


Abstract
Background/Aim: The plasma level of the oxidative stress biomarker catalase in patients with gallstone disease has not been previously compared with that of patients with cancer. Moreover, the number of analgesic doses required during the first 24 h postoperatively (NAD24) after laparoscopic cholecystectomy (LC) or mini-cholecystectomy (MC) in patients with gallstones is unreported. The aim of the present study was to determine the correlation between the plasma catalase level in patients with gallstones according to cholecystectomy technique versus patients with cancer. Patients and Methods: Initially, 114 patients with symptomatic gallstone disease were randomized into LC (n=54) or MC (n=60) groups. The plasma level of catalase was measured immediately before, immediately after and 6 hours after operation. Results: The median plasma catalase levels preoperatively and following surgery in the LC and MC patients versus those with cancer did not differ statistically significantly. The median plasma level of catalase increased immediately after operation, but the alteration was statistically insignificant (p=0.132). Interestingly, there was a statistically significant weak inverse correlation between the individual NAD24 and median plasma catalase values postoperatively in patients with gallstone disease (r=−0.283, p=0.042). Conclusion: The plasma catalase levels preoperatively and following surgery in the LC and MC patients versus those with cancer were quite similar. Cholecystectomy patients with high plasma levels of catalase appeared to require significantly fewer analgesic doses during the first 24 hours postoperatively (NAD24), suggesting that better oxidative balance following surgery could have a protective role against postoperative pain.
Gallstone disease (GSD) is one of the most common gastrointestinal disorders, affecting 6-22% of adults in Western countries (1). Cholecystectomy is one of the most common abdominal surgical procedures performed in the USA, with over 750,000 operations annually (2). In Finland, 8,478 cholecystectomies were performed in 2015, and laparoscopic cholecystectomy and small-incision mini-cholecystectomy (MC) have been shown to be alternative methods in handling cholecystolithiasis in comparison with open cholecystectomy (3). The safety and effectiveness of MC have been confirmed in several studies (3-14). However, the traditional laparoscopic cholecystectomy (LC) with diathermy hook dissection has been the gold standard in gallstone surgery since the beginning of the laparoscopic era. In comparison to open surgery, LC has several well-known benefits, for example, shorter hospital stay, reduced postoperative pain, improved cosmetic results and shorter convalescence. Despite the advantages of LC, there was up to a five-fold increase in bile leakage and bile duct injury reported at the onset of the era of laparoscopy (15-17). Although recent trends suggest its reduction, the rates for bile duct injury after LC seems to be higher than during the era of open surgery. Interestingly, in spite of MC increasing surgical stress by enhancing the inflammatory reaction (18), there seems to be no major intraoperative and short-term differences comparing LC and MC in the treatment of GSD.
Our previous article reported a statistically significant inverse correlation between the plasma superoxide dismutase-1 (SOD1) levels postoperatively and the individual values of the 11-point numeric rating scale at 24 hours (NRS24) following surgery in patients with benign disease and those with cancer (19). Firstly, the aim of this study was to determine correlation between plasma catalase levels in patients undergoing cholecystectomy compared with patients with cancer and secondly, to determine association between plasma catalase level and analgesic doses during the first 24 hours postoperatively (NAD24) in the patients undergoing cholecystectomy.
Patients and Methods
The study was approved by the Ethics Committee of Kuopio University Hospital District, Kuopio, Finland (DNRO 27/02/2013) and was registered in the ClinicalTrials.gov database (ClinicalTrials.gov Identifier: NCT01723540; Consort diagram, Figure 1), and was conducted in accordance with the Declaration of Helsinki. The study was a prospective, randomized, multicenter clinical trial consisting of 114 patients with confirmed symptomatic cholelithiasis. Written consent was collected from participants, after receiving verbal and written information about the study. Patients were randomized to undergo either LC (n=54) or MC (n=60) at two separate hospitals in Finland: Kuopio University Hospital, Kuopio (n=86) and Helsinki University Central Hospital, Helsinki (n=28) between March 2013 and May 2015. The design of the study is presented in Figure 1. After patient enrolment, randomization was achieved with a sealed envelope method assigning patents to either LC or MC groups. The patients with cancer, recruited from our previous study, included 10 patients with gastrointestinal cancer and 19 with gynecological cancer (19).
The surgical techniques used were standardized for both groups. The LC procedure was performed using the four-trocar technique (two 10-mm and two 5-mm trocars) and intra-abdominal pressure was set at 12 mmHg. Ultrasonic scissors (Harmonic ACE®; Ethicon Endo-Surgery, Cincinnati, OH, USA) were used in both the MC and LC procedures. The gallbladder was dissected from the liver with ultrasonic scissors. The cystic artery was sealed with ultrasonic scissor and two metal clips were inserted into the cystic duct.
The MC technique is minimalIy invasive open technique with very short wound; the mean length of skin incision (±SD) was 4.8 (±1.6) cm, and the rectus muscle was not cut, but split. A skin incision length of more than 7.0 cm or cutting of the rectus muscle was considered as a conversion to conventional open operation. Incisions were infiltrated with local anesthetic (20 ml ropivacaine at 7.5 mg/ml) at the end of the operation. Both study groups were standardized regarding endotracheal anesthesia and postoperative care including the overall pain surveyed and filed on a 11-point NRS following surgery (0=no pain; 10=worst pain).
For postoperative rescue analgesia, the patients were given 3 mg oxycodone i.v. if the pain at rest was NRS 3/10 or higher or the NRS was 5/10 or higher during cough/movement. The total number of 3-mg oxycodone doses required during the first 24 hours postoperatively (NAD24) for cholecystectomy patients was very carefully recorded in the patient records. The study protocol was fully described in our earlier original work (20).
EDTA-blood samples were taken before surgery (PRE) immediately after surgery (POP1) and at 6 hours post-operatively (POP2) and centrifuged at 1,000 × g for 15 minutes. Plasma was separated and stored frozen at −70°C until analyzed. Plasma high sensitivity C-reactive protein (hs-CRP) levels was analyzed with a Cobas 6000-analyzer (Hitachi, Tokyo, Japan) using the method by Roche Diagnostics (Mannheim, Germany). The plasma catalase assays were performed using enzyme-linked immunosorbent assay ELISA Kit (Elisa kit for catalase, product number SEC418Hu; Cloud-Clone Corporation, Katy, TX, USA). The manufacturers intra-assay CV% and the inter-assay CV% were <10% and <12%, respectively.
The data were entered and analyzed with a statistical software program (IBM SPSS Statistics 24.0; IBM, Armonk, NY, USA). Differences in baseline characteristics between groups were tested by Fisher's exact test and in the case of continuous data, the analysis was performed by independent samples t-test. Group differences at three time points were tested by the Mann-Whitney U-test and the Wilcoxon signed-rank test. The results of the laboratory measurements are presented as median with interquartile range as distributions were right skewed. A two-sided p-value of less than 0.05 was considered statistically significant. Spearman's method was used to test for correlation of individual GPX1 with catalase values immediately after surgery (Figure 2), and for catalase values 6 hours after surgery with NAD24 for cholecystectomy patients (Figure 3).
Results
The perioperative variables and data were quite similar in the study groups. In spite of a slightly higher mean body weight in the LC versus the MC patients (p=0.057, Table I), there was no statistically significant difference in the mean body mass index (p=0.111, respectively, Table I). Interestingly, the mean length of the skin incision was significantly longer in the LC than in the MC group (by >55%, p<0.001, Table I).
The median plasma CAT levels preoperatively and after surgery in the cholecystectomy patients and patients with cancer were quite similar (Table II). However, the patients with cancer had a trend for higher median plasma catalase values after operation compared to the cholecystectomy patients (p=0.052, Table II).
There was a highly significant correlation between catalase and GPX1 values immediately after surgery (r=0.449, p=0.001, Figure 2). Interestingly, there was a statistically significant inverse correlation between the individual NAD24 and median plasma catalase values 6 hours postoperatively in LC and MC patients (r=−0.283, p=0.042, Figure 3). The median plasma level of hs-CRP increased by 7.4% immediately after surgery (p=0.021, Table III) and then had increased by 62.1% at 6 hours postoperatively (p<0.001, Table III).
Discussion
Oxidative stress has an important role in several acute and chronic conditions from reactive oxidative species (ROS)-mediated inflammation and tissue damage in tumorigenesis (21) and oxidative stress following excess use of alcohol (22) to the pathogenesis of toxic liver disease (23) and the possible role of ROS in atherogenesis (24). Since postoperative pain continues to be a significant problem following surgery, we have sought answers to whether there is an association between ROS and pain following surgery. In previous work, we found a statistically significantly inverse correlation between plasma SOD1 values postoperatively and the individual values of the NRS24 following surgery in patients with benign disease and those with cancer (19).

Design of the study as a flowchart. POP1=First sample immediately after surgery, POP2=second sample 6 hours after surgery. CAT=plasma catalase and hs-CRP=high sensitive C-reactive protein.
Catalase is a common enzyme protecting nearly all living cells from oxidative damage by ROS. Catalase is a tetramer of four polypeptide chains, each over 500 amino acids long with four iron-heme groups that allow catalase to react with hydrogen peroxide, decomposing it to water and oxygen (25). The assessment of the plasma catalase levels as a biomarker of oxidative stress in patients with gallstones has been rarely reported. Arsalani-Zadeh et al. (26) and Yiannakopoulou et al. (27) reviewed the literature to compare ROS in open and laparoscopic procedures. There is no meta-analysis available due the heterogeneity of data, selection criteria and diversity of ROS biomarkers used. Eleven studies compared ROS in open and laparoscopic cholecystectomy. There was only one case–control study of catalase available, where Olakowski et al. found enhanced oxidative stress patients who underwent open surgery (n=18) compared to LC patients (n=15) (28).
Baseline demographic characteristics and surgical data for the two study groups. Values are mean±standard deviation or number of cases. Student's t-test or *Fisher's exact test were used.

Scatter plots of plasma catalase (CAT) values immediately post-operatively (POP1) versus glutathione peroxidase (GPX1) values in cholecystectomy patients (r=0.449, p=0.001).
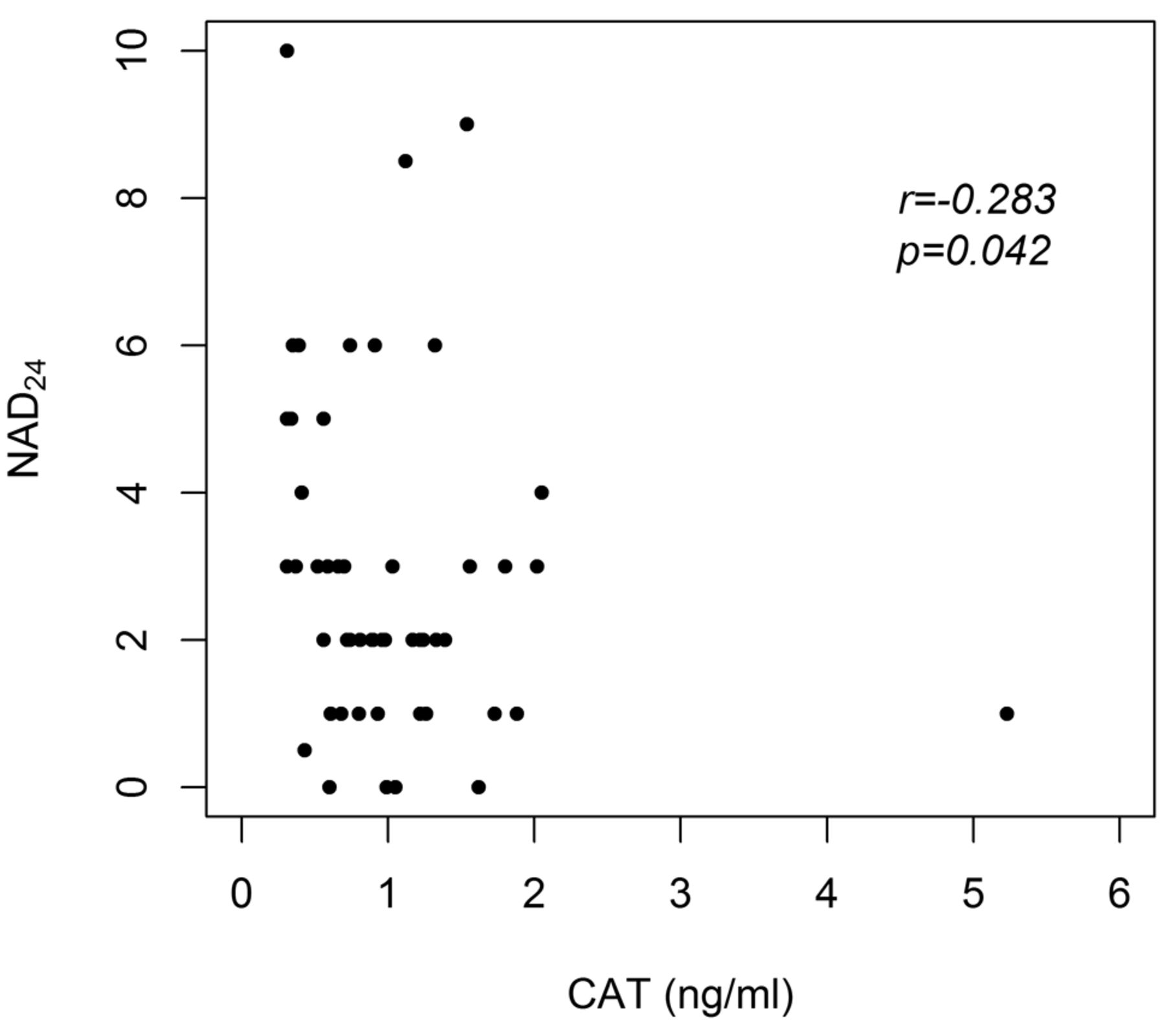
Scatter plots of plasma catalase (CAT) values at 6 hours post-operativeIy (POP2) versus number of analgesic doses during the first 24 hours postoperatively (NAD24) in cholecystectomy patients (r=−0.283, p=0.042).
Plasma levels of high sensitive C-reactive protein (hs-CRP,) and catalase (CAT) before operation (PRE), immediately after operation (POP1) and 6 h after operation (POP2) in patients undergoing minicholecystectomy (MC) and laparoscopic cholecystectomy (LC) compared to patients with cancer. Values are median (interquartile range). Mann-Whitney U-test was used.
The first endpoint of our study was to determine the ROS response to surgical trauma measured by plasma catalase levels in cholecystectomy patients. The second endpoint was to determine the correlation between the plasma catalase levels and NAD24 in LC and MC patients. The quite similar median plasma catalase levels in the LC and MC patients support our earlier finding of similar ROS response to these two techniques (29-31). Interestingly, a highly significant inverse correlation between individual NAD24 values and plasma catalase values postoperatively in cholecystectomy patients was found. This might suggest that enhanced ROS balance following surgery may have a protective role against postoperative pain.
Several methods have been used in the detection of catalase activity (32-34). Türker et al. measured the absorbance of hydrogen peroxide, which is decomposed by catalase, and catalase activity spectrophotometrically (32). The median plasma catalase levels preoperatively and following surgery in the early postoperative and late postoperative (about 24 hours) periods were measured and there was a statistically significant postoperative enhancement in the catalase level in their study (30.4, 43.2, 52.3 IU/g Hb, respectively, p<0.01). Woźniak et al. also determined catalase activity by a quite similar spectrophotometrical method and compared the effect of cervical spinal cord injury (CSCI) on oxidative stress (33): control group I included 30 healthy volunteers, control group II included 15 patients with cerebral contusion without CSCI, and the study group included 42 patients with CSCI. There was a statistically significant difference in the median plasma catalase levels between control groups I and II and the CSCI group (41.5 and 59.4, versus 69.9, respectively, p<0.001). Their results confirm that CSCI damage is accompanied by enhanced oxidative stress.
The postoperative alteration of plasma hs-CRP and catalase (CAT) levels in the group of all patients combined. Plasma levels were measured before operation (PRE), immediately after operation (POP1) and 6 h after operation (POP2). Median (interquartile range) values are shown. The Wilcoxon signed-rank test was used.
Research in biomarkers of ROS has changed dramatically within very few years and the collection of blood samples without altering ROS levels is not a simple procedure (34). Standard operation procedures should be approved and followed strictly throughout blood sample collection, handling and storage (35).
In conclusion, the plasma catalase levels preoperatively and following surgery in cholecystectomy patients and patients with cancer were quite similar. Cholecystectomy patients with high plasma levels of catalase appeared to require significantly fewer analgesic doses during the first 24 hours postoperatively, which may suggest that better oxidative balance following surgery might have a protective role against postoperative pain.
Acknowledgements
The study was funded by the Heikki, Aino and Aarne Korhonen Foundation and the EVO-funding of the Helsinki and Kuopio University Hospital.
Footnotes
Conflicts of Interest
The Authors report no conflicts of interest or financial ties to disclose. The Authors alone are responsible for the content and writing of this article.
- Received July 9, 2018.
- Revision received August 11, 2018.
- Accepted August 21, 2018.
- Copyright© 2018, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Three-dimensional Laparoscopy (3D-LC) Versus Minilaparotomy (MC) in Cholecystectomy: A Prospective Randomized Study
- Plasma Concentration of the Lipid Peroxidation (LP) Biomarker 4-Hydroxynonenal (4-HNE) in Benign and Cancer Patients
- The Induction of Antioxidant Catalase Enzyme With Decrease of Plasma Malonidialdehyde: An Important Reactive Oxidative Species Inhibiting Mechanism
- The Rectus Sheath Block (RSB) Analgesia Following Laparotomy Could Affect Malonidialdehyde (MDA) Concentrations in Benign Disease and Cancer
- Rectus Sheath Block (RSB) Analgesia Could Enhance Significantly the Patient Satisfaction Following Midline Laparotomy in Benign Disease and in Cancer: A Prospective Study With Special Reference to Nitrosative Stress Marker Nitrotyrosine (NT) Plasma Concentrations
- Nitrotyrosine (NT), a Nitrosative Stress Biomarker, Plasma Concentrations in Gallstone Disease and Cancer Patients
- Plasma Catalase in Relation to Pain Following Midline Laparotomy: A Prospective Study of Patients with Benign Diseases and Patients with Cancer