


Abstract
The aim of this study was to explore the efficacy and safety of high-dose pemetrexed with cisplatin versus combination with temozolomide in patients with brain metastases (BM) of lung adenocarcinoma. After standard whole-brain radiotherapy (WBRT, 30 Gy/10 fractions), patients with BM of non-small cell lung cancer (NSCLC) were given high-dose pemetrexed (900 mg/m2) on day 1 of each cycle (3 weeks), and cisplatin was administered on days 1-3 in the cisplatin-treated group. The temozolomide-treated group was treated as follows: 75 mg/m2 temozolomide orally with concurrent WBRT followed by 150 mg/m2 temozolomide on days 1-5 with high-dose pemetrexed (900 mg/m2) on day 1 of each cycle (3 weeks). Six cycles later, high-dose pemetrexed (900 mg/m2) monotherapy or the best available supportive therapy was administered to both groups. An evaluation was carried out every 2-3 cycles. The primary end-points were objective response rate (ORR), progression-free survival (PFS), and overall survival (OS). Secondary end-points included safety and tolerability. Thirty-two patients in the pemetrexed plus cisplatin (PC) group and 28 patients in the pemetrexed plus temozolomide (PT) group were enrolled from November 2013 to October 2015. The ORR was 68.8% and 75%, in the PC and PT groups, respectively, and there was no statistically significant difference between the two groups (p=0.711). The median PFS rates of the PC and PT groups were 13.6 months and 16.9 months, respectively, and the median OS rates of the PC and PT groups were 18.9 months and 19.3 months, respectively. There were no differences in PFS and OS between the two groups. There were no grade 4 or higher side-effects in either group, but grade 3 side-effects such as leucopenia (2/32, 6.3%), nausea/vomiting (2/32, 6.3%), alopecia (1/32, 3.1%), rash (3/32, 9.4%) and renal insufficiency (1/32, 3.1%) were observed in the PC group, whereas the PT-group-only showed the following grade 3 side-effects: leucopenia (1/28, 3.6%) and nausea/vomiting (2/28, 7.1%). The data showed that the PT group achieved the same efficacy in PFS and OS as the PC group but with fewer toxicities. Therefore, high-dose pemetrexed plus temozolomide may be a better regimen for treating NSCLC with BM due to its better safety.
Brain metastases (BM) are a source of significant morbidity and mortality and herald a poor prognosis in patients with metastatic lung cancer. Up to 30% of patients with lung cancer develop metastases during the evolution of their disease (1-3), and 10% of patients have metastases at the time of diagnosis (4). Surgery and stereotactic radiosurgery (SRS) have been extensively used to treat patients with brain metastases (4-7) with one to three brain metastases. Unfortunately, most cases of BM from non-small cell lung cancer (NSCLC) are unable to receive surgery or radiosurgery when they are diagnosed (8). The median survival time of patients with NSCLC with BM treated with whole-brain radiotherapy (WBRT) is 3-6 months, with a significant proportion of patients dying of intracranial progressive disease a few months after treatment (9, 10).
The role of chemotherapy has been evaluated in few studies, with a modest, but clear efficacy that depends on the combination of drugs used (11). Pemetrexed, an inhibitor of thymidylate synthase, dihydrofolate reductase, and glycinamide ribonucleotide formyl transferase, has been shown to be effective against NSCLC with BM (12-14). As a first-line therapy for treating patients with stage IV NSCLC, pemetrexed plus cisplatin showed a 30.6% objective response rate (ORR), 4.8-month median progression free survival (PFS) and 10.3-month median overall survival (OS) (14). Dinglin et al. (13) investigated a 42-patient population and suggested that with concurrent WBRT, the objective cerebral response rate (RR) (complete and partial response) in the intent-to-treat population was 68.3% and that the extracerebral and ORR were 34.1% and 36.6%, respectively. The PFS of patients with BM was 10.6 months, and the median OS was 12.6 months.
Because high-dose chemotherapy is capable of bypassing the blood–brain barrier (BBB) to increase the drug concentration in brain tumours, we adopted high-dose pemetrexed (900 mg/m2), based on the safety and toxicity analyses of phase I studies, to investigate the efficacy and safety of pemetrexed in patients with NSCLC BM (15-17).
Pharmacological therapy for metastatic disease in the central nervous system (CNS) is complicated by the BBB. Temozolomide is a second-generation alkylating agent, with nearly 100% bioavailability, and is administered orally. Temozolomide readily crosses the BBB, achieving cerebrospinal fluid concentrations that are approximately 30% of plasma concentrations in both animal and human models (18). Preclinical and phase I trials have shown the additive and synergistic activity of temozolomide combined with other chemotherapeutic agents against solid tumours (19). Toxicity is lower, with fewer than 5% of patients experiencing myelosuppression (20).
In this prospective cohort study, we compared the efficacy and safety of pemetrexed plus cisplatin (PC) versus pemetrexed plus temozolomide (PT) in patients with BM from NSCLC.
Patients and Methods
Patients. Between November 2013 and October 2015, 60 patients with histologically or cytologically confirmed lung adenocarcinomas with BM were treated with PC (32 patients) or PT (28 patients). Eligible patients were from three institutions, with a Karnofsky Performance status (KPS) of ≥70 and a life expectancy of 8 weeks or longer. In these patients, surgery or radiosurgery of BM was not deemed appropriate.
Baseline evaluations included a complete medical history, physical and neurologic examinations, a determination of the Eastern Co-operative Oncology Group performance status (ECOG PS), a haematological evaluation, and clinical chemistry assessments (including liver and renal function tests). The baseline tumour size was determined by gadolinium-enhanced magnetic resonance imaging (MRI) of the brain. Haematological tests were repeated on day 22 of each cycle. Brain MRI or computed tomographic scans were required every 2 to 3 cycles and 4 weeks after the last course of treatment.
Exclusion criteria included uncontrolled pleural or pericardial effusion or ascites, a severe and uncontrolled complication, uncontrollable diabetes mellitus or hypertension (blood pressure ≥150/100 mmHg), clinically significant cardiovascular disease, pregnancy or lactation, a history of active double cancer, and an unstable psychiatric disorder.
The trial is registered under the number NCT02284490 and was approved by the Ethics Committee of Shandong Cancer Hospital, Qingdao University affiliated Yantai Yuhuangding Hospital, and Shandong University affiliated Qilu Hospital. All enrolled patients, by signing the consent form, stated that they were capable of understanding the diagnosis and nature of treatment.
Treatment. All patients underwent WBRT prescribed at a dose of 30 Gy/10 fractions for 5 days per week up to 2 weeks. At least 2 weeks after the completion of WBRT, pemetrexed (900 mg/m2) plus cisplatin (20 mg/m2) were administered on day 1 and days 1-3, respectively, in the PC group. In the PT group, temozolomide (75 mg/m2) was administered concomitant with WBRT and followed by pemetrexed (900 mg/m2) plus temozolomide (150 mg/m2) on day 1 and days 1-5, respectively. The chemotherapy was repeated every 21 days for six cycles. All patients received oral folic acid (400 μg) daily and a vitamin B12 injection (1,000 μg) every 9 weeks, beginning at least 1 week before the first dose and continuing until 3 weeks after the last dose of the study treatment. If the disease became stable after therapy, the patients continued receiving high-dose pemetrexed (900 mg/m2) as maintenance therapy until eventual disease progression or the development of intolerable toxicities. Concomitant supportive therapies, such as erythropoietic agents or granulocyte colony-stimulating factors, were allowed according to the American Society of Clinical Oncology guidelines (21).
Response evaluation and statistical analysis. The patients were followed up using brain gadolinium-enhanced MRI after 2-3 cycles of treatment. The tumour responses were evaluated according to the Response Assessment in Neuro-oncology (RANO (22)) by MRI. Patients who were unable to undergo MRI due to internal metal objects or other reasons were ineligible. Treatment related toxicity was evaluated according to the National Cancer Institution Common Terminology Criteria for Adverse Events 3.0 (23). The Patients who had not experienced progression or not died during the study were censored on the date of the last tumour assessment.
The primary endpoints were ORR, PFS, and OS, secondary endpoints included safety and tolerability. ORR was based on the best response measured according to the RANO. PFS was defined as the time from treatment initiation to the first occurrence of disease progression or death. OS was defined as the time from treatment initiation to the date of death from any cause. Patients who had not experienced progression or death during the study were terminated on the date of the last tumor assessment.
Treatment related toxicity was evaluated according to the National Cancer Institution Common Terminology Criteria for Adverse Events 3.0.
Statistical analysis was carried out using Statistical Product and Service Solutions version 17 (SPSS Inc., Chicago, IL, USA). The tumour response rate was calculated as the proportion of qualified patients with a best tumour response between the arms using the Mann-Whitney U-test. OS, PFS and the differences between groups in survival were estimated using the Kaplan–Meier method.
Results
Patients. Between November 2013 and October 2015, 60 patients were enrolled into this phase II trial at three centres. Thirty-two patients were included in the PC group, and 28 patients entered the PT group. All patients had adenocarcinoma and were eligible for the statistical analysis. Their demographic and clinical characteristics are shown in Table I.
Treatment. All patients received standard WBRT (30 Gy, 10 fractions) and the PT group received concomitant temozolomide. A median of six cycles (range=2-6 cycles) of chemotherapy followed for both groups. All enrolled patients received follow-up evaluations. The follow-up rate was 100%. Seven out of the 32 (21.9%) patients in the PC group and four out of the 28 (14.3%) patients in the PT group received maintenance chemotherapy, consisting of high-dose (900 mg/m2) pemetrexed and cisplatin or other second-line therapies.
Efficacy. All 60 patients were eligible for response assessments. The 53 patients with CNS symptoms had symptom relief in both groups. Regarding the primary end-point, the PC group had an ORR [complete response (CR) plus progressive disease (PR)] of 68.8% (CR: 18.8%, PR: 50%), and the PT group had an ORR of 75% (CR: 21.4%, PR: 53.6%) (Table II). There was no statistically significant difference in response between the two groups (p=0.711).
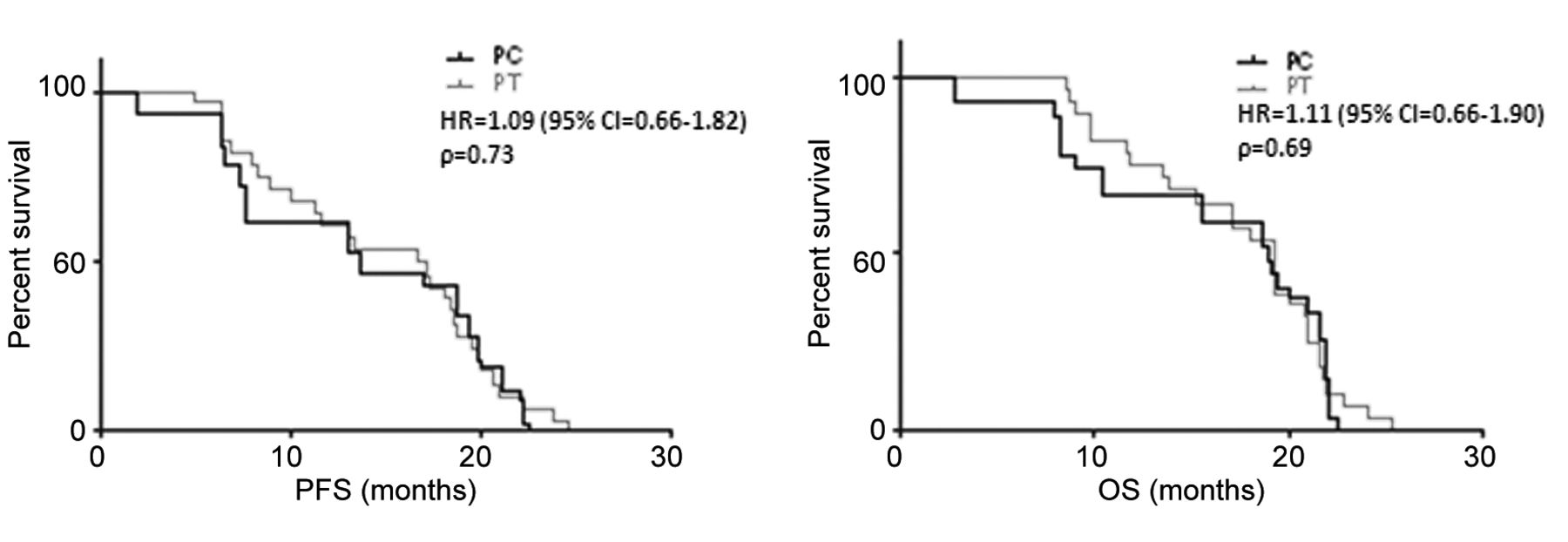
The median PFS and OS were 13.6 months (range, 2-22.5 months) and 18.9 months (range=2.8-22.5 months), respectively, in the PC group, and 16.9 months (range, 5.0-24.4 months) and 19.3 months (range, 8.5-25.3 months), respectively, in the PT group. There were no statistically significant differences in the PFS and OS between the groups (Figure 1).
By the end of the analysis, 25 patients and 22 patients had died of disease progression in the PC group and PT group, respectively; seven and six patients in the PC group and PT group, respectively, have continued follow-up. According to the PARAMOUNT result, four patients out of seven (57.1%) in the PC group received high-dose pemetrexed (900 mg/m2) as a maintenance therapy, and the other three patients (42.9%) received second-line or higher therapy due to disease progression. In the PC group, one patient out of six (16.7%) received high-dose pemetrexed (900 mg/m2) as a maintenance therapy, and the other five patients (83.3%) received second-line or higher therapy due to disease progression. Decisions regarding which therapies to use were made by the individual investigators.
Patient characteristics.
Best cerebral response rates
Safety. Toxicities are summarized in Table III. Regarding leucopenia, neutropoenia, anaemia, thrombocytopoenia, nausea/vomiting, alopecia, rash, fatigue, renal insufficiency, hepatic insufficiency, oral mycosis, constipation and diarrhoea, no side effects of grade 4 or higher were observed in either group. In the PC group, grade 3 toxicities included leucopenia, nausea/vomiting, alopecia and skin rash. In the PT group, Grade 3 toxicities only included leucopenia and nausea/vomiting. Grade 1 and 2 toxicities in the PT group were fewer than in the PC group. The results suggested that the toxicities in the PT group were fewer and milder than in the PC group. All side effects were well tolerated. Toxicity during the maintenance phase was minimal.
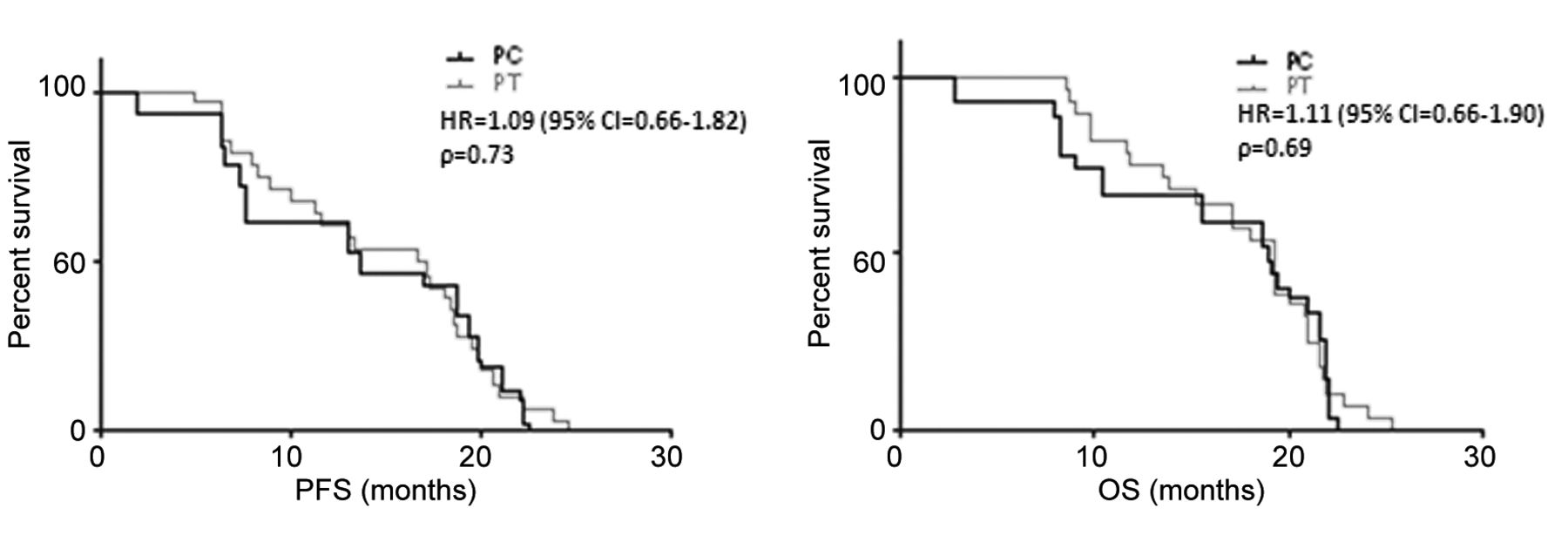
The progression-free survival (PFS) and overall survival (OS) of the group of patients treated with pemetrexed plus cisplatin (PC) versus that treated with pemetrexed plus temozolomide (PT). The median PFS and OS were 13.6 months (range=2–22.5 months) and 18.9 months (range=2.8–22.5 months), respectively, in the PC group and 16.9 months (range=5.0–24.4 months) and 19.3 months (range=8.5–25.3 months), respectively, in the PT group. There were no statistically significant differences in the PFS and OS between the groups. HR: Hazard ratio; CI, confidence interval.
Toxicities.
Discussion
This three-institution phase II study revealed that high-dose pemetrexed plus cisplatin or temozolomide was effective for NSCLC with BM, when surgery or radiosurgery was not possible. The efficacies of the two regimens did not differ. Compared to the PC regimen, the PT regimen had significantly less toxicity in patients with adenocarcinoma and BM. Our data suggest that both regimens led to better intracranial response rates, the ORRs were 68.8% in the PC group and 75% in the PT group, with a remarkably CR for BM of 18.8% (6/32) and 21.4% (6/28), respectively.
The median PFS and OS were 13.6 months (range=2-22.5 months) and 18.9 months (range=2.8-22.5 months), respectively, in the PC group and 16.9 months (range, 5.0-24.4 months) and 19.3 months (range=8.5-25.3 months), respectively, in the PT group. There were no statistically significant differences in the PFS and OS between the groups. The results were comparable to other chemotherapeutic agents used in NSCLC with BM (8, 14, 24-27). There are three possible reasons for our longer PFS and OS: (a) all patients had cytologically- or histologically-proven lung adenocarcinoma, with a statistically significantly higher mean survival time than for patients with other histologies of NSCLC with BM (28); (b) patients enrolled in this study were all eligible for WBRT with KPS≥70, which may sensitize tumours to our regimen; and (c) the synergistic efficacy of high-dose pemetrexed plus cisplatin or temozolomide after WBRT may have led to these encouraging results.
The role of chemotherapy for the treatment of BM arising from lung cancer has been limited by poor efficacy and high toxicity. Many investigators have been discouraged by the concern that chemotherapy drugs that would have efficacy against the primary tumour (e.g., lung carcinoma), such as vincristine, doxorubicin, and carboplatin, would not cross the BBB and would therefore not be active against metastatic disease (29). However, the data suggest that the BBB is disrupted when BM are present, with reports showing that the concentration of chemotherapy drugs, including platinum, is similar in intracerebral and extracerebral tumours (30, 31).
Administration of chemotherapy at full dose with maximal activity against local and micrometastatic disease is highly desirable. Pemetrexed, a multitarget antifolate chemotherapy agent, inhibits the thymidylate synthase enzyme, resulting in a decrease in the thymidine that is necessary for pyrimidine synthesis. Pemetrexed also inhibits dihydrofolate reductase and glycinamide ribonucleotide formyl transferase, the latter of which is a folate-dependent enzyme involved in purine synthesis. Supplemented with intermittent folic acid or with continuous daily multivitamins containing nutritional doses of folic acid, pemetrexed was administered up to 1,050 mg/m2 in a cancer-treatment trial (15-17).
Temozolomide has a demonstrated preclinical activity against a variety of solid tumours (32). Temozolomide is orally bioavailable and well tolerated, enabling it to be used in heavily pretreated patients and in combination with other agents. It readily crosses the BBB, achieving excellent concentrations in the brain, which makes it an attractive agent against BM (33, 34). Preclinical data indicate that combination of temozolomide with other chemotherapeutic agents may produce additive or synergistic responses (19). Temozolomide is therefore an excellent candidate for use in combination chemotherapy for the treatment of BM arising from lung cancer (35).
Pemetrexed plus cisplatin has been demonstrated to be efficacious in the first-line management of stage IV NSCLC (1, 36). Because temozolomide has several properties in the treatment of BM, we designed this study to compare the efficacy and safety between high-dose pemetrexed plus cisplatin and high-dose pemetrexed plus temozolomide.
In conclusion, treatment with pemetrexed plus temozolomide demonstrated a clinically equivalent efficacy with a significantly improved safety profile compared to pemetrexed plus cisplatin for NSCLC with BM in this study. Further randomized trials should be conducted to confirm our results.
Footnotes
↵* These Authors contributed equally to this work
Conflicts of Interest
The Authors declare that there are no conflicts of interest in regard to this study.
- Received May 19, 2017.
- Revision received July 7, 2017.
- Accepted July 7, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved





{kind=link}