


Abstract
Aim: The present study investigated the visualization of the arterial networks in the stomach (ANS) during gastric tube (GT) creation using indocyanine green fluorescence and the HyperEye Medical System (HEMS), and the feasibility of the HEMS-line-marking method (LMM). Patients and Methods: We reviewed 51 consecutive patients who had undergone esophageal surgery with GT reconstruction. Patients for whom the HEMS was deployed after GT creation to confirm the anastomosed area's blood supply formed the control group (n=28). Patients for whom the HEMS was deployed before GT creation to confirm and mark the ANS border comprised the HEMS-LMM group (n=23). Results: The HEMS-LMM visualized the ANS border, and the leakage rate decreased from 17.9% to 4.4% (p=0.204). Conclusion: The HEMS-LMM is safe and feasible for visualizing the blood supply border of the right gastroepiploic artery and the ANS before GT creation during esophageal surgery, and it might reduce leakage in esophageal surgery.
Anastomotic leakage and necrosis of the reconstructed conduit are among the most challenging complications associated with esophageal surgery (1). As a consequence of the rich arterial networks in the stomach (ANS), gastric tube (GT) reconstruction is the most popular method to overcome the complications associated with esophagectomies (2). Although a good arterial blood supply to the GT is essential to avoid leakage, the conventional methods used to assess the blood supply to the GT, such as those associated with color and arterial palpation, are often ambiguous.
The indocyanine green (ICG) fluorescence method has been recently used during gastrointestinal tract, cardiovascular, and breast cancer surgery to visualize blood supplies or lymphatic flows (3-6). The HyperEye Medical System (HEMS) (Mizuho Ikakogyo Co., Ltd, Tokyo, Japan) is an ICG-based camera system that can simultaneously detect color and near-infrared rays that range from 380 to 1,200 nm (7). We have been performing ICG fluorescence assessments using the HEMS, since 2011, to visualize the blood supply to the GT during esophageal surgery, and we have used the HEMS after creating the GT to identify suitable anastomosis points on the side of the greater curvature of the stomach. However, although we have used the HEMS, we have experienced partial GT necrosis and leakage, which were likely to have been caused by interruptions in the ANS during GT creation (Figure 1). We have, therefore, devised a new method for creating GT that preserves the ANS and involves using the HEMS before the GT is created, and the boundary of the blood supply is marked using a HEMS-line-marking method (HEMS-LMM). This retrospective study aimed to evaluate the feasibility of the HEMS-LMM.
Patients and Methods
Patients and surgical procedures. We retrospectively reviewed 51 consecutive patients who had undergone esophagectomies or esophageal bypasses that were followed by pulling the GTs up towards the neck and cervical anastomoses using a circular stapler at our institution between September 2011 and March 2015. From 2011 to 2014, the HEMS was deployed in 28 patients after the GT had been created, and these patients comprised the control group. Since 2014 and following our experience of GT necrosis, the HEMS-LMM has been deployed before GT creation, and 23 patients comprised the HEMS-LMM group. All patients had esophageal cancer, and one patient in the control group had an esophageal rupture caused by a thoracic aortic aneurysm.
The esophagectomy comprised of a neck dissection, thoracoscopic esophagectomy with the patient in the prone position, laparoscopic gastric mobilization (LGM), GT creation, and anastomosis creation at the neck. During the LGM, the left gastroepiploic artery (GEA) and left gastric artery were divided, and the right GEA was carefully preserved. After the LGM, we performed a small-incision laparotomy and removed the esophagus and the stomach. The esophageal bypass procedure comprised a cervical esophageal resection and gastric mobilization without a dissection of the lymph nodes.

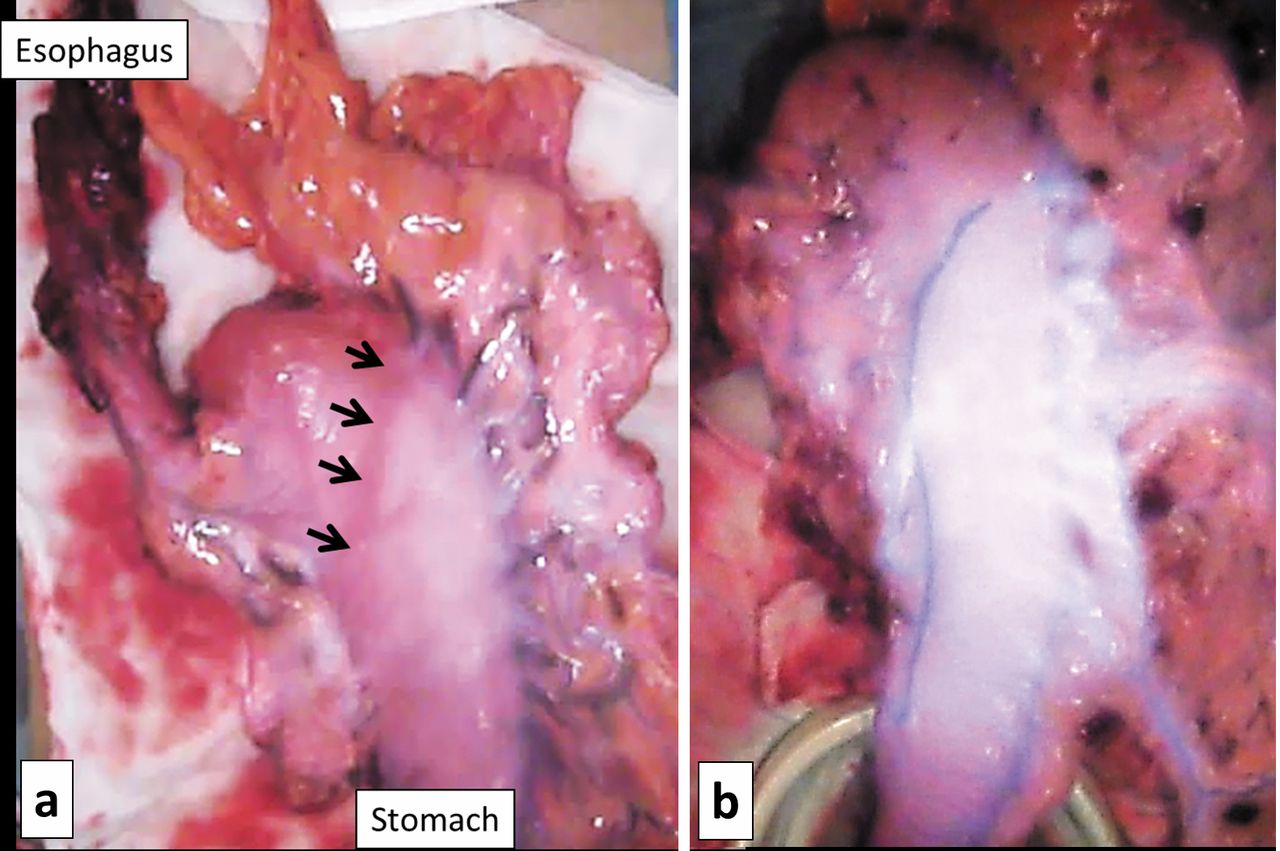
A HyperEye Medical System (HEMS) image after gastric tube (GT) creation. The HEMS image shows a low level of indocyanine green fluorescence on the lesser curvature side of the GT (arrow), which was in contrast to the estimated anastomosis area (dotted arrow) (a). An area of good fluorescence spread via the greater curvature of the GT, however, the area of poor fluorescence remained, and this patient showed partial GT necrosis this area (b).
HyperEye Medical System-line-marking method. We performed the ICG fluorescence test using the HEMS. The anesthesiologist injected 2 mL (5 mg) of ICG dye through a central vein catheter and flash-injected 10 mL of saline. The blood flow to the stomach via the right GEA was visualized on a color monitor. By simultaneously comparing the image on the color monitor with the actual surgical field in the well-lit operating room, we could detect an area in the stomach that had a good arterial blood supply, then we marked the border of the ANS as a cutting line using linear staplers, and we identified a suitable anastomosis point on the side of the stomach with the greater curvature (Figure 2). After creating the GT using linear staplers, we pulled it up towards the neck, and we used the HEMS to check the anastomosis point. Finally, we created the cervical esophagogastric tube end-to-side anastomosis using a circular stapler. We then inserted a nasogastric tube through the anastomosis and closed the entry hole of the GT using a linear stapler. A feeding jejunostomy catheter was inserted into all of the patients.
After surgery, the patients were transferred to the intensive care unit. The day after surgery, the patients were weaned-off the ventilator and they were returned to the ward, if their overall condition was good. Seven days after surgery oral intakes were started, if the patient had no evidence of an anastomotic leakage, for example, fever, swelling, or redness of the neck. Since August 2014, we have been performing routine endoscopies to check for anastomoses before initiating the oral intakes.
The study measures included the patients' characteristics, operative times, operative blood loss volumes, the use of thoracoscopy or laparoscopy, the incidence of postoperative leakages, the incidence of pneumonia, the incidence of recurrent nerve palsy, and the lengths of the postoperative hospital stays (LOH).
Results
Table I summarizes the patients' characteristics and their operative outcomes. There were no differences between the groups with respect to age, sex, body mass index (BMI), comorbidities, cancer stage, determined using the TNM classification (7th edition), and neoadjuvant chemotherapy (NAC) administration. Each group contained three patients who had undergone esophageal bypasses with their GT reconstructions.
Using the HEMS, the blood supply to the stomach or the GT could be evaluated in all patients within 10 sec of the ICG injection. None of the patients experienced adverse events associated with the ICG injections. The ICG flow could be clearly visualized using the HEMS, and we could detect the boundary of the ANS and the anastomosis area on the GT by comparing the actual color of the GT with the one on the HEMS image. The operative time was slightly longer in the HEMS-LMM group than in the control group, that mainly related to the supraclavicular lymph node (SCLN) dissection that pasted for approximately 1 h. Eleven cases (47.8%) in the HEMS-LMM group and seven cases (25.0%) in the control group required SCLN dissections (p=0.149). There were no differences between the groups with respect to incidence of postoperative pneumonia or recurrent nerve palsy, or the median LOH. The leakage rate in the HEMS-LMM group (4.4%) was about one-quarter that in the control group (17.9%).
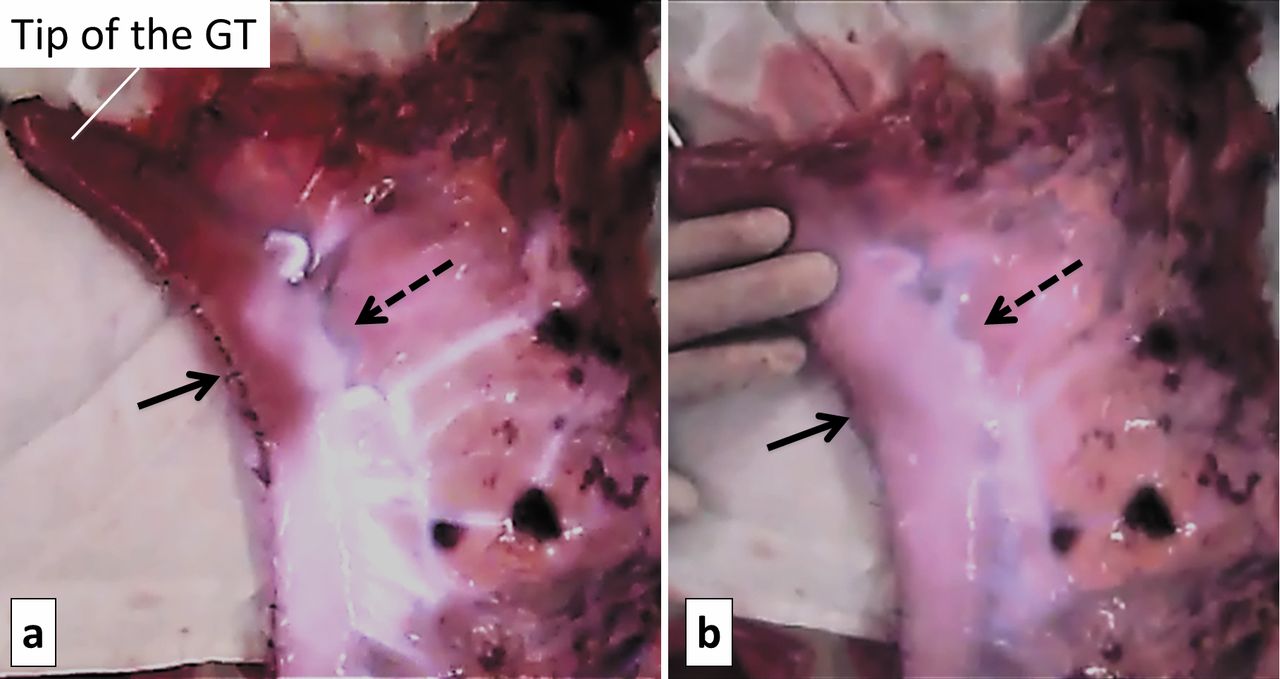
The HyperEye Medical System (HEMS)-line-marking method visualized the blood flow and the border of the blood supply from the right gastroepiploic artery on the stomach (arrows) (a). Line marking was achieved using the HEMS (b).
Summary of patients to whom the HEMS was performed in esophageal surgery with GT reconstruction.
Table II summarizes the characteristics of 6 patients who developed leakages. Five patients in the control group developed leakage. Out of these, 3 patients had cardiovascular diseases including myocardial infarctions or aortic aneurysms, and 2 had history of mediastinal radiotherapy. We reviewed their HEMS images, and confirmed areas of weak fluorescence on the GT of two of the patients who had cardiovascular diseases (Figure 3). However, the HEMS images showed good levels of fluorescence on the GT of the two patients who had been irradiated. One male patient in the HEMS-LMM group developed a late leakage. He had undergone chemoradiation therapy for cervical esophageal cancer, and he underwent salvage esophagectomy with a GT reconstruction for recurrence of cancer 7 months after the initial treatment. His short-term course after surgery was uneventful, and he was discharged from the hospital 17 days after the surgery. However, he was re-admitted to our Hospital 2 weeks after discharge because of fever and cough. An endoscopy revealed a fistula on the right oral side of the anastomosis, but the color of the GT mucosa was good. We diagnosed a late leakage caused by cervical esophageal necrosis within the area that had been irradiated.

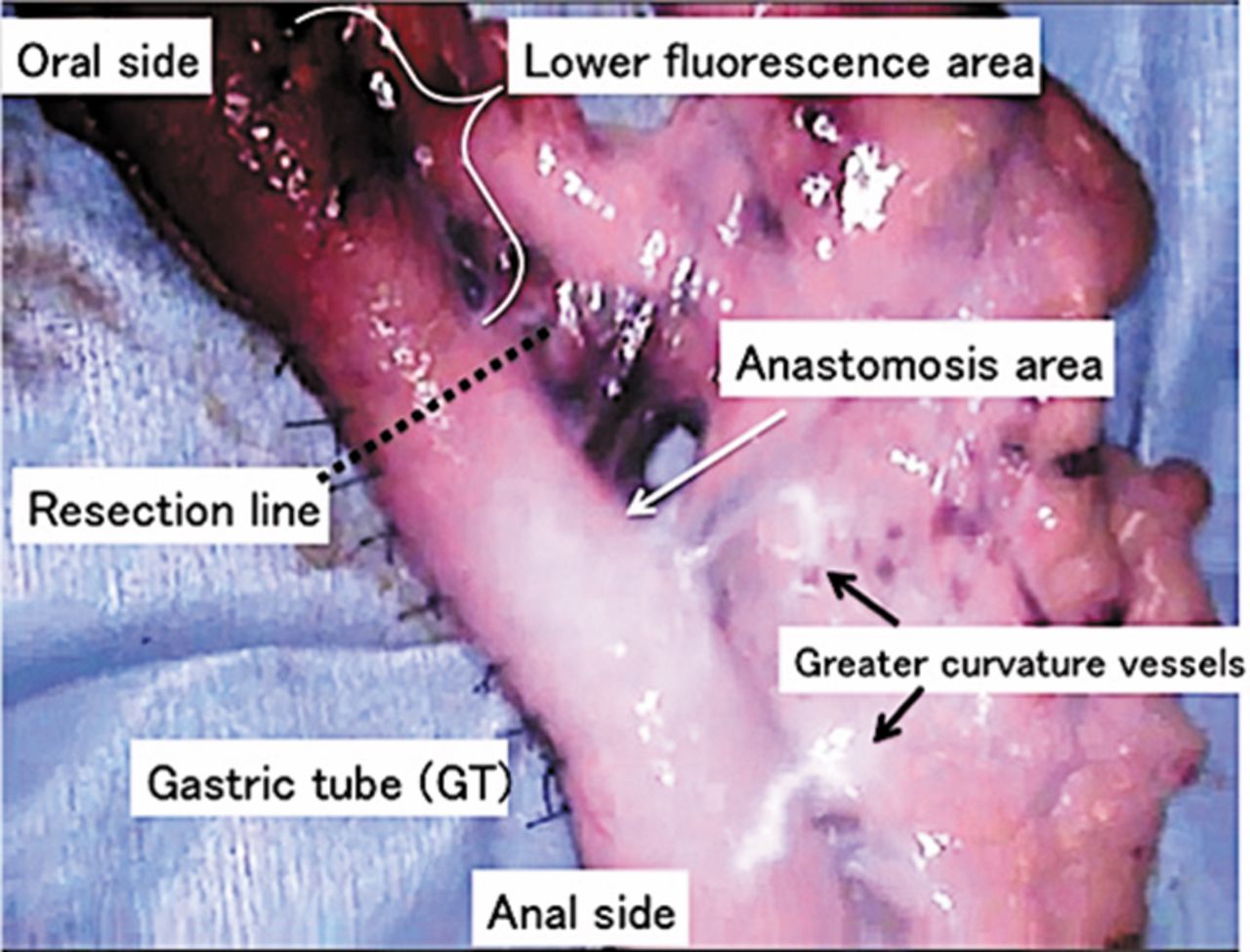
A HyperEye Medical System (HEMS) image of the gastric tube (GT) that shows late leakage at the tip. Using the HEMS, we were able to detect an area of good blood supply at the estimated anastomosis area. However, the indocyanine green fluorescence intensity at the tip of the GT was lower than that seen at the anastomosis point. After the anastomosis, we resected the tip of the GT at the high fluorescence intensity line (dotted line) using a linear stapler; however, late leakage occurred at the resection line.
Summary of patients who developed leakage.
Discussion
Although the short-term outcomes from esophagectomies for esophageal cancer have improved at our Institution with the introduction of LGM, which is a less invasive technique (8, 9), anastomotic leakage remains a problematic complication. Securing a good arterial blood supply and relieving the tension at the anastomosis site are essential. However, a method that enables for evaluation of the arterial blood supply to the anastomosis has not been established. In esophagectomies, the right GEA mainly supplies blood to the GT; however, approximately 30% of patients lack the connection between the right and left GEA (10). In these cases, the blood supply to the anastomosis depends on the ANS; however, identifying this network based on color alone is difficult. Our study suggests that the ICG fluorescence method can visualize the GEA and the ANS.
Some investigators who have not deployed the HEMS have, nevertheless, reported the usefulness of ICG fluorescence for evaluating blood supply to the anastomosis during esophagectomies (11, 12). The key advantage relating to the deployment of the HEMS is that the blood flow can be visualized on a color monitor in a well-lit operating room (13), and it enables for detection of areas of good blood supply through simultaneous comparisons with the actual surgical field. The HEMS does not require the operating room lights to be switched off, and surgery can be performed as the blood flow is evaluated. However, we experienced GT necrosis in a patient in whom the HEMS was deployed after GT creation, which led us to consider the deployment of the HEMS before GT creation to confirm the ANS border. Subsequently, we began to deploy the HEMS-LMM before GT creation. In addition, we could repeat the test using the HEMS during surgery because ICG is washed-out within 20 min of injection (5). We have also undertaken small intestinal surgery in whom the HEMS was used to evaluate the mesenteric blood flows (14).
With respect to cases that experienced leakages, the leakage in case 1 occurred at the tip of the GT, and it appeared that we had cut the tip of the GT on the line that had a lower level of fluorescence. Therefore, surgeons should pay attention to the anastomosis and to the tip of the GT. This patient resumed oral intake 7 days after surgery, because no evidence of a leakage was found, for example, fever or swelling of the neck. The early mechanical pressure applied to the tip of the GT, which had a lower fluorescence intensity, might have additionally contributed to the delayed leakage; therefore, initiation of oral intake should have been postponed. Case 5 involved partial GT necrosis. In this case, the fluorescence intensity in the area of the leakage in the GT was obviously low compared with that seen in the peripheral region. We considered that an interruption of the ANS had led to the low level of fluorescence of the GT. Therefore, surgeons should pay attention to absence of fluorescence in the estimated anastomosis area, at the tip of the GT, and on the ANS boundary. The HEMS-LMM has the advantage of confirming these areas before creating the GT.
The HEMS may be considered safe in clinical practice, because none of the patients in the HEMS group experienced adverse events associated with the ICG injection. However, precise criteria have not yet been established for the HEMS in relation to postponement of oral intake or where the anastomosis of the vessels should be performed. A history of cardiovascular disease might be associated with a risk of leakage (15), and our data suggest that a lower fluorescence intensity in the HEMS images is indicative of a risk of delayed leakage. When the HEMS images show low levels of fluorescence, early necrosis may occur. Furthermore, even when the HEMS images show good levels of fluorescence on the GT, a history of mediastinal radiation therapy might be associated with a risk of leakage after esophageal surgery (16).
The usefulness of early endoscopic assessments following esophagectomies has been previously reported (17). Early endoscopic assessments may contribute to establishment of criteria for the HEMS by comparing the ICG fluorescence with the endoscopic images of the anastomosis. In addition, the HEMS can be used to predict which reconstruction method is the most suitable following esophageal surgery, including the estimated anastomosis and the GT resection line. This is an issue that should be investigated in the future.
The present study was limited by its retrospective nature, involving a small number of patients. Further investigations need to be undertaken in order for the usefulness of the HEMS-LMM for preventing leakages after esophageal surgery to be determined.
The HEMS-LMM is safe and feasible for visualizing the blood supply border associated with the right GEA and the ANS before GT creation during esophageal surgery. It might reduce leakage, but further investigations are required to establish criteria that determine when the HEMS should be deployed to ensure there are no leakages.
Acknowledgements
The Authors thank the clinical engineer Kazunori Aki from Kochi University for providing the technical support for the HEMS.
Footnotes
Financial Support
None.
Conflicts of Interest
None.
- Received July 16, 2015.
- Revision received August 27, 2015.
- Accepted August 31, 2015.
- Copyright© 2015 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved
References
In this issue





{kind=link}
{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- Near-infrared nerve-binding fluorophores for buried nerve tissue imaging
- Innovations for Cervical Esophagogastrostomy in Thoracic Esophageal Cancer Operations
- Gastric Tube Reconstruction with Superdrainage Using Indocyanine Green Fluorescence During Esophagectomy
- Analysis of Factors Associated with Weight Loss After Esophagectomy for Esophageal Cancer