


Abstract
Pertuzumab (Perjeta®) represents the first monoclonal antibody in a new class of agents known as dimerization inhibitors. Pertuzumab was recently approved for the treatment of Human Epidermal Receptor 2 (HER2)-positive breast cancer in the metastatic and neo-adjuvant setting. This approval for first-line therapy for metastatic breast cancer was based on the results of a large randomized multicenter phase III trial showing a significant improvement in overall survival when pertuzumab was combined with trastuzumab and docetaxel in HER2-positive metastatic breast cancer. In the neoadjuvant setting, dual HER2 blockade by trastuzumab and pertuzumab improved the complete pathological response rate. However, pertuzumab development was not confined to breast cancer and in the present article, we focus on pertuzumab data for solid tumors other than breast cancer, and review the biological rationale for its use, the published pre-clinical and clinical evidence, as well ongoing trials.
HER Receptor Family: An Established Drug Target In Solid Tumors
The role of human epidermal growth factor receptors (HER) in solid tumors has been extensively studied over the past decade (1-5). Several malignancies are associated with increased expression and mutations of HER family members (6-8). The HER family comprises of four members: HER2, HER1 (also known as EGFR, epidermal growth factor receptor), HER3, and HER4. HER2 gene amplification or overexpression occurs in approximately 20% of breast and gastric cancer cases (9, 10). EGFR is a key target in colorectal cancer and in non-small cell lung cancer (NSCLC). All family members share a similar transmembrane glycoprotein structure: a glycosylated extracellular domain (ECD) with four sub-domains allowing-binding of different ligands and receptor dimerization; a hydrophobic transmembrane domain for anchoring in the cell membrane; and an intracellular domain endowed with tyrosine kinase activity. The ligand binding to the ECD of these receptors (except HER2) triggers a large conformational change in the ECD, which leads to the exposure of a dimerization arm in its domain II. The ligand binding results in either homodimerization or heterodimerization between two different HERs. Dimerization induces tyrosine kinase phosphorylation and downstream signaling onto the mitogen-activated protein (MAP) kinase, the phospholipase C (PLCγ), and phosphoinositide-3 kinases (PI3K) cascades, leading to cell migration and proliferation, as well as cell survival.
All HER family members play a key role in carcinogenesis in multiple types of solid tumors, particularly of breast, colorectal and ovarian cancer, but also prostate, gastric and NSCLC. However, within the HER family, HER2 differs from its homologs because no specific ligand has yet been identified and HER2 is constitutively present at the cell surface in an active conformation. HER2 is, therefore, considered as the preferential heterodimerization partner for other HER proteins. In contrast, HER3 accepts many ligands, but has only a weak intracellular tyrosine kinase activity. Hence, the dimers vary in their signaling potencies, with HER2 and HER3 possessing the strongest mitogenic activity, particularly through the activation of the PI3K/AKT pathway. HER dimerization is a key process for the activation of different signaling pathways and was, therefore, considered a potential target for new drug development (11, 12).
Since the approval of trastuzumab in 1998, there have been significant advances over our knowledge regarding the biology of HER2-positive breast cancer, as well as of the molecular mechanism of trastuzumab activity and the development of resistance to the drug. Trastuzumab was for nearly 15 years the only available HER2 antibody. The lack of HER2 gene amplification or overexpression was rapidly identified as a predictive biomarker of trastuzumab inefficacy in HER2-negative breast cancer. Trastuzumab improved survival in many trials and was considered as the standard of care in neoadjuvant, adjuvant as well as metastatic HER2-positive breast cancer (13-17).
However, trastuzumab failed to lead to any significant response or survival improvement in parents with other types of solid tumor, except gastric cancer. A hypothesis for these disappointing results is the lack of gene amplification or overexpression in most of these solid tumors (18, 19). In addition, some patients have primary resistance or will develop secondary mechanisms of resistance to trastuzumab (20). One of the most frequent mechanisms of resistance is HER3 overexpression. Indeed, although trastuzumab binds to ECD domain IV of HER2, and blocks downstream signaling, it is not effective in inhibiting heterodimerization, especially regarding the most potent HER2–HER3 dimer. As a consequence, blockade of the HER2–HER3 dimerization was considered an attractive target. These findings led to the development of a novel class of HER2-targeted therapy.
Rationale for Pertuzumab Development
Pertuzumab is the first antibody from a novel therapeutic class called dimerization inhibitors. Pertuzumab is a recombinant humanized monoclonal antibody that binds to the extracellular dimerization domain II of HER2, targeting a different epitope from that of trastuzumab. The binding of the drug to the dimerization domain prevents the formation of the ligand-induced HER2 heterodimer, which is the most potent dimer in activating mitogenic and survival signaling pathways. Pertuzumab's mechanism of action is complementary to that of trastuzumab, which blocks the signaling pathway without affecting dimerization (Figure 1).
In addition, as an antibody, the antitumor activity of pertuzumab is partially linked to immune system activation, in particular of natural killer cells through antibody-dependent cellular cytotoxicity.
Taken together, these data emphasize on the properties and unique mechanisms of action of pertuzumab and support its potential efficacy in solid tumors even lacking HER2 overexpression or gene amplification. Indeed, whereas pertuzumab has shown an outstanding activity in HER2-positive breast cancer, in the neoadjuvant and the metastatic setting, it may also be a promising drug for other solid tumors (21).
Pertuzumab from Preclinical Data to Phase I Trials
Pre-clinical experiments have shown synergistic antitumor activity using pertuzumab as a single agent or in combination with trastuzumab in xenograft models of lung, prostate, ovarian, colorectal, gastric or breast cancer (22-24). Based on these results, pertuzumab was developed in phase I trials (with trastuzumab), as well as a single agent, and in combination with cytotoxic drugs (docetaxel and capecitabine) and targeted therapies (Trastuzumab-DM1, EGFR inhibitors) (Table I). Encouraging results have been reported, with some partial responses and long-term responders (stabilization >2.5 months in prostate, ovarian, colorectal and lung cancer). Overall, pertuzumab was well- tolerated, with grade 1-2 rash, vomiting, diarrhea and asthenia as the most common adverse events. No maximum tolerated dose was reached in any of the trials and the recommended dose for future studies was based on pharmacokinetic results. These encouraging results from the pre-clinical data, along with the safety results obtained in the phase I trials led to pertuzumab development in many types of solid tumors, including gastric colorectal cancer, NSCLC, ovarian and prostate cancer, as a single agent or in combination. Development for therapy of other tumor types was, however, prematurely stopped regarding pre-clinical and phase I results.
Pertuzumab in Phase II and III Trials
Gastric cancer. The prognosis for advanced or metastatic gastric cancer remains poor, with a median overall survival not exceeding 6 to 11 months and with few efficacious therapeutic options (25). In this setting, many trials have been conducted to identify new ‘druggable’ targets in order to improve patients' outcome. HER2 gene amplification or overexpression has been known since 1986 and occurs in 16-22% of intestinal gastric cancer subtypes and 6-7% of diffuse subtypes (9, 26). Pre-clinical data, as well as results from phase I trials assessing trastuzumab in HER2-positive gastric cancer, very early suggested the potential efficacy of trastuzumab in gastric cancer (27, 28).
These data led to a randomized phase III trial in HER2-positive gastric and gastroesophageal junction cancer. This study randomized 584 patients in two arms: an arm with standard chemotherapy (cisplatin plus 5-fluorouracil/capecitabine) and an experimental arm combining trastuzumab with chemotherapy. Overall survival was significantly improved in the experimental arm: 13.8 versus 11.1 months [hazard ratio (HR)=0.74, 95% confidence interval (CI)=0.60 to 0.90, p=0.0046) with no increase in toxicity (29). These results led to trastuzumab approval for patients with first-line, HER2-positive metastatic gastric and gastroesophageal junction cancer in combination with a cisplatin-based chemotherapy.
Pre-clinical studies in gastric cancer xenograft models have demonstrated the synergistic effect of combining pertuzumab with trastuzumab (23). These data, along with encouraging results from pertuzumab/trastuzumab association in metastatic HER2-positive breast cancer, supported the development of a randomized open-label multi-center phase IIa study. The primary end-point was to investigate the pharmacokinetics and safety of two different doses (840 mg and 420 mg) of pertuzumab in combination with trastuzumab and a standard cisplatin/capecitabine chemotherapy in the first-line treatment of HER2-positive gastric cancer. Based on the safety profile and pharmakinetic data, the recommended dose of pertuzumab for a further phase III trial was 840 mg every three weeks. At the interim safety assessment that was recently reported by Yoon-Koo et al., no unexpected toxicity was found (30). The most frequent adverse events of grade 3 or more were diarrhea, neutropenia, hyponatremia and stomatitis. In gastric cancer, pertuzumab development is on-going with a multi-center, international randomized phase III trial (clinicaltrials.gov identifier NCT01774786) that is currently recruiting patients, whose primary end-point is overall survival. The trial investigates the standard cisplatin/fluoropyrimidine (either 5-fluorouracil or capecitabine) and trastuzumab, compared to the same regimen plus pertuzumab. Secondary end-points include progression-free survival, objective response rate, duration of response, clinical benefit rate, safety and pharmacokinetics. The first results are expected in 2014.
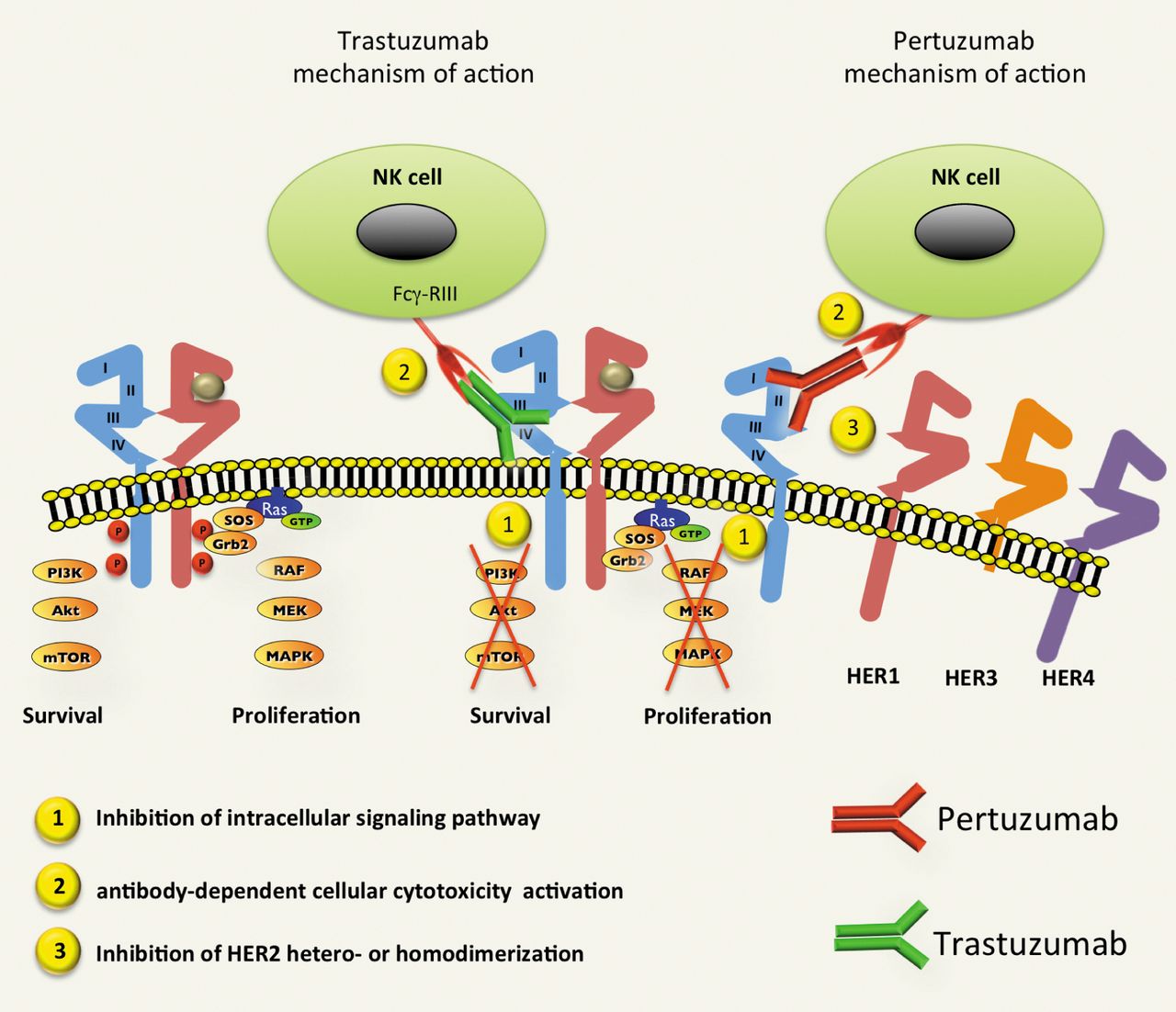
Mechanism of action of trastuzumab and pertuzumab. Trastuzumab binds to the extracellular domain IV of HER2, and blocks downstream signaling pathways (RAS/RAF/MAPK and PI3K/Akt/mTOR), without affecting dimerization. Pertuzumab, targets the dimerization domain (domain II) and prevents the formation of the ligand-induced HER2 heterodimer, which is the most potent dimer in activating mitogenic and survival signaling pathways. In addition, as an antibody, the antitumor activity of pertuzumab and trastuzumab is partially linked to immune system activation, in particular with natural killer cells through antibody-dependent cellular cytotoxicity. NK: natural killer; Fcγ R III: Fcγ receptor III.
Colorectal cancer. EGFR is a key element of colorectal carcinogenesis by regulating signaling pathways involved in proliferation, cell survival and tumor invasion. The effectiveness of therapeutic monoclonal antibodies to EGFR has been demonstrated by numerous phase III trials in patients with metastatic colorectal cancer, not harbouring RAS mutations (31, 32). However, all patients will eventually cease to respond to anti-EGFR treatment by the development of different resistance mechanisms, among which is HER3 overexpression, as EGFR inhibition induces HER3 and HER2–HER3 heterodimers (33). As HER2–HER3 activates the MAPK signaling pathway despite blockade of EGFR, pertuzumab might be a promising drug to overcome heterodimer-mediated anti-EGFR resistance. A phase I/II trial has been conducted to assess the efficacy and safety of cetuximab anti-EGFR antibody approved in colorectal cancer and other solid tumors) and pertuzumab combination in patients with cetuximab-resistant metastatic colorectal cancer (34). The study was prematurely stopped due to severe toxicity, including grade 3 skin rash, mucositis and diarrhea. Despite an encouraging response rate of 14% in this setting, the development of the cetuximab/pertuzumab combination was stopped in the light of overlapping toxicity profiles of the two drugs.
Main clinical trials with pertuzumab in solid tumors (other than breast cancer).
NSCLC. Over the past decade, the management of NSCLC has dramatically changed thanks to a better knowledge of molecular biology and the identification of new therapeutic targets including EGFR mutations. Indeed, the EGFR signaling pathway plays a key role in NSCLC carcinogenesis. EGFR overexpression takes place in around 60% of all NSCLC and is associated with a poor prognosis (35). Activating EGFR mutations have been identified in 10 to 20% of lung adenocarcinomas and tyrosine kinase inhibitors targeting EGFR (EGFR-TKI) led to objective response rate, progression-free survival and overall survival improvements in several large randomized trials (36-38). HER2 is expressed in nearly 40% of NSCLC but is overexpressed in only 2 to 5% of cases, jeopardizing the development anti-HER2 therapies in NSCLC. However, pertuzumab might be of interest since it has some antitumor activity even in tumors expressing low HER2 levels (score 1+ or 2+).
Very few clinical studies have evaluated the antitumor activity of pertuzumab in NSCLC. Pre-clinical studies confirmed its antitumor activity in two models of lung cancer xenografts with different HER2 expression levels (39). These pre-clinical data, along with the crucial role of the EGFR signaling pathway, especially HER1–HER2 heterodimer, led to the further clinical development of pertuzumab in NSCLC. The phase I results confirmed the preclinical findings, obtaining prolonged stabilization (4.1 months) in one heavily pretreated patient with NSCLC (40).
A first phase II study was therefore undertaken in 33 patients with metastatic NSCLC previously treated with chemotherapy (41). All patients were treated with pertuzumab monotherapy. The results were disappointing, without any objective response whatever the EGFR or HER2 status. Similar results were reported in another study by Herbst et al. in 43 patients treated with single-agent pertuzumab. Of the 43 patients (all previously treated with at least one prior chemotherapy regimen) no objective response and only a few cases of stable disease were observed (progression-free survival=6.1 weeks) (42).
In the light of these data with single-agent pertuzumab, the drug was further developed in combination with erlotinib in second- and third-line treatment. Indeed, pre-clinical data suggested the involvement of HER1–HER2 dimerization in the mechanisms of resistance to EGFR-TKI (41). Hence the addition of pertuzumab to EGFR inhibitor can possibly circumvent EGFR-TKI resistance by blocking HER1–HER2 dimerization and inhibiting the downstream signaling pathway. A phase I study was conducted in 15 patients to determine the optimal dose of erlotinib and pertuzumab (43). The authors report encouraging results, with a partial response rate of 20% and a stability of more than six months was achieved in one patient. No dose-limiting toxicity was reported. Overall, the combination of pertuzumab with erlotinib was well-tolerated, with most common adverse events being grade 2 or 3 skin rash and grade 1 or 2 diarrhea. The phase II trial (clinicaltrials.gov identifier NCT00855894) combining erlotinib (150 mg/d, secondarily reduced to 100 mg/d) and pertuzumab (420 mg/ every three weeks) was recently closed to recruitment and the results are pending.
Prostate cancer. Prostate cancer is the most common malignancy in men, with more than 200,000 new cases per year in the US, accounting for 30,000 deaths per year. The treatment of metastatic prostate cancer is based on androgen deprivation until disease becomes resistant to castration. Substantial advances have been made over the past decade in metastatic prostate cancer treatment with the arrival of new molecules targeting the androgen receptor axis, especially in patients with castration-resistant prostate cancer (CRPC) (41). However, the role of HER2 in prostate cancer, especially its prognostic value, remains uncertain.
Pre-clinical data showed that adding trastuzumab to hormonal therapy could delay the development of resistance to castration, supposedly due to a cross-talk between the androgen receptor and HER2-induced signaling pathways (45). Several studies have shown that HER family receptors can activate downstream signaling pathways, such as MAPK or AKT/mammalian target of rapamycin (mTOR) pathways, and ligand-independent androgen receptor thereby providing a mechanism to exhaust androgen deprivation therapy and allowing cells to become androgen-independent (46, 47). However, despite all these pre-clinical observations, clinical studies have not yet demonstrated any benefit of trastuzumab in prostate cancer regardless of stage or level of androgen dependence until investigators focused on pertuzumab.
Indeed, phase I results were promising, with one partial response and three cases of stable disease (2.6, 2.7 and 5.5 months) among five heavily pretreated patients with prostate cancer (40). Two phase II trials were undertaken to confirm these results. The first study assessed the efficacy and safety of pertuzumab as a single agent at two different doses (420 mg versus 1,050 mg) in 68 patients with CRPC before any chemotherapy (48). Unfortunately, no objective response, defined as prostate specific antigen (PSA) decline of >50%, was observed in that study. A similar study was conducted in a population of patients with CRPC previously treated with docetaxel. The 41 patients included in the study received pertuzumab monotherapy with a conventional dose of 420 mg after a loading dose of 840 mg (49). Again, no objective responses were reported. These disappointing results have definitively condemned the development of pertuzumab for this condition. The lack of biomarkers in order to select the population most likely to benefit from pertuzumab is certainly the main reason for these two failures.
Ovarian cancer. In recent years, landmark advances have been made towards treatment of ovarian cancer with the development of many novel therapies targeting various signaling pathways, including HER and AKT/mTOR (50). The HER signaling pathway is of particular interest in the light of its involvment in ovarian cancer pathogenesis. Many ovarian tumor samples express all members of the HER family and HER2 activation is detectable in a subset of tumors, including tumors with non-amplified HER2 genes and lower levels of HER2 expression (51). Several consistent data from the literature have stressed on the prognostic role of HER1 and HER2 overexpression in ovarian cancer (52). HER2 as the preferred dimerization partner (HER1–HER2, and HER2–HER3 dimers), activates intracellular signaling pathways, driving ovarian tumor cell proliferation even in the absence of HER2 overexpression. Several studies have been conducted to investigate the efficacy of trastuzumab in ovarian cancer. The results were disappointing, probably because of the low percentage of HER2 overexpression in ovarian cancer, ranging from 6-12% depending on the study. Indeed, trastuzumab efficacy requires HER2 overexpression or gene amplification, and response rates were approximatively 7% with trastuzumab single-agent therapy (53). Nevertheless, through its unique mechanism of action, pertuzumab may show some activity in tumors lacking HER2 overexpression. The efficacy and safety of pertuzumab was, therefore, studied in three phase II trials in ovarian cancer at different stages.
Gordon et al. enrolled 123 heavily pre-treated (average of five prior chemotherapy regimens) patients with platinum-resistant ovarian cancer. Patients were randomized between pertuzumab at a dose of 420 mg every three weeks after a loading dose of 840 mg and pertuzumab at a fixed dose of 1,050 mg. The overall response rate was only 4.3% (3.6% for the ’standard’ arm and 4.8% for the fixed dose of pertuzumab) but 41% of patients achieved prolonged stable disease and biological responses. No unexpected adverse event was reported. Exploratory biomarker analysis suggests that the phosphorylated HER2 status could be a predictor of clinical benefit in pertuzumab-treated patients (54).
Another randomized, placebo-controlled, double-blind, multi-center phase II trial enrolled 130 patients with platinum-resistant disease given either an experimental arm combining gemcitabine-plus-pertuzumab, or gemcitabine-plus-placebo. The primary study end-point, which was progression-free survival improvement, was not reached (2.0 versus 2.9 months; HR=0.66, 95% CI=0.43-1.03, p=0.07). The objective response rate was 4.6% in the gemcitabine plus placebo arm (three partial responses) versus 13.8% in the gemcitabine plus pertuzumab arm (nine partial responses). However, by analyzing the progression-free survival based on HER3 mRNA expression rate, results became significantly different in favor of the pertuzumab regimen (1.3 versus 5.3 months; HR=0.32, 95% CI=0.17-0.59, p=0.0002) for patients with low versus high HER3 mRNA expression (55). In terms of toxicity, the authors reported a higher rate of grade 3-4 neutropenia, diarrhea and back pain in the gemcitabine–pertuzumab arm. Similar results were recently reported by Kaye et al. in a third phase II study conducted in a population of patients with platinum-sensitive ovarian cancer. The 149 patients in the trial all received carboplatin chemotherapy combined with either paclitaxel (2/3) or gemcitabine (1/3) and were randomized to receive additional placebo or pertuzumab. No significant response rate or progression-free survival improvement was obtained by the addition of pertuzumab (56). However, the low expression of HER3 mRNA was again associated with a progression-free survival benefit by adding pertuzumab, although the difference was not significant. Low HER3 mRNA levels might thus be a predictor of response to pertuzumab. The underlying hypothesis is that low HER3 mRNA levels would surrogate the activation of the signaling pathway and thus HER2–HER3 dimerization activity, targeted by pertuzumab. Recent preclinical data confirmed this hypothesis, suggesting that the expression of HER3 mRNA, and to a lesser extent of HER2, could be considered as a predictive factor for pertuzumab response (57). Indeed, HER2 and HER3 mRNA expression is down-regulated by the activation of the HER signaling pathway via heregulin and EGF, two ligands of HER3 and HER1, respectively. This hypothesis needs to be confirmed prospectively and a phase III trial is currently ongoing in ovarian cancer (clinicaltrials.gov identifier NCT01684878), for which eligibility criteria include low HER3 mRNA level. The primary end-point is overall survival, to be improved by the addition of pertuzumab to a standard chemotherapy with paclitaxel or topotecan.
Conclusion
Pertuzumab has demonstrated efficacy in metastatic breast cancer for which it recently received approval. Its development in therapy of other types of solid tumor is ongoing, and has shown interesting results. Indeed, confirmation of the more promising results that will perhaps modify our current practice is awaited in gastric and gastroesophageal junction tumors, as well as in advanced ovarian cancer. The identification of biomarkers, such as the level of expression of HER3 mRNA in ovarian cancer, appears to be essential for a better identification of patients likely to benefit from the drug. If further data confirm the relevance of selecting patients with low HER3 mRNA for best efficacy of pertuzumab, selecting tumors for which results were so far disappointing might reactivate discarded clinical research trials.
Indeed, drug-induced and sometimes unexpected positive feedback of tumor growth is of crucial importance in the onset of resistance to targeted therapies. Given the existing cross-talk between druggable membrane receptors and HER-induced signaling, it is likely that blocking receptor dimerization be an outstanding goal for combining pertuzumab with other therapeutic molecules. This highlights the outstanding importance of combining ancillary biological studies with clinical research, especially in the field of targeted therapies.
Acknowledgements
None.
Footnotes
-
This article is freely accessible online.
-
Disclosures
The Authors have nothing to disclose regarding this article.
- Received January 14, 2014.
- Revision received February 18, 2014.
- Accepted February 20, 2014.
- Copyright© 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved





{kind=link}