our hypothesis, Labbé et al8 reported that epithelial microcysts were smaller in diameter in trabeculectomy without MMC (from 10 to 150 μm) with respect to filtering surgery with MMC application (from 10 to 300 μm).
Furthermore, in the same study, the authors did find the presence of hyper-reflective microdots in the superficial epithelium layer (probably representing necrotic epithelial cells or inflammatory cells) only in eyes that received MMC and in no eyes that did not.
Conversely, in an our previous study11 in which we analysed different epithelial parameters such as the microcyst density and surface of filtering blebs with and without the intraoperative use of MMC, we did not report any microscopic differences between patients who received intraoperative MMC and patients who did not. When analysing subepithelial layers, Messmer et al9 reported a bleb stroma organised with a less rarified collagen-like network and with smaller cystic spaces in patients who did not receive intraoperative MMC with respect to patients who did.
By considering all these findings, one may suggest that the use of intraoperative MMC affects the feature of the bleb stroma and the size of epithelial microcysts, but probably do not modify the total surface of intraepithelial microscysts.
Recently Amar and colleagues,21 using both impression cytology and in vivo confocal microscopy, hypothesised that microcysts observed at the surface of functioning blebs seemed to correspond to goblet cells, mostly containing aqueous humour instead of highly hydrophilic gel-forming mucins. Therefore, they suggested that the transcellular pathway of the aqueous humour could occur at the level of goblet cells toward the ocular surface. The authors proposed that larger microcysts observed using in vivo confocal microscopy could correspond to a confluence of adjacent empty or degenerating goblet cells, resulting in large clear spaces. In our study, the presence of conjunctival globet cells was not methodically investigated because we searched for anatomical modifications of so-called conjunctival epithelial cysts induced by surgery and not for biological analysis of cell morphology or function. However, the hypothesis of biological modification of globet cells is an interesting feature that deserves further investigation.
In conclusion, the analysis of conjunctiva in medically and surgically treated glaucomatous patients before and after trabeculectomy provided additional and valuable information which clarified important physiopathological aspects of the aqueous outflow and the effects induced by filtering procedures.
REFERENCES
Footnotes
Competing interests None.
Provenance and Peer review Not commissioned; externally peer reviewed.
Patient consent Obtained.
Linked Articles
- At a glance