


Abstract
Herein we report on a case of synchronous large gastrointestinal stromal tumor (GIST) and adenocarcinoma of the stomach treated with radical surgery following neoadjuvant therapy with imatinib mesylate. A 58-year-old man was referred to our hospital with a large mass in the peritoneal cavity. Abdominal computed tomography showed a large mass measuring 21×20×14 cm in the left upper peritoneal cavity. Esophagogastroduodenoscopy revealed a large elevated lesion in the upper body and a depressed lesion in the lower gastric body near the lesser curvature. Biopsy specimens revealed GIST in the large elevated lesion and signet-ring cell carcinoma in the depressed lesion. Because of the large size of the GIST, the patient was treated with neoadjuvant therapy with imatinib mesylate (400 mg/day) for 5 months. After confirmation of a marked decrease in tumor size following imatinib mesylate therapy, the patient underwent total gastrectomy and regional lymph-node dissection with distal pancreatectomy and splenectomy. Pathological examination confirmed the diagnosis of high-risk GIST and signet-ring cell carcinoma invading the muscularis propria with one lymph-node metastasis. At the time of writing, the patient was receiving postoperative chemotherapy using oral fluoropyrimidine (S-1) without evidence of disease recurrence for 4 months after surgery. In addition to the present case, we provide a retrospective review of another 15 patients who were diagnosed with synchronous GIST in the stomach and primary gastric adenocarcinoma.
Gastrointestinal stromal tumors (GISTs) are the most common mesenchymal tumor of the gastrointestinal (GI) tract and are believed to arise from precursor interstitial cells of Cajal. GISTs are most commonly found in the stomach, accounting for 0.1-3% of all GI malignancies, and can be characterized at the molecular level by activating mutations in the receptor tyrosine kinases KIT proto-oncogene receptor tyrosine kinase (KIT) and platelet-derived growth factor receptor-α (PDGFRA) (1). Adenocarcinoma is the most common histological type of malignancy in the stomach. Adenocarcinoma can coexist with another synchronous tumor of a different histological type in a different part of the stomach. The synchronous occurrence of tumors of different histological types in the stomach has recently become the subject of increasing interest. Synchronous occurrence of GIST and adenocarcinoma in the stomach is uncommon, with only a few patients with GIST and synchronous gastric cancer described in the literature.
A novel treatment strategy for locally advanced or metastatic GIST is the use of different tyrosine kinase inhibitors (e.g. imatinib) to inhibit growth factor receptor c-KIT tyrosine kinase. Neoadjuvant treatment in patients who present with inoperable GISTs may enable successful and less radical surgery after cytoreduction. Herein we report a case of a patient with synchronous large GIST and adenocarcinoma of the stomach treated by surgery after 5 months of neoadjuvant therapy with imatinib mesylate, a tyrosine kinase inhibitor. In addition, we review previously published case reports of synchronous large GIST and adenocarcinoma of the stomach.
Case Report
A 58-year-old Japanese man visited his local doctor complaining of abdominal discomfort. Abdominal ultrasonography revealed a large mass in the peritoneal cavity and the patient was referred to our hospital. Until that point, the patient had been well with an unremarkable history. Upon presentation, the laboratory findings were as follows: normal red blood cell count (400×104/mm3; normal range 400-552×104/mm3); increased white blood cell count (14.4×103 /mm3; normal range 3.6-9.6×103/mm3); normal platelet count (33.6×104/mm3; normal range 14.8-33.9×104 /mm3); low total protein (6.4 g/dl; normal range 6.7-8.1 g/dl), low albumin (3.5 g/dl; normal range 3.9-4.9 g/dl); high lactate dehydrogenase (314 U/l; normal range 119-229 U/l); and high C-reactive protein (10.5 mg/dl; normal value, <0.30 mg/dl). However, levels of alanine aminotransferase, aspartate aminotransferase, total bilirubin, and serum creatinine were within normal limits, as were serum carcinoembryonic antigen and cancer antigen 19-9. The patient was subsequently admitted to our hospital complaining of right epigastric pain.

Computed tomographic image prior to imatinib mesylate therapy, showing a 21-cm diameter mass in the left upper peritoneal cavity.
Abdominal contrast-enhanced computed tomography (CT) showed a large, well-defined mass measuring 21×20×14 cm, with a heterogeneous component occupying the left upper peritoneal cavity, compressing the liver and pancreas (Figure 1). Esophagogastroduodenoscopy (EGD) revealed a large elevated lesion with a deep central ulcer in the upper body (Figure 2A) and a depressed lesion with an indistinct margin on the lower gastric body near the lesser curvature (Figure 2B). Histopathological analysis of an endoscopic biopsy sample from the large elevated lesion revealed GIST, whereas a biopsy sample from the depressed lesion revealed signet-ring cell carcinoma (SRCC). There was no evidence of metastatic lesions in other organs. We made a clinical diagnosis of synchronous large GIST and adenocarcinoma in the stomach.
Since it seemed unlikely that complete resection would be possible because of the large size of the tumor, the patient was treated with neoadjuvant therapy of imatinib mesylate (400 mg/day) for 5 months. After treatment, a CT scan confirmed a partial response, with a decrease in tumor dimensions to 9.1×8.3×7.5 cm, without any evidence of metastases (Figure 3). The patient then underwent a total gastrectomy and regional lymph-node dissection with distal pancreatectomy and splenectomy. Intraoperatively, there was no peritoneal dissemination and a complete resection was performed by partial resection of the diaphragm because of tumor invasion. Gross examination of the resected specimen showed a well-circumscribed, elevated lesion in the posterior wall of the fornix (Figure 4, arrow) and a depressed lesion measuring 9.0×7.5 cm (Figure 4, arrowhead). Pathological examination confirmed the diagnosis of high risk GIST for the elevated lesion and SRCC for the depressed lesion, which had invaded the muscularis propria with one lymph node metastasis.
During the postoperative course, the patient developed a minor pancreatic fistula that was treated conservatively using tube drainage. In addition, the patient has been receiving postoperative chemotherapy with oral fluoropyrimidine (S-1) without evidence of disease recurrence for 4 months after surgery.
Discussion
Herein we describe a rare case of a patient with synchronous development of adenocarcinoma and GIST in the stomach treated by radical resection following neoadjuvant imatinib mesylate, administered because of the large size of the tumor. A search of the English language literature published between 2000 and 2016 was conducted using the Medline and PubMed databases for articles on the synchronous occurrence of GIST in the stomach and primary gastric adenocarcinoma with the key words “gastrointestinal stromal tumor”, “adenocarcinoma”, and “treatment”. Data on age, gender, tumor location, tumor size, depth of invasion, histological type, staging, treatment, and outcome for each patient were obtained. The clinicopathological features of the 15 previously reported cases (2-13) and the present case are listed in Table I. The median age of patients was 70 years (range=52-80 years) and there was a male predominance, with a male to female ratio of 11:5.
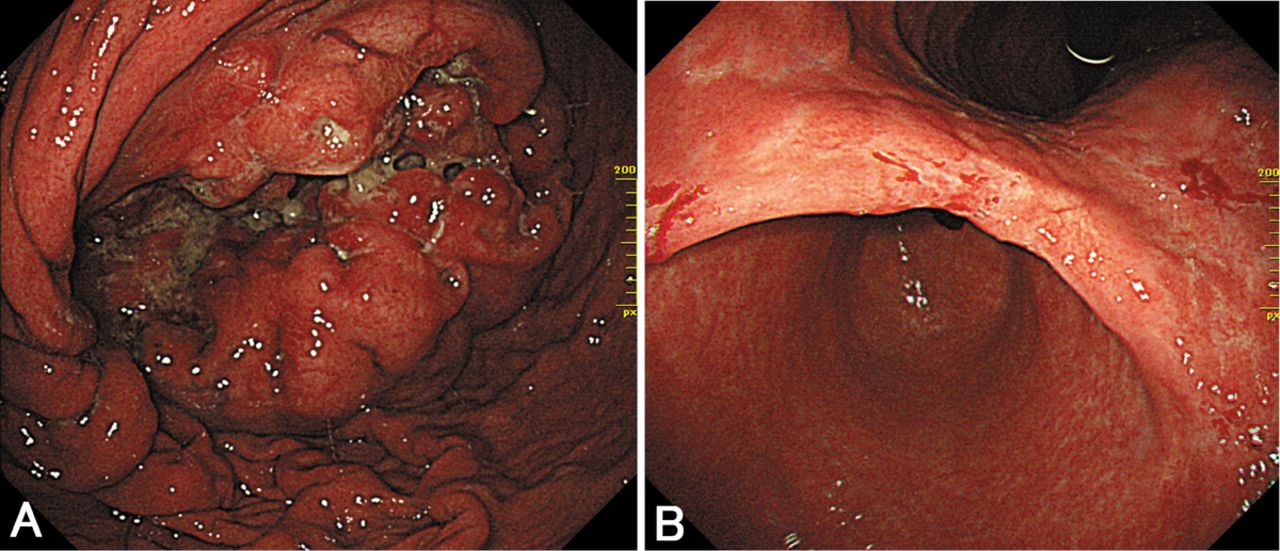
Esophagogastroduodenoscopy prior to imatinib mesylate therapy, showing gastrointestinal stromal tumor (A) and adenocarcinoma (B) in the stomach.

Computed tomographic image after 5 months of neoadjuvant imatinib mesylate therapy, showing a marked decrease in the size of the tumor.

Macroscopic appearance of the resected specimen showing the gastrointestinal tumor (arrow) and the adenocarcinoma (arrowheads).
Reported cases of synchronous gastrointestinal tumor and adenocarcinoma in the stomach.
GIST lesions in the upper one-third of the stomach were reported in five cases, four patients had lesions in the middle one-third of the stomach, and three had lesions in the lower one-third of the stomach. The median tumor size for GIST was 1.4 cm (range=0.3-21 cm), and this was smaller than the median tumor size of the gastric adenocarcinoma (4.9 cm; range=1.0-10.2 cm). Only three patients had a larger GIST than adenocarcinoma, and the patient with the largest GIST was the present case. The gastric adenocarcinomas had invaded to varying depths, with lesions confined to the mucosa in one patient, but invading the submucosa in four cases, the muscularis propria in two cases, the serosa in five cases, and penetrating the serosa in one case. Histological analysis of gastric adenocarcinoma revealed six intestinal-type and six diffuse-type carcinomas. Treatment consisted of total gastrectomy in five patients, distal gastrectomy in five patients, proximal gastrectomy in one patient, and partial gastrectomy in one patient. To the best of our knowledge, the present case is the first case of synchronous GIST and adenocarcinoma in the stomach treated with radical surgery after a course of neoadjuvant imatinib mesylate therapy.
Helicobacter pylori has been confirmed to play a key pathogenic role in a number of diseases, including gastric cancer, malignant lymphoma, and other non-GI entities. Despite being rare, the clinicopathological characteristics of synchronous primary gastric adenocarcinoma and lymphoma have been reported previously (14, 15). However, there is no evidence that H. pylori infection is linked to the development of GISTs, although it has been implicated in the development of gastric cancer. With regard to the pathogenesis of the synchronous occurrence of GIST and adenocarcinoma, although it seems to be simply coincidence, the development of these tumors may involve common carcinogenic agents.
A previous report on synchronous gastric adenocarcinoma and gastric lymphoma found that the prognosis for this entity may depend more on the behavior of the adenocarcinoma than on the lymphoma (16, 17). In the case of gastric adenocarcinoma with GIST, the treatment regimen and therapeutic outcomes may depend on the status of the adenocarcinoma. If the size of the tumor is large without any distant metastases, a surgical approach should be considered carefully because of the possibility of incomplete resection. In the present case, because the size of the GIST had decreased in response to imatinib mesylate, complete resection during total gastrectomy with distal pancreatectomy was chosen as the best treatment option. In cases such as the one reported herein, neoadjuvant therapy of imatinib mesylate may be a promising option enabling subsequent successful resection.
In conclusion, the present case indicates that neoadjuvant therapy with imatinib mesylate may be an effective treatment for patients with synchronous large GIST and gastric adenocarcinoma in order to achieve subsequent complete radical resection. Further studies and accumulation of additional cases are needed to confirm the ideal treatment for this entity.
Footnotes
Financial Support
None.
Conflicts of Interest
None.
- Received February 3, 2016.
- Revision received March 17, 2016.
- Accepted March 22, 2016.
- Copyright© 2016 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}
{kind=link}
{kind=link}
{kind=link}