


Abstract
Background/Aim: Osteosarcoma is a rare type of bone cancer that affects mostly children and adolescents. First-line chemotherapy for osteosarcoma has not been improved for many decades. Eribulin has been used to treat breast cancer and liposarcoma in the clinic. Materials and Methods: A patient-derived orthotopic xenograft (PDOX) mouse model of osteosarcoma was established by tumor insertion within the tibia. This model more closely mimics osteosarcoma in clinical settings and was used to test the efficacy of eribulin. Tibia-insertion osteosarcoma PDOX mouse models were randomized into two groups: a control group (n=4) and an eribulin-treatment group (n=5). Mice were treated for fourteen days, four weeks after initial implantation. Tumor size and body weight were measured, and tumor histology was examined. Results: Significant tumor growth inhibition (p=0.044) was observed in mice treated with eribulin compared to the control group. Histology demonstrated necrosis in the eribulin-treated tumors. There was no body-weight loss in the treated mice. Conclusion: Eribulin may be a clinically-effective, off-label chemotherapy for recalcitrant osteosarcoma that has failed first- and second-line therapy.
Osteosarcoma is a rare bone cancer affecting mostly children and adolescents; there are only 1,000 new cases per year in the United States (1). Surgery, radiation, and a combination of neoadjuvant and adjuvant chemotherapy are first-line treatment for osteosarcoma (2, 3). The current first-line chemotherapy for osteosarcoma is a combination of high-dose methotrexate, doxorubicin, and cisplatinum (4). Osteosarcoma patients often develop resistance to these drugs, which leads to metastases and fatality (5). Novel, more-effective treatment for osteosarcoma has been difficult to develop. Many previous animal studies testing new therapies for osteosarcoma used subcutaneous-implantation mouse models, which are poor surrogate models of cancer in patients and may not reflect the effectiveness of treatments as accurately as orthotopic-implantation models (6-9).
Our laboratory developed the patient-derived orthotopic xenograft (PDOX) model for many cancer types, including osteosarcoma (5, 10). Recently, we developed an improved osteosarcoma PDOX model in which the tumor is inserted into a hole made in the tibia of nude mice in order for the patient osteosarcoma to grow within the bone, as it does clinically (11). Eribulin is a third-line FDA-approved therapy for metastatic breast-cancer patients who were previously treated with an anthracycline and a taxane (12). Eribulin has also been approved for the treatment of metastatic liposarcoma patients who have progressed after anthracycline treatment (12). A Phase II study of eribulin conducted in recurrent or refractory osteosarcoma patients showed no objective responses (4). The present study uses an orthotopic, more-clinically-accurate osteosarcoma mouse model to test eribulin as a potential effective off-label chemotherapy for treating patients with osteosarcoma, who have failed first-line chemotherapy (11).
Materials and Methods
Mice. The present study was conducted on athymic (nu/nu) nude mice (AntiCancer, Inc., San Diego, CA, USA) and followed an AntiCancer, Inc. Institutional Animal Care and Use Committee (IACUC) protocol specifically approved for this study. The present study followed the principles and procedures outlined in the National Institutes of Health Guide for the Care and Use of Animals under Assurance Number A3873-1. All animal procedures have been previously described (13-20).
Patient-derived tumor. The osteosarcoma was obtained previously from a 14-year-old boy with pelvic osteosarcoma following a UCLA Institutional Review Board-approved protocol (IRB#10-001857) with written informed consent obtained from the patient and his parents. The patient was not administered chemotherapy or radiotherapy before the fresh biopsy sample was taken (20).
Establishment of an orthotopic osteosarcoma tibia-implantation PDOX model. Nude mice with subcutaneously-implanted tumors larger than 10 mm in diameter were anesthetized with a ketamine mixture and tumor tissue was harvested and divided into 1 mm3 fragments (11). In nude mice, after a skin incision was made and the tibia was exposed, a blade was inserted into the tibia bone and rotated to create a hole 1-mm in diameter (Figure 1A) (11). The tumor fragment was placed inside the hole (Figure 1B). The wound was closed with a 5-0 PDS-II suture.
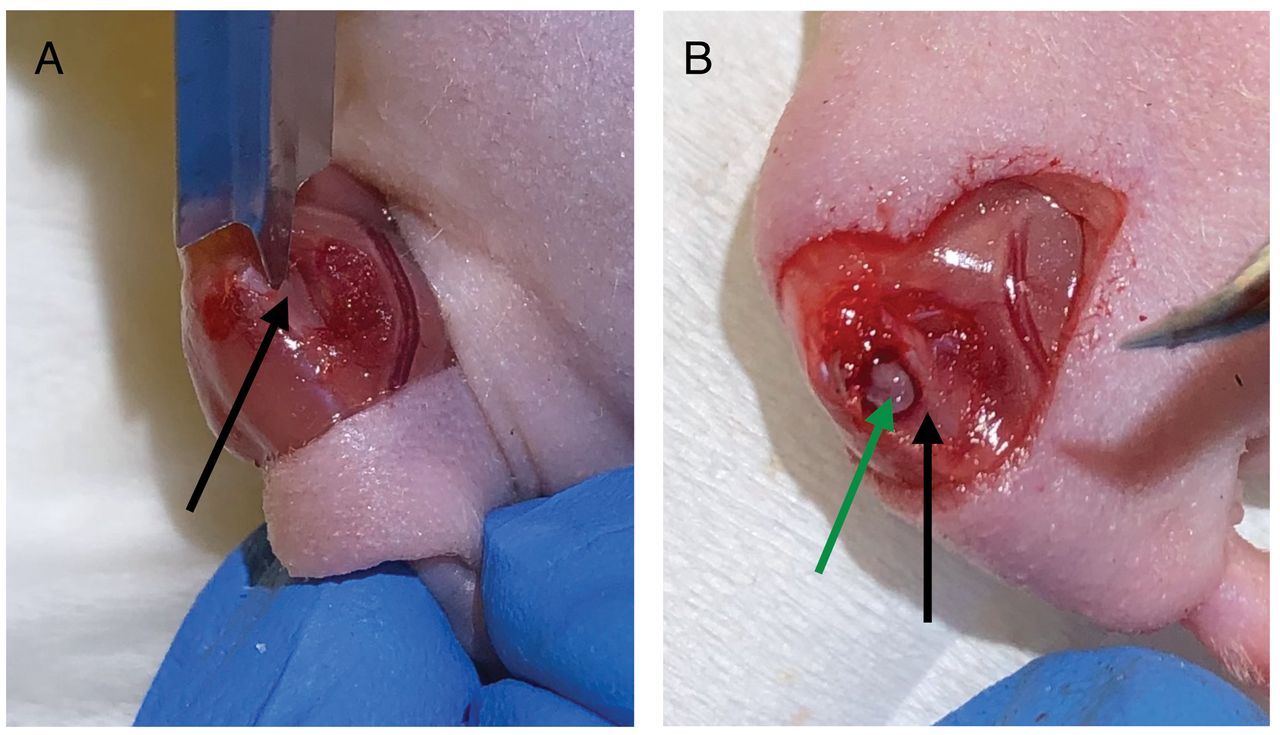
Establishment of a tibia-insertion osteosarcoma PDOX model. The black arrows indicate the tibia bone. (A) Hole made in the tibia by rotating a blade. (B) A one-mm3 tumor fragment was implanted into the hole in the tibia, using a fine tweezer. The green arrow indicates the tumor fragment inserted in the hole created in the tibia.
Treatment scheme. The osteosarcoma PDOX models were divided into two groups randomly, four mice in the control group and five mice in the treatment group. After four weeks, tumor size was measured. The following treatment scheme was performed for two weeks: control group, no treatment; treatment group, eribulin 0.25 mg/kg by intraperitoneal injection, once a week (Figure 2). Mice were weighed and tumor size was measured with calipers at one and two weeks after the start of treatment. Tumor volume was calculated as previously described (7). All mice were sacrificed 6 weeks after implantation, as previously described (13-21).

Schematic of treatment plan. Tumor and body weight measurement: Days 0, 7, 14. Eribulin administered: Days 0 & 7.
Hematoxylin and eosin staining. Fixation, paraffin sectioning, and staining were performed, as previously described (14). Hematoxylin and eosin (H&E) staining was performed according to standard protocols (19).
Statistical analysis. All statistical analyses were performed with JMP Pro ver.15.0.0 (SAS Institute, Cary, NC, USA). The Student’s t-test was used to compare two groups. p-values were two-sided, and a p-value of ≤0.05 is regarded as statistically significant.
Results
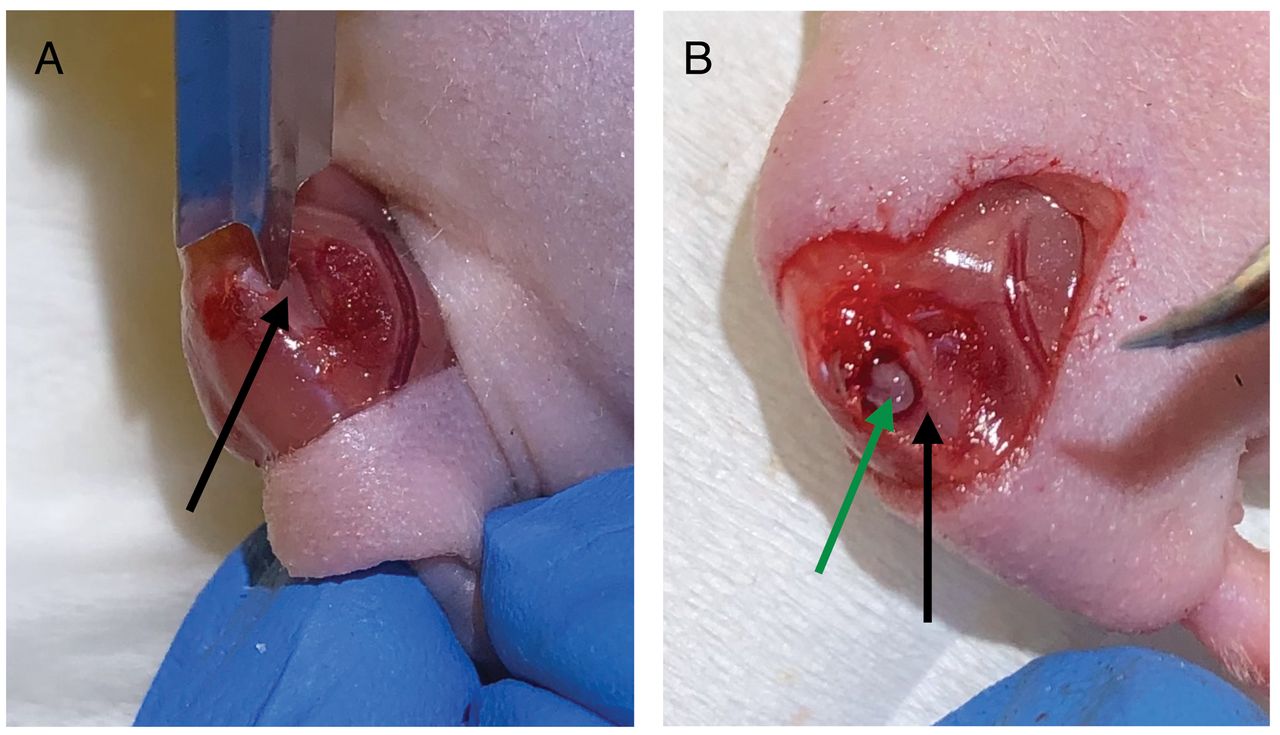
Efficacy of eribulin on the clinically-relevant osteosarcoma PDOX model. The treatment schema is illustrated in Figure 2. Eribulin inhibited tumor growth of the osteosarcoma PDOX model: At day 14, the mean relative tumor volume (tumor volume value at day 14 divided by tumor volume at day 0) in the control mice was 8.9 mm3 and in the eribulin-treated mice, relative tumor volume was 5.4 mm3 (p=0.044) (Figure 3). Representative photos of the tumor-bearing mice clearly show eribulin inhibited osteosarcoma growth (Figure 4). There was no significant difference between the relative body weight (calculated by dividing the body weight of mice at day 14 by the body weight at day 0) of mice in the control group compared to that in the treatment group (Figure 5).

Relative tumor volume (tumor volume at day 7 or 14, divided by tumor volume at day 0). N=4 mice for control group; N=5 mice for treatment group. p<0.05. Bar: mean±SEM.

Osteosarcoma orthotopic tibia-insertion PDOX mouse models. Black arrows indicate location of tumors. (A) mouse from untreated control group, day 14. (B) mouse from treatment group, day 14.
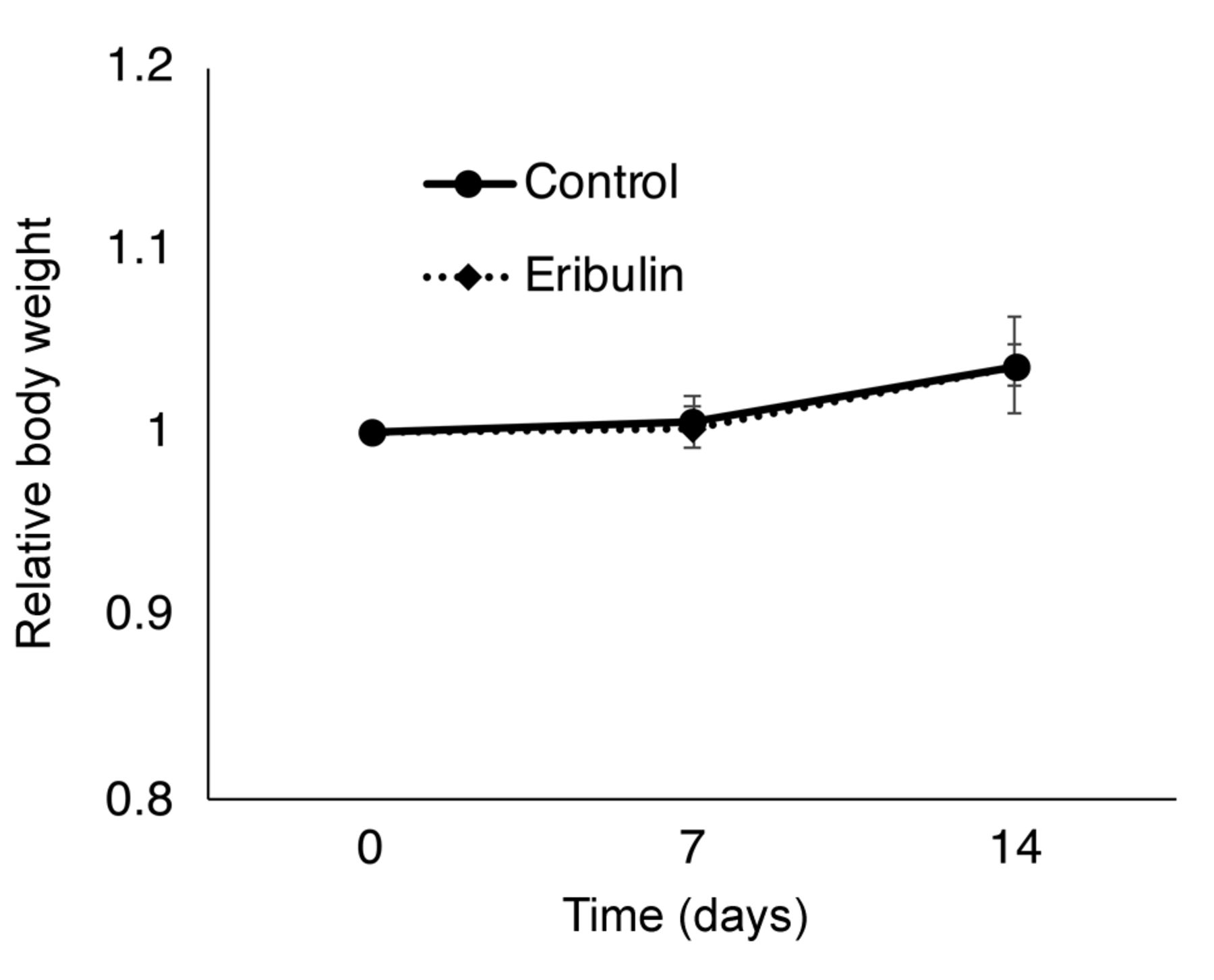
Relative body weight. N=4 mice for control group; N=5 mice for treatment group. p>0.05. Bar: mean±SEM.
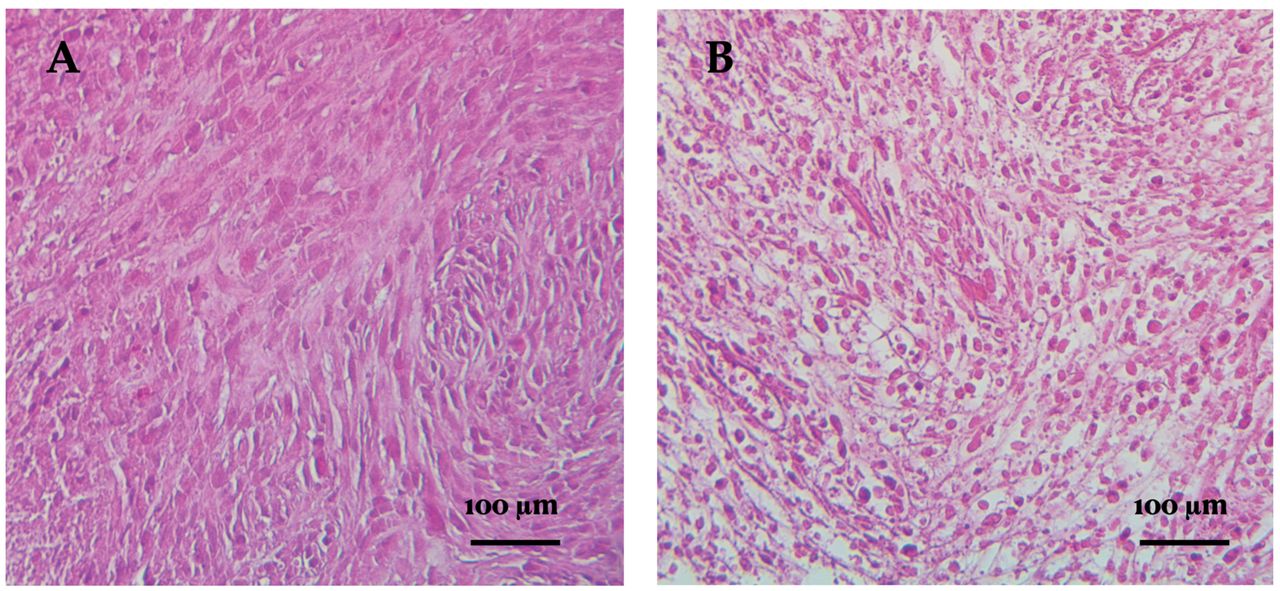
Histology of the treated and control osteosarcoma PDOX model. H&E staining showed that tumors from the control group comprised viable, highly-dense cancer cells with pleomorphic spindle-shaped cells (Figure 6A). H&E staining showed that tumors from the treatment group exhibited decreased pleomorphic spindle-shaped cell density, characteristic of necrosis (Figure 6B).

Tumor histology in the osteosarcoma PDOX model. Scale bars: 100 μm. (A) Tumor sample from the untreated control group. (B) Tumor sample from the treatment group. 100× Magnification, H&E staining.
Discussion
Until recently, most mouse models of osteosarcoma have utilized subcutaneous transplants of tumors, which ignores the fact that osteosarcoma grows in the bones of patients. Our laboratory developed the first-generation orthotopic model of patient osteosarcoma by implanting the tumor into the internal condyle of the femur (21). Although the first-generation PDOX model was a qualitative improvement over the subcutaneous models, the osteosarcoma was growing on the bone rather than in the bone, as it does in patients (21). Recently, we developed a second-generation osteosarcoma PDOX model with a 1 mm hole made in the mouse tibia, in which the patient osteosarcoma tissue was implanted (11). Thus, in the second-generation osteosarcoma PDOX model the tumor grows within the bone. A bone-insertion model of a bone tumor is far more clinically relevant than subcutaneous models where the tumor is in a heterotopic microenvironment (22).
A recent review has emphasized the importance of patient-derived cancer models for rare cancers but claims the paucity of patient-derived mouse models, especially of sarcomas (23). The review fails to cite any of the more than sixty papers on PDOX models of all major types of sarcoma (5, 13-21, 24).
In a previous study, using the first-generation osteosarcoma PDOX model established from a lung-metastatic osteosarcoma, eribulin was also found to be effective (21). The present study of an osteosarcoma derived from the pelvis, with a more clinically-relevant model, as well as the previous study of an osteosarcoma derived from a lung metastasis, indicate the clinical potential of eribulin for refractory osteosarcoma that has failed first-line or higher lines of chemotherapy. If a patient’s osteosarcoma PDOX model shows sensitivity to eribulin, the present and previous results suggest its off-label use for the patient may be considered.
Acknowledgements
This paper is dedicated to the memory of A. R. Moossa, M.D., Sun Lee, M.D., Professor Li Jiaxi and Masaki Kitajima, M.D.
Footnotes
Authors’ Contributions
N.W., J.Y., and R.M.H designed and performed experiments and wrote the article; J.Y. and Y.A. gave technical support and conceptual advice. N.W., M.B., and R.M.H wrote, reviewed, and/or revised the manuscript.
This article is freely accessible online.
Conflicts of Interest
AntiCancer uses PDOX models for contract research. N.W., J.Y., Y.A., and RMH are or were unsalaried associates of AntiCancer Inc. The Authors declare that there are no potential conflicts of interest regarding this study.
Funding
The present study was funded in part by Robert M. Hoffman Foundation for Cancer Research, which had no role in the design, execution, interpretation, or writing of the study.
- Received March 3, 2021.
- Revision received March 12, 2021.
- Accepted March 16, 2021.
This is an open access article distributed under the CC BY license (https://creativecommons.org/licenses/by/4.0/).
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Non-invasively Imageable Tibia-tumor-fragment Implantation Experimental-bone-metastasis Mouse Model of GFP-expressing Prostate Cancer
- Oral-recombinant Methioninase Converts an Osteosarcoma from Methotrexate-resistant to -sensitive in a Patient-derived Orthotopic-xenograft (PDOX) Mouse Model
- Osteosarcoma Patient-derived Orthotopic Xenograft (PDOX) Models Used to Identify Novel and Effective Therapeutics: A Review
- Osteosarcoma of the Breast in a Patient Derived Orthotopic Xenograft (PDOX) Mouse Model Is Arrested by both Cisplatinum and Eribulin