


Abstract
Background/Aim: In the present study, the breast cancer patient-derived orthotopic xenograft (PDOX) model was used to identify an effective drug for a highly aggressive triple negative breast cancer (TNBC). Materials and Methods: The TNBC tumor from a patient was implanted in the right 4th inguinal mammary fat pad of nude mice to establish a PDOX model. Three weeks later, 19 mice were randomized into the untreated-control group (n=10) and the eribulin treatment group (n=9, eribulin, 0.3 mg/kg, i.p., day 1). Results: On day 8, eribulin significantly inhibited tumor volume compared to the control group (p<0.01). Eribulin regressed tumors in 3 mice (33.3%) and apparently eradicated them in 6 mice (66.7%). At day 14, tumor regrowth was observed in 2 mice of the eribulin group, which was undetectable on day 8. However, 44.4% (4 out of 9) of the mice in the eribulin group were tumor-free on day 14. Conclusion: A single low-dose eribulin was efficacious on a highly aggressive TNBC. The breast cancer PDOX model can be used to identify highly effective drugs for TNBC.
- Eribulin
- PDOX
- patient-derived orthotopic xenograft
- patient-derived xenograft
- PDX
- TNBC
- triple-negative breast cancer
Between 10~20% of breast cancer patients are diagnosed with triple negative breast cancer (TNBC) based on the lack of estrogen receptor (ER), progesterone receptor (PR) and human epidermal growth factor receptor 2 (HER-2) (1). Triple negative breast cancer is treated with chemotherapy and/or radiotherapy after surgery, but has a poor prognosis despite chemotherapy, such as anthracyclines and taxanes, and is considered a recalcitrant disease with poor survival (2, 3).
Eribulin is a non-taxane, synthetic microtubule-dynamics inhibitor with antimitotic activity. Eribulin binds microtubule ends to prevent microtubule polymerization, blocks the cell cycle at the G2/M cell-cycle phase, and causes apoptosis (4). Eribulin also affects tumor vasculature remodeling, which increases vascular perfusion, reduces hypoxia, reverses epithelial-to-mesenchymal transition (EMT) and decreases migration ability and invasion (5-7). Recently, Eribulin has been used for patients with metastatic breast cancer since it showed increased overall survival in the EMBRACE trial (8).
Patient-derived orthotopic xenograft (PDOX) models of immunodeficient mice can recapitulate the histopathologic/molecular characteristics of the primary tumor (9, 10) and can be used to screen multiple chemotherapeutics for individual treatment. Our laboratory developed the patient-derived orthotopic xenograft (PDOX) model of breast cancer in nude mice and described the orthotopic growth and metastases to the lung of breast cancer in 1993 (11).
In the present study, we established a PDOX nude-mouse model of a highly aggressive TNBC and evaluated the efficacy of eribulin using this model.
Materials and Methods
Mice. Athymic nu/nu nude female mice (AntiCancer Inc., San Diego, CA, USA), 4-6 weeks old, were used in this study. Animals were housed in a barrier facility on a high efficiency particulate arrestance (HEPA)-filtered rack under standard conditions of 12-hour light/dark cycles. The animals were fed an autoclaved laboratory rodent diet. All animal studies were conducted according to an AntiCancer Institutional Animal Care and Use Committee (IACUC)-protocol specifically approved for this study and in accordance with the principles and procedures outlined in the National Institute of Health Guide for the Care and Use of Animals under Assurance Number A3873-1. To minimize any suffering of the animals, anesthesia and analgesics were used for all surgical experiments. Animals were anesthetized by subcutaneous injection of a 0.02 ml solution of 20 mg/kg ketamine, 15.2 mg/kg xylazine, and 0.48 mg/kg acepromazine maleate. The response of animals during surgery was monitored to ensure adequate depth of anesthesia (9, 10).
Patient-derived TNBC and establishment of PDOX. A 74-year-old female patient was diagnosed with invasive ductal carcinoma in the right breast. She underwent breast-conserving surgery with sentinel lymph node biopsy in the Department of Surgery, Samsung Medical Center (SMC), Seoul, Korea. The tumor size was 2.4 cm and nodal status was N0. Histologic grade was 3. ER/PR/HER2 was negative and the Ki-67 value was 80.35%. Written informed consent was obtained from the patient, and the Institutional Review Board (IRB) of SMC approved this experiment. Fresh patient-derived tumor tissue samples were immediately transported to the laboratory at MetaBio Inc. on ice. The samples were cut into 3~4 mm3 size fragments and implanted subcutaneously into nude mice. After subcutaneously-grown tumors reached 10 mm in diameter, they were harvested and cut into 2~3 mm3 size fragments. The tumor fragments were implanted in the right 4th inguinal mammary fat pad by surgical orthotopic implantation (SOI) to establish the PDOX model. The wound was closed with 7-0 nylon suture (11).
Treatment dose and schedule. Three weeks after SOI, the TNBC PDOX mouse models were randomized into two groups of nine to ten mice each: G1, untreated control (n=10); G2, eribulin (n=9, 0.3 mg/kg, i.p., day 1). And then mice were observed for two weeks.
Tumor length, width, and mouse body weight were measured twice a week. Tumor volume was calculated with the following formula: Tumor volume (mm3)=length (mm)×width (mm)×width (mm)×1/2. Mice in the control group were sacrificed on day 8 and in the eribulin group on day 14.
Statistical analyses. All statistical analyses were performed with R ver. 3.6.1 (R foundation, Vienna, Austria). Significant differences were determined using the Student's t-test. Graphs show the mean tumor volume and number of mice, and error bars represent standard deviation. A probability value of p<0.05 was defined as statistically significant.
Results
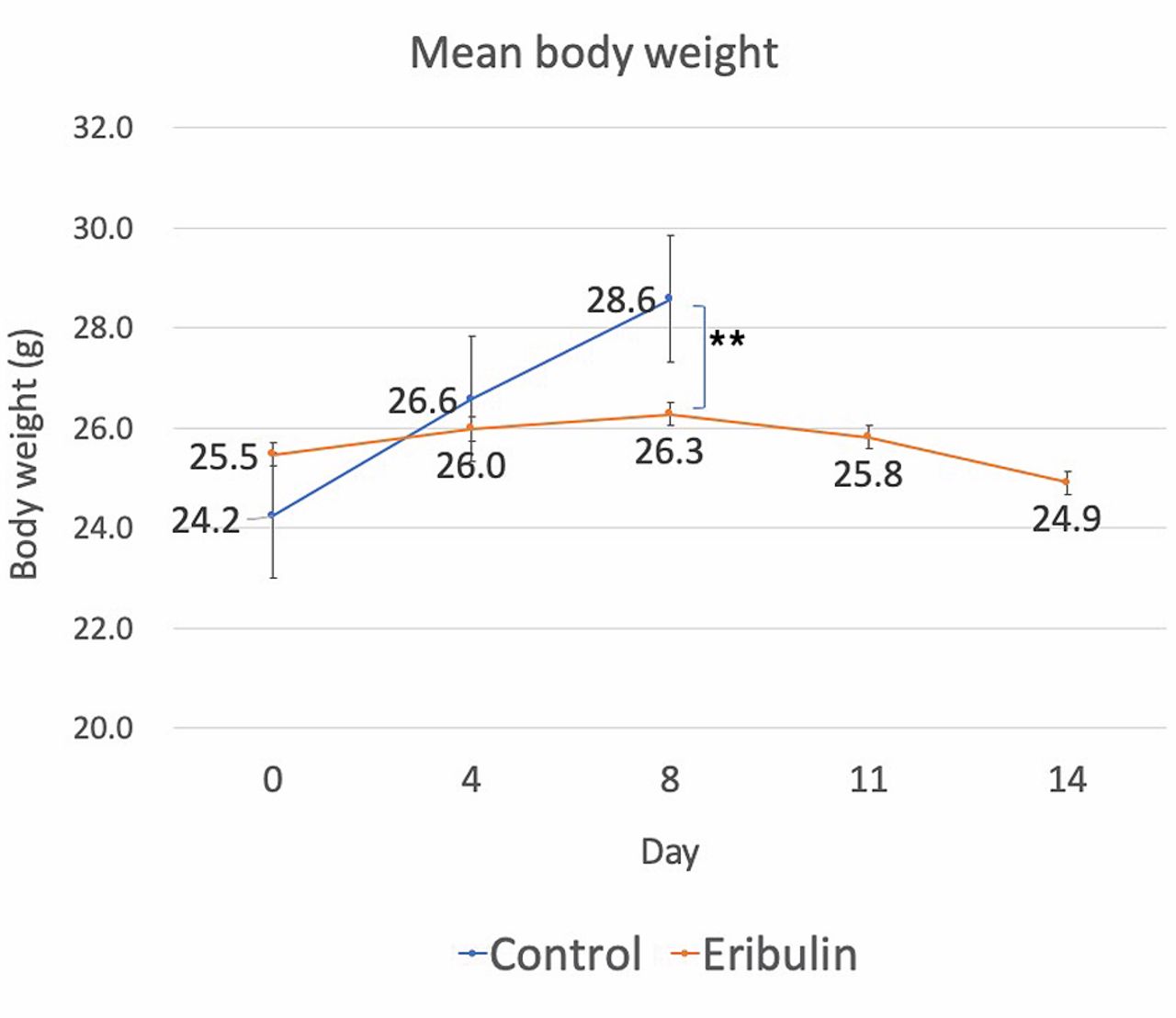
On day 8, 6 out of 10 mice in the control group had tumors larger than 3000 mm3 with a mean tumor volume of 3156.33 mm3. In contrast to the control group, the mean tumor volume of the eribulin group was 19.1 mm3 (p<0.01, Figure 1). All tumors either regressed or disappeared in the eribulin group on day 8 (Figure 2). Tumors regressed in 3 mice (33.3%) and disappeared in the other 6 mice (66.7%). On day 14, 44.4% of the mice (4 out of 9) in the eribulin group still were without tumors. There was no statistically significant difference in body weight between the two groups on day 0 and day 4. But on day 8, there was a statistically significant difference on body weight that may be the result of differences in the tumor burden between the two groups (Figure 3). Histology did not show a difference between the tumors of the control group and the regrown tumors of the eribulin group (Figure 4).
Discussion
Eribulin has been previously shown to be efficacious at doses ranging from 0.1-2 mg/kg, once to thrice a week in several in vivo studies with tumors derived from cancer cell lines (4, 12, 13).
The present study has important implications since it demonstrated the efficacy of eribulin on a highly aggressive TNBC in a PDOX model by showing tumor regression and disappearance with a single low-dose eribulin.
Eribulin showed an improvement in overall survival (OS) compared with available cytotoxic therapy in patients with heavily pretreated metastatic breast cancer in the EMBRACE trial (8).
Another Phase III trial compared eribulin with capecitabine in metastatic breast cancer. There was a significant survival advantage with eribulin over capecitabine among breast cancer patients with HER2-negative breast cancer as well as TNBC (14). Based on these results, eribulin is used for the treatment of patients with metastatic breast cancer.
In TNBC, pathologic complete response (pCR) at the time of surgery is a favorable prognostic factor correlated with improved disease outcomes. The efficacy of eribulin as neoadjuvant treatment was studied only to a limited extent and some results were disappointing. Other clinical trials have not shown significantly improved efficacy of neoadjuvant eribulin over standard therapies (15, 16). But eribulin is still an attractive drug because its toxicity profile compares favorably with taxanes, and also avoids the risk of late toxicities associated with anthracyclines (17).
In the present study, the patient's tumor was growing rapidly compared with previously reported tumors from breast cancer cell line (18). It only took four weeks to reach a 3000 mm3 tumor volume in the control mice and we could get important information about the aggressiveness of this tumor by establishing and using a PDOX model of the patient's tumor. The breast cancer PDOX model was developed by our laboratory in 1993 (11) and it took another 18 years until another laboratory published on a breast cancer PDOX model, claiming novelty for their study (18).

Tumor volume. TNBC tumors were implanted by surgical orthotopic implantation (SOI) in the right 4th inguinal mammary fat pad. Chemotherapy started. Resulting tumors were measured with calipers (*p<0.01).

Tumor regression in the eribulin group. Presence of tumor was determined by tumor volume measurement and palpation.

Mean body weight. Body weight was measured twice a week (**p<0.05).
In conclusion, eribulin regressed a highly aggressive TNBC in the PDOX model. In this study, the PDOX model was successfully used to demonstrate that a single low-dose eribulin was effective against TNBC and this result suggested the potential of eribulin as a treatment for TNBC. Orthotopic models of cancer represent clinical cancer, unlike subcutaneous tumor models (19-21). Future experiments will label the TNBC PDOX with fluorescent proteins in order to visualize micro-metastasis (22).

Histology of PDOX TNBC. Hematoxylin and eosin (H&E) staining of the untreated control PDOX tumor (A) and the eribulin-treated PDOX tumor (B).
Acknowledgements
This paper is dedicated to the memory of A. R. Moossa, M.D., Sun Lee, M.D., Professor Li Jiaxi, and Masaki Kitajima, MD.
Footnotes
Authors' Contributions
Conception and design: HIL and RMH. Acquisition of data: HIL, JY, SI, HN, YT, NS, QH, YS, and RMH. Analysis and interpretation of data: HIL, JY, SI, HN, YT, NS, QH, YS, HJC, SJN, MBK, JSL, CH, MB, SRS, and RMH. Writing, review, and/or revision of the manuscript: HIL, RMH, and SRS.
This article is freely accessible online.
Conflicts of Interest
AntiCancer Inc. uses PDOX models for contract research. HIL, JY, SI, HN, YT, NS, QH, YS and RMH are or were unsalaried associates of AntiCancer Inc. There are no other competing financial interests.
- Received March 24, 2020.
- Revision received April 5, 2020.
- Accepted April 6, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Non-invasive Fluorescence Imaging of Breast Cancer Metastasis to the Brain in an Orthotopic Nude-mouse Model With Very-narrow-band-width Laser Excitation of Red Fluorescent Protein Resulting in an Ultra-bright Signal Without Skin Autofluorescence
- Salmonella typhimurium A1-R Exquisitely Targets and Arrests a Matrix-producing Triple-negative Breast Carcinoma in a PDOX Model
- Efficacy of Oral Recombinant Methioninase and Eribulin on a PDOX Model of Triple-negative Breast Cancer (TNBC) Liver Metastasis
- A triple-negative matrix-producing breast carcinoma is arrested by tumor-targeting Salmonella typhimurium A1-R in a PDOX model
- Oral Methioninase Inhibits Recurrence in a PDOX Mouse Model of Aggressive Triple-negative Breast Cancer