Three and Five-Year Mortality in Ovarian Cancer after Minimally Invasive Compared to Open Surgery: A Systematic Review and Meta-Analysis

 , ,
, ,
Abstract
:1. Introduction
2. Experimental Section
3. Results
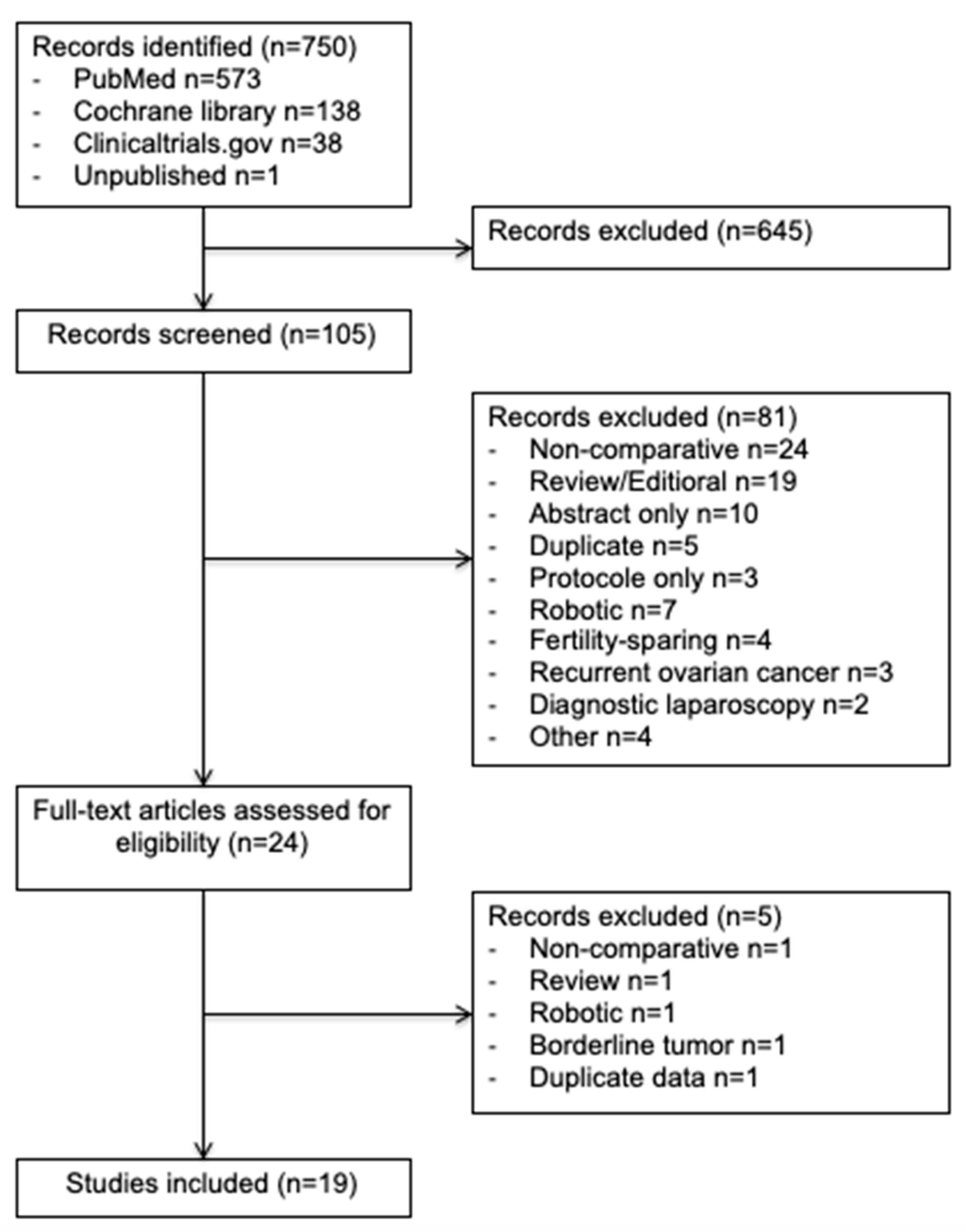
3.1. Literature Search
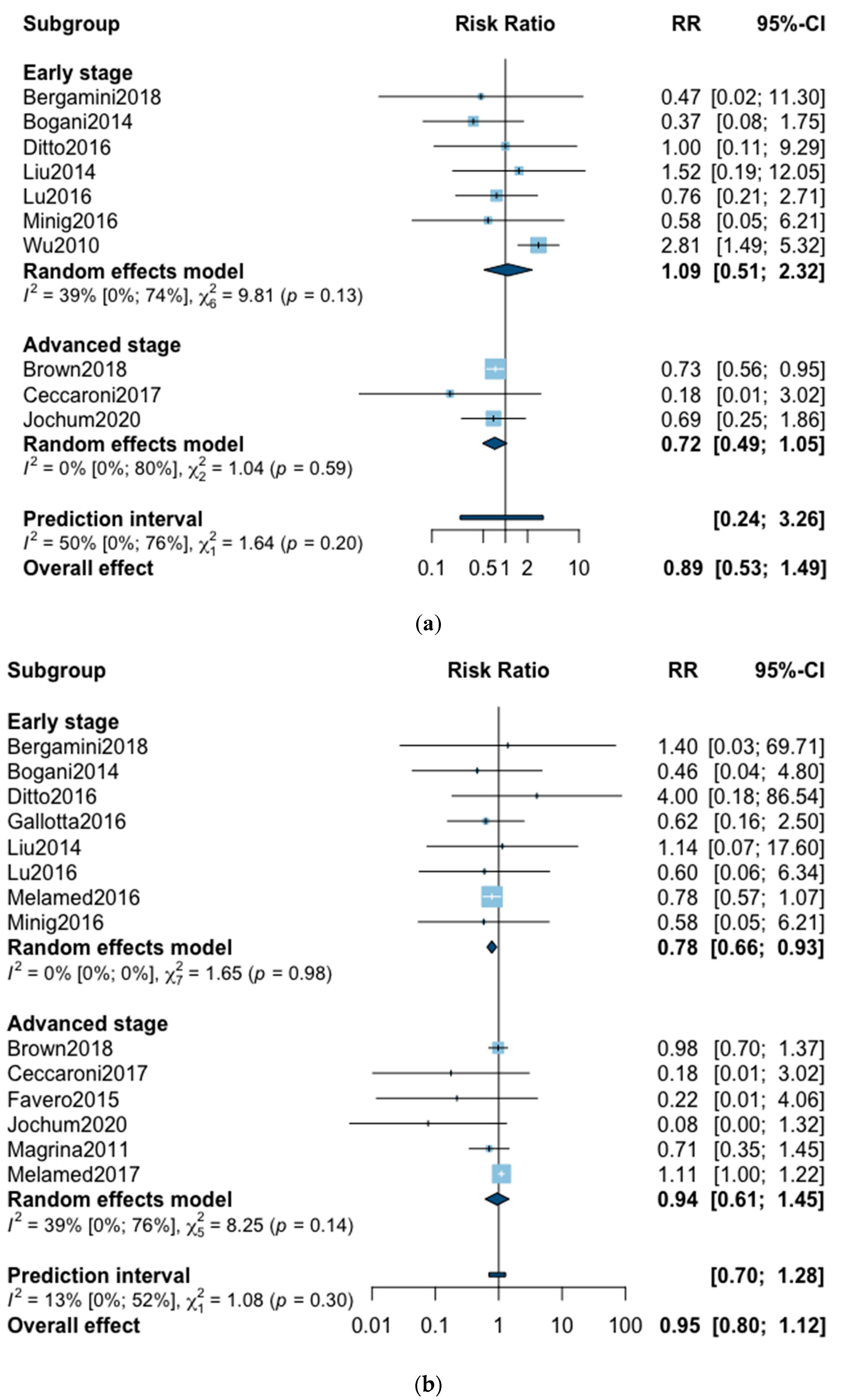
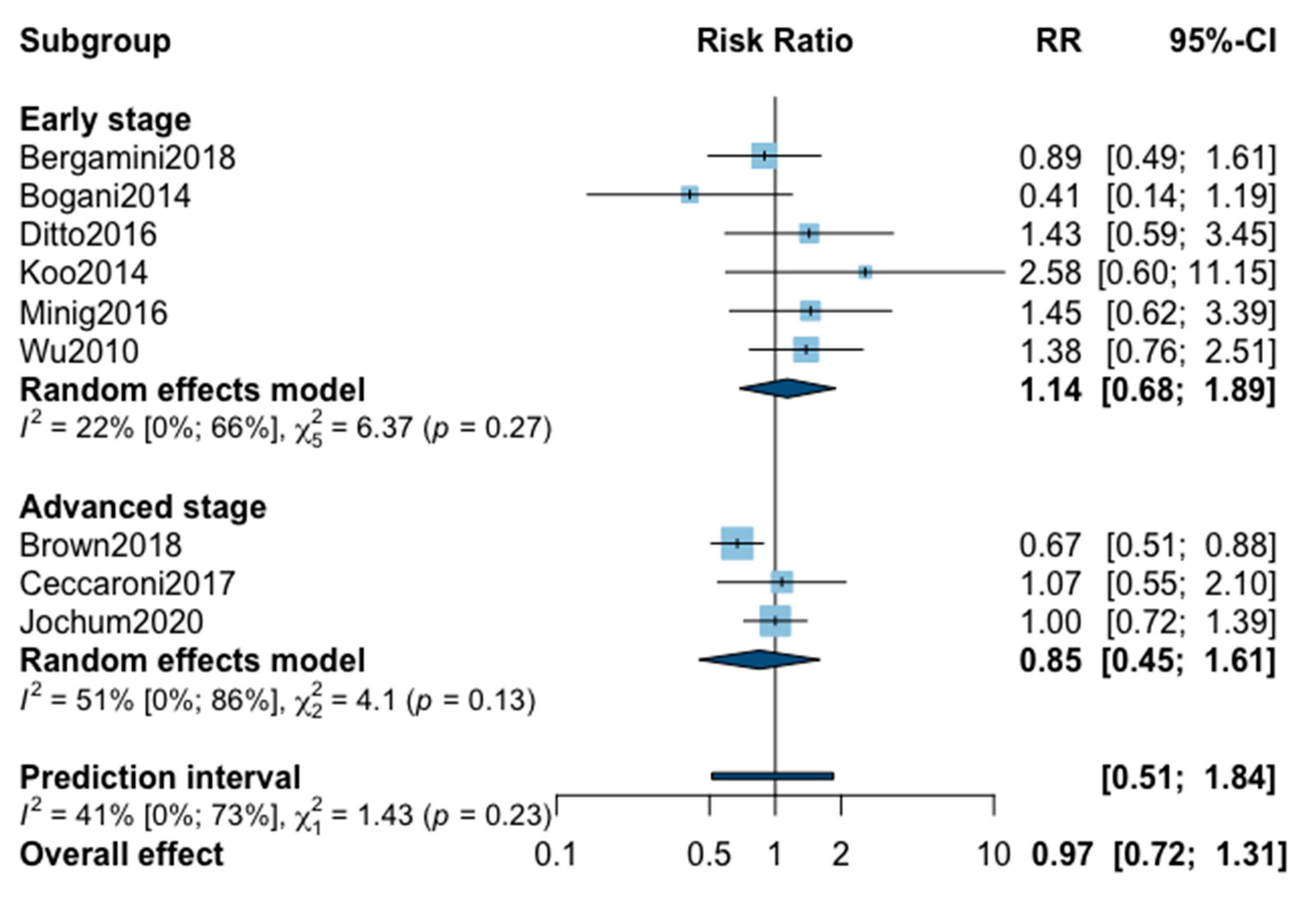
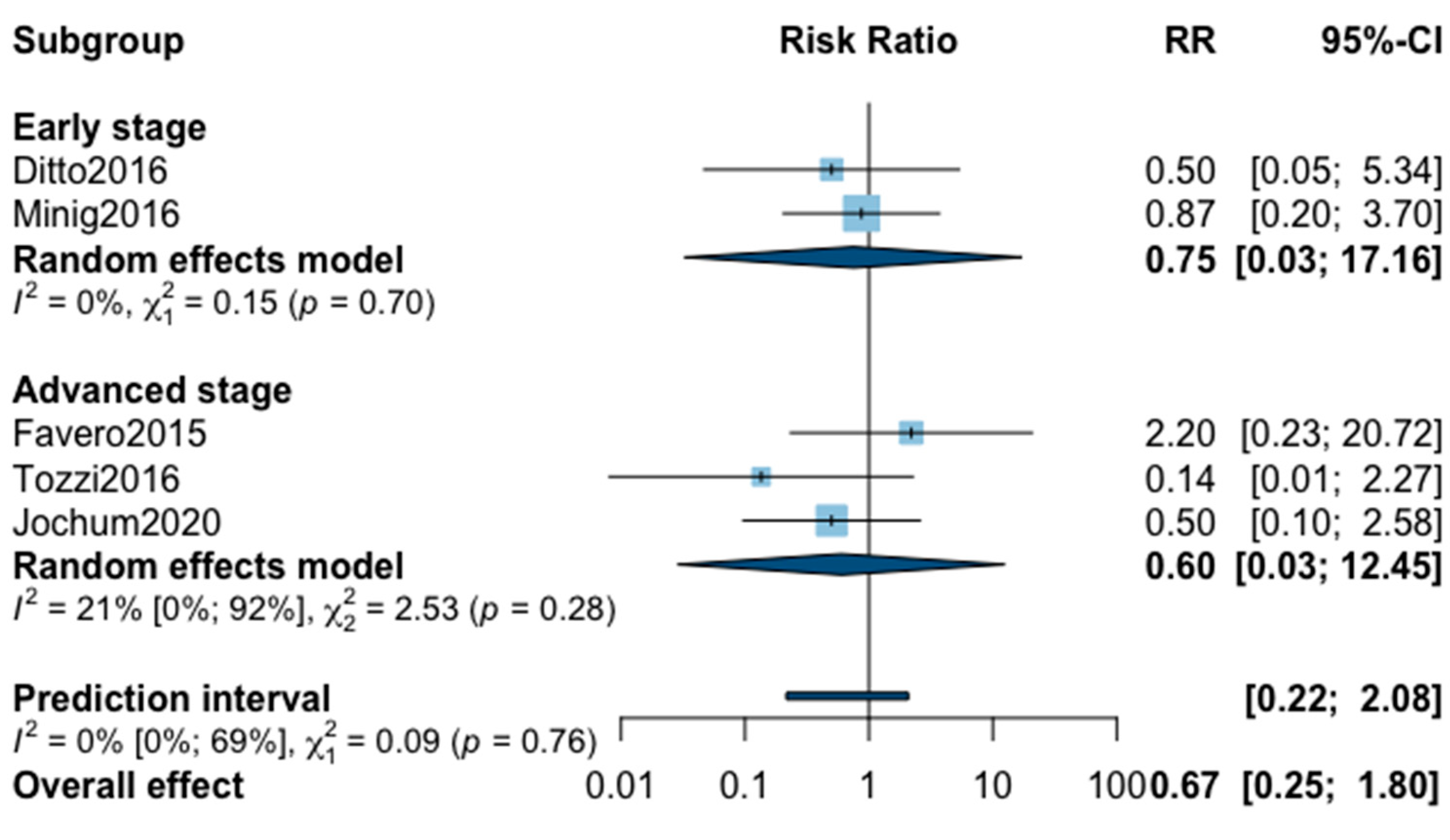
3.2. Overall Mortality
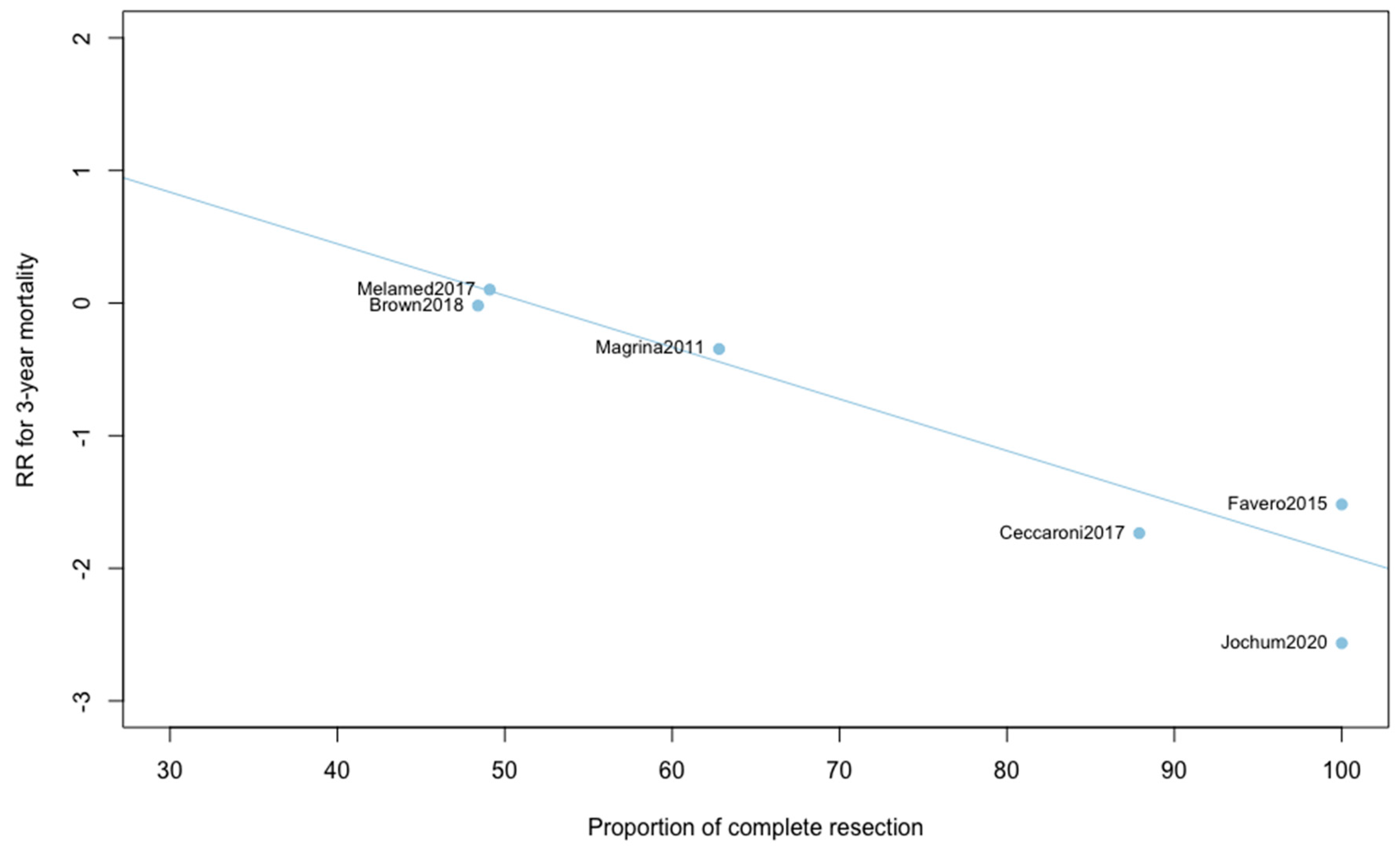
3.3. Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
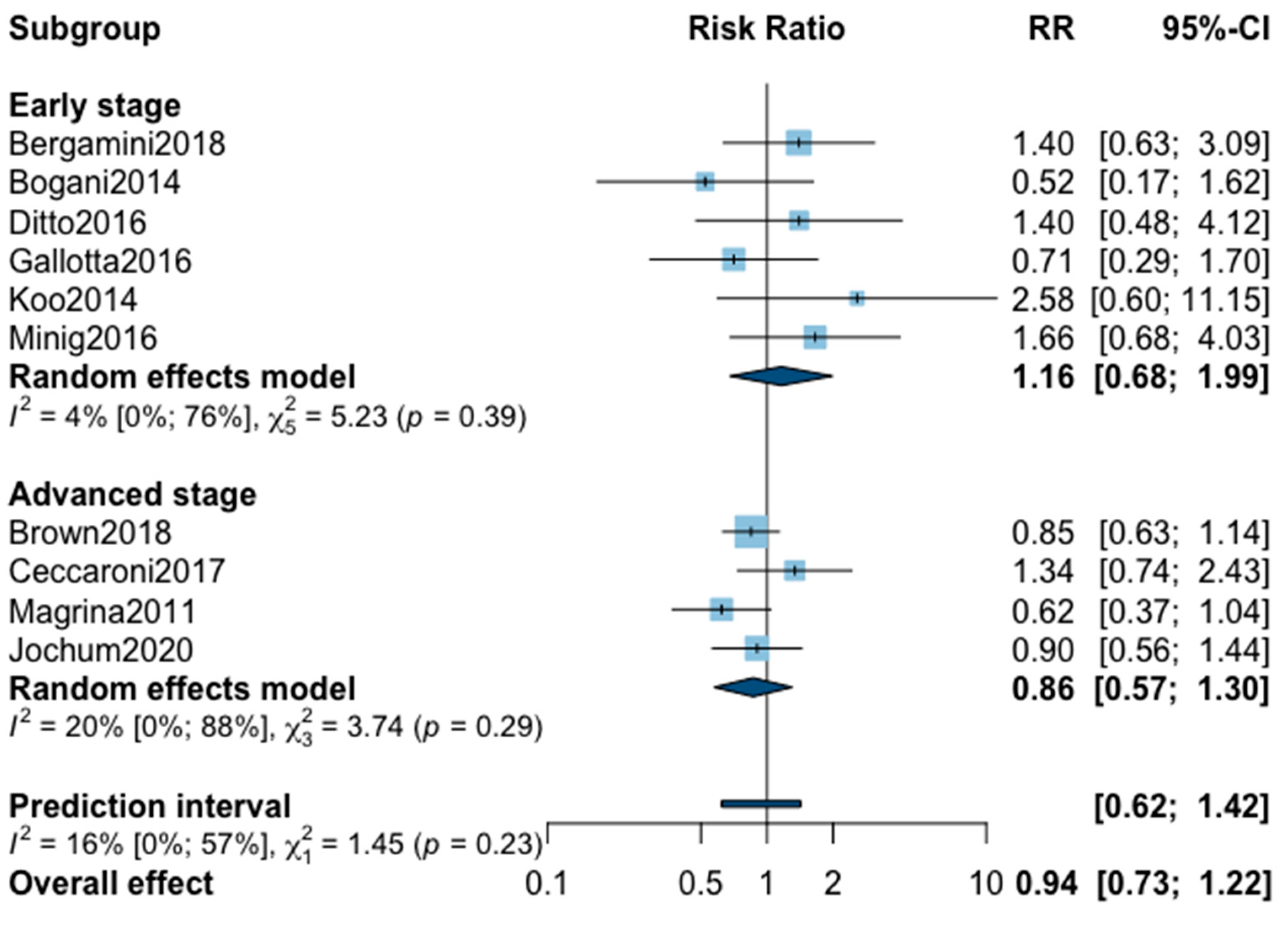
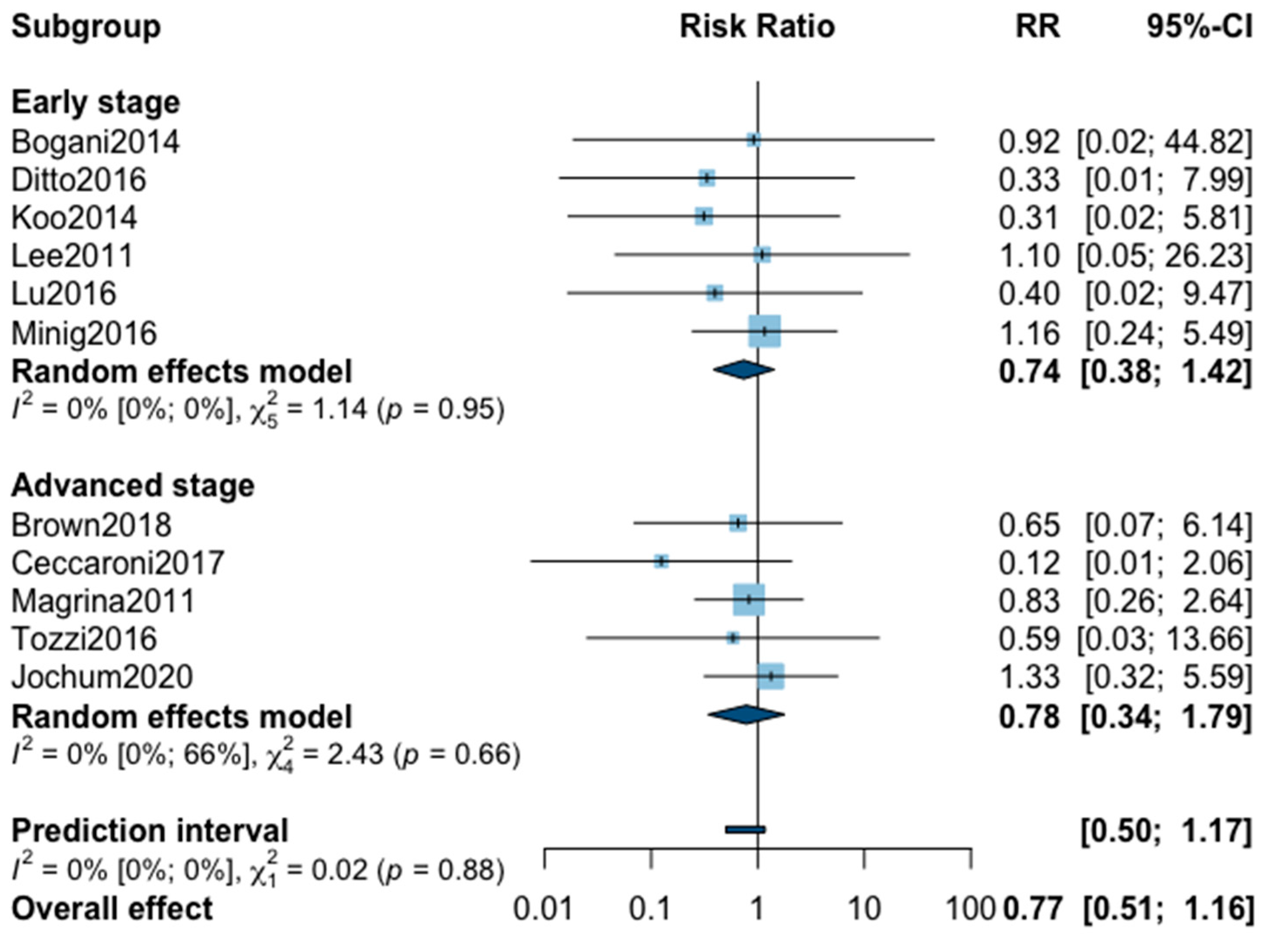
Appendix A. Meta-Analysis for Recurrence


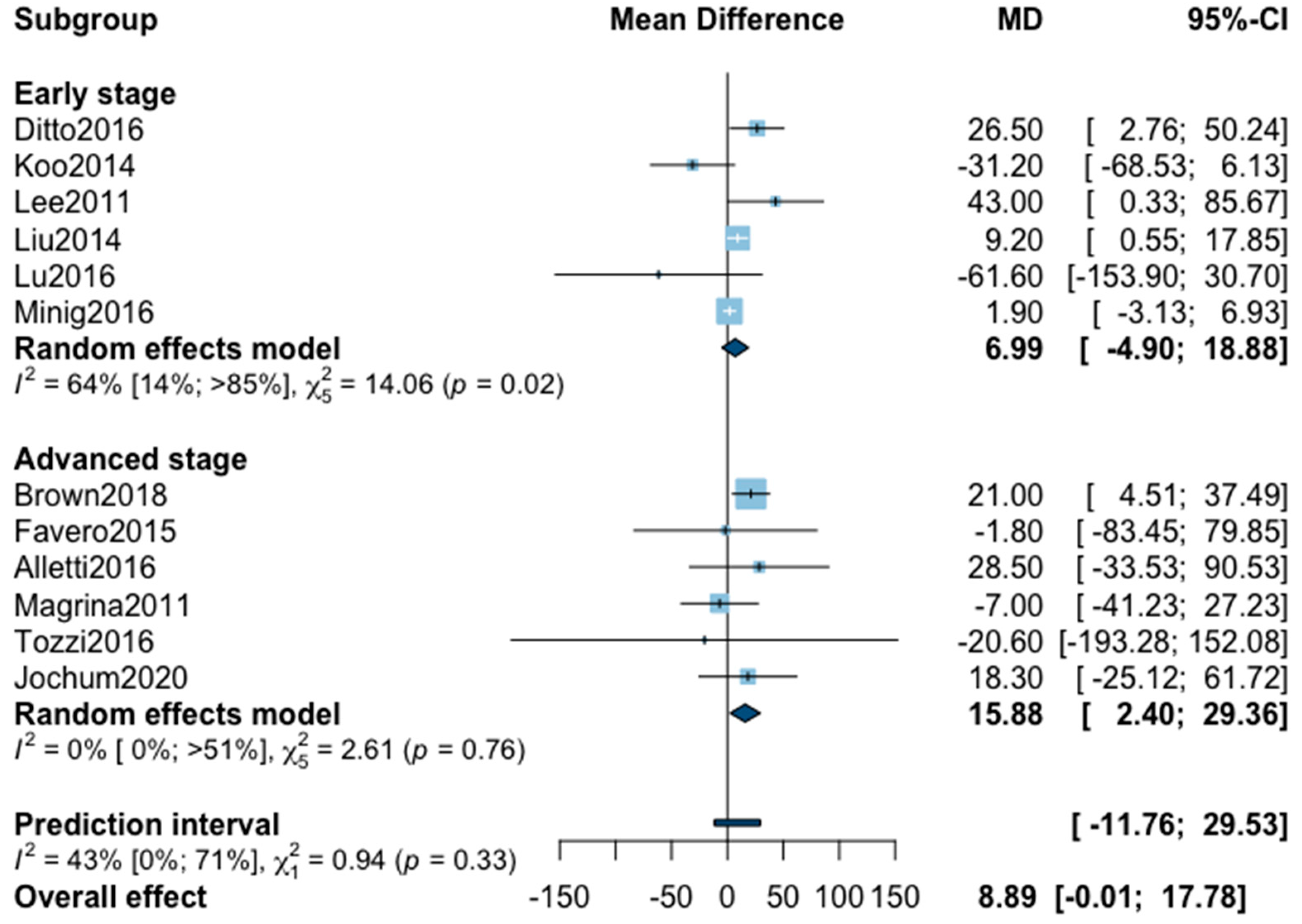
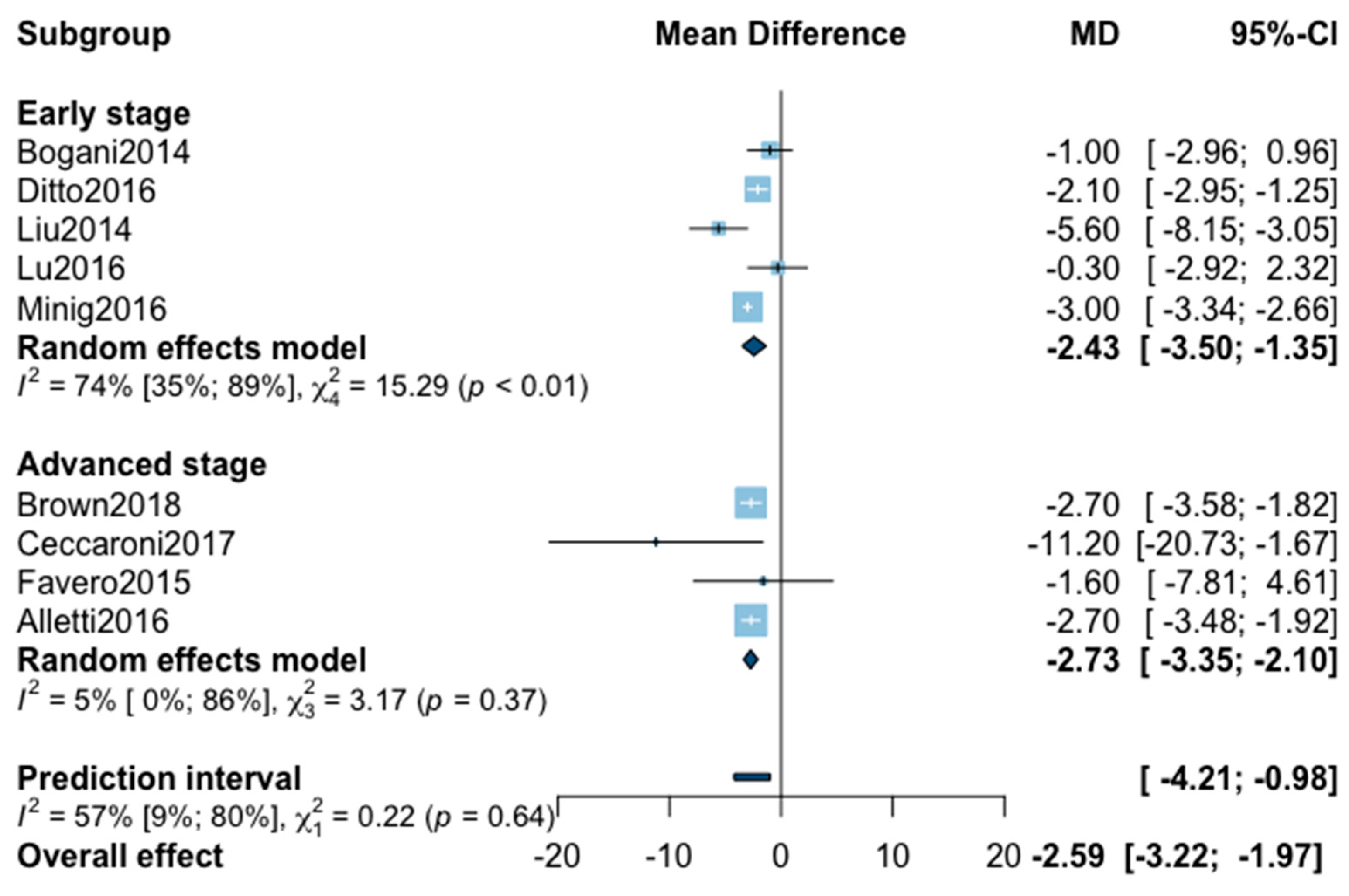
Appendix B. Meta-Analysis for Perioperative Outcomes






Appendix C

References
- Ferlay, J.; Soerjomataram, I.; Dikshit, R.; Eser, S.; Mathers, C.; Rebelo, M.; Parkin, D.M.; Forman, D.; Bray, F. Cancer incidence and mortality worldwide: Sources, methods and major patterns in GLOBOCAN 2012. Int. J. Cancer 2015, 136, E359–E386. [Google Scholar] [CrossRef] [PubMed]
- Colombo, N.; Sessa, C.; du Bois, A.; Ledermann, J.; McCluggage, W.G.; McNeish, I.; Morice, P.; Pignata, S.; Ray-Coquard, I.; Vergote, I.; et al. ESMO-ESGO consensus conference recommendations on ovarian cancer: Pathology and molecular biology, early and advanced stages, borderline tumours and recurrent disease. Ann. Oncol. 2019, 30, 672–705. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Menderes, G.; Black, J.; Azodi, M. The role of minimally invasive interval debulking surgery in advanced epithelial ovarian cancer. Expert Rev. Anticancer. Ther. 2016, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fagotti, A.; Perelli, F.; Pedone, L.; Scambia, G. Current Recommendations for Minimally Invasive Surgical Staging in Ovarian Cancer. Curr. Treat. Options Oncol. 2016, 17, 3. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-Y.; Kim, D.-Y.; Kim, J.-H.; Kim, Y.-M.; Kim, Y.-T.; Nam, J.-H. Laparoscopic Versus Laparotomic Surgical Staging for Early Stage Epithelial Ovarian Cancer. J. Minim. Invasive Gynecol. 2011, 18, S59. [Google Scholar] [CrossRef]
- Lu, Q.; Qu, H.; Liu, C.; Wang, S.; Zhang, Z.; Zhang, Z. Comparison of Laparoscopy and Laparotomy in Surgical Staging of Apparent Early Ovarian Cancer: 13-year Experience. Med. Baltim. 2016, 95, e3655. [Google Scholar] [CrossRef]
- Shi, C.; Gao, Y.; Yang, Y.; Zhang, L.; Yu, J.; Zhang, T. Comparison of efficacy of robotic surgery, laparoscopy, and laparotomy in the treatment of ovarian cancer: A meta-analysis. World J. Surg. Oncol. 2019, 17, 162. [Google Scholar] [CrossRef]
- Falcetta, F.S.; Lawrie, T.A.; Medeiros, L.R.; da Rosa, M.I.; Edelweiss, M.I.; Stein, A.T.; Zelmanowicz, A.; Moraes, A.B.; Zanini, R.R.; Rosa, D.D. Laparoscopy versus laparotomy for FIGO stage I ovarian cancer. Cochrane Database Syst. Rev. 2016, 10, CD005344. [Google Scholar] [CrossRef]
- Zhang, Y.; Fan, S.; Xiang, Y.; Duan, H.; Sun, L. Comparison of the prognosis and recurrence of apparent early-stage ovarian tumors treated with laparoscopy and laparotomy: A meta-analysis of clinical studies. BMC Cancer 2015, 15, 597. [Google Scholar] [CrossRef] [Green Version]
- Cardenas-Goicoechea, J.; Wang, Y.; McGorray, S.; Saleem, M.D.; Carbajal Mamani, S.L.; Pomputius, A.F.; Markham, M.-J.; Castagno, J.C. Minimally invasive interval cytoreductive surgery in ovarian cancer: Systematic review and meta-analysis. J. Robot. Surg. 2019, 13, 23–33. [Google Scholar] [CrossRef]
- Bogani, G.; Cromi, A.; Serati, M.; Di Naro, E.; Casarin, J.; Pinelli, C.; Ghezzi, F. Laparoscopic and open abdominal staging for early-stage ovarian cancer: Our experience, systematic review, and meta-analysis of comparative studies. Int. J. Gynecol. Cancer 2014, 24, 1241–1249. [Google Scholar] [CrossRef] [PubMed]
- Bogani, G.; Borghi, C.; Maggiore, U.L.R.; Ditto, A.; Signorelli, M.; Martinelli, F.; Chiappa, V.; Lopez, C.; Sabatucci, I.; Scaffa, C.; et al. Minimally Invasive Surgical Staging in Early-stage Ovarian Carcinoma: A Systematic Review and Meta-analysis. J. Minim. Invasive Gynecol. 2017, 24, 552–562. [Google Scholar] [CrossRef] [PubMed]
- Stroup, D.F.; Berlin, J.A.; Morton, S.C.; Olkin, I.; Williamson, G.D.; Rennie, D.; Moher, D.; Becker, B.J.; Sipe, T.A.; Thacker, S.B. Meta-analysis of observational studies in epidemiology: A proposal for reporting. Meta-analysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000, 283, 2008–2012. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, T.P. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLOS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Dindo, D.; Demartines, N.; Clavien, P.-A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Borenstein, M.; Higgins, J.P.T. Meta-analysis and subgroups. Prev. Sci. 2013, 14, 134–143. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions, version 6.0; Cochrane: London, UK, 2019. [Google Scholar]
- Egger, M.; Davey Smith, G.; Schneider, M.; Minder, C. Bias in meta-analysis detected by a simple, graphical test. BMJ 1997, 315, 629–634. [Google Scholar] [CrossRef] [Green Version]
- Brown, J.; Drury, L.; Crane, E.K.; Anderson, W.E.; Tait, D.L.; Higgins, R.V.; Naumann, R.W. When Less Is More: Minimally Invasive Surgery Compared with Laparotomy for Interval Debulking After Neoadjuvant Chemotherapy in Women with Advanced Ovarian Cancer. J. Minim. Invasive Gynecol. 2019, 26, 902–909. [Google Scholar] [CrossRef]
- Ceccaroni, M.; Roviglione, G.; Bruni, F.; Clarizia, R.; Ruffo, G.; Salgarello, M.; Peiretti, M.; Uccella, S. Laparoscopy for primary cytoreduction with multivisceral resections in advanced ovarian cancer: Prospective validation. “The times they are a-changin”? Surg. Endosc. 2018, 32, 2026–2037. [Google Scholar] [CrossRef] [PubMed]
- Ditto, A.; Bogani, G.; Martinelli, F.; Signorelli, M.; Chiappa, V.; Scaffa, C.; Indini, A.; Leone Roberti Maggiore, U.; Lorusso, D.; Raspagliesi, F. Minimally Invasive Surgical Staging for Ovarian Carcinoma: A Propensity-Matched Comparison With Traditional Open Surgery. J. Minim. Invasive Gynecol. 2017, 24, 98–102. [Google Scholar] [CrossRef] [PubMed]
- Favero, G.; Macerox, N.; Pfiffer, T.; Köhler, C.; da Costa Miranda, V.; Estevez Diz, M.D.P.; Fukushima, J.T.; Baracat, E.C.; Carvalho, J.P. Oncologic Concerns regarding Laparoscopic Cytoreductive Surgery in Patients with Advanced Ovarian Cancer Submitted to Neoadjuvant Chemotherapy. Oncology 2015, 89, 159–166. [Google Scholar] [CrossRef] [PubMed]
- Gallotta, V.; Petrillo, M.; Conte, C.; Vizzielli, G.; Fagotti, A.; Ferrandina, G.; Fanfani, F.; Costantini, B.; Carbone, V.; Scambia, G. Laparoscopic Versus Laparotomic Surgical Staging for Early-Stage Ovarian Cancer: A Case-Control Study. J. Minim. Invasive Gynecol. 2016, 23, 769–774. [Google Scholar] [CrossRef]
- Gueli Alletti, S.; Petrillo, M.; Vizzielli, G.; Bottoni, C.; Nardelli, F.; Costantini, B.; Quagliozzi, L.; Gallotta, V.; Scambia, G.; Fagotti, A. Minimally invasive versus standard laparotomic interval debulking surgery in ovarian neoplasm: A single-institution retrospective case-control study. Gynecol. Oncol. 2016, 143, 516–520. [Google Scholar] [CrossRef]
- Koo, Y.-J.; Kim, J.-E.; Kim, Y.-H.; Hahn, H.-S.; Lee, I.-H.; Kim, T.-J.; Lee, K.-H.; Shim, J.-U.; Lim, K.-T. Comparison of laparoscopy and laparotomy for the management of early-stage ovarian cancer: Surgical and oncological outcomes. J. Gynecol. Oncol. 2014, 25, 111–117. [Google Scholar] [CrossRef] [Green Version]
- Lee, M.; Kim, S.W.; Paek, J.; Lee, S.H.; Yim, G.W.; Kim, J.H.; Kim, J.W.; Kim, Y.T.; Nam, E.J. Comparisons of Surgical Outcomes, Complications, and Costs Between Laparotomy and Laparoscopy in Early-Stage Ovarian Cancer. Int. J. Gynecol. Cancer 2011, 21. [Google Scholar] [CrossRef]
- Liu, M.; Li, L.; He, Y.; Peng, D.; Wang, X.; Chen, W.; Fu, X.; Ma, Y. Comparison of laparoscopy and laparotomy in the surgical management of early-stage ovarian cancer. Int. J. Gynecol. Cancer 2014, 24, 352–357. [Google Scholar] [CrossRef]
- Magrina, J.F.; Zanagnolo, V.; Noble, B.N.; Kho, R.M.; Magtibay, P. Robotic approach for ovarian cancer: Perioperative and survival results and comparison with laparoscopy and laparotomy. Gynecol. Oncol. 2011, 121, 100–105. [Google Scholar] [CrossRef]
- Melamed, A.; Keating, N.L.; Clemmer, J.T.; Bregar, A.J.; Wright, J.D.; Boruta, D.M.; Schorge, J.O.; Del Carmen, M.G.; Rauh-Hain, J.A. Laparoscopic Staging for Apparent Stage I Epithelial Ovarian Cancer: Analysis of the National Cancer Data Base. Am. J. Obstet. Gynecol. 2017, 216, 50.e1–50.e12. [Google Scholar] [CrossRef] [Green Version]
- Melamed, A.; Nitecki, R.; Boruta, D.M.; Del Carmen, M.G.; Clark, R.M.; Growdon, W.B.; Goodman, A.; Schorge, J.O.; Rauh-Hain, J.A. Laparoscopy Compared With Laparotomy for Debulking Ovarian Cancer After Neoadjuvant Chemotherapy. Obstet. Gynecol. 2017, 129, 861–869. [Google Scholar] [CrossRef] [PubMed]
- Minig, L.; Saadi, J.; Patrono, M.G.; Giavedoni, M.E.; Cárdenas-Rebollo, J.M.; Perrotta, M. Laparoscopic surgical staging in women with early stage epithelial ovarian cancer performed by recently certified gynecologic oncologists. Eur. J. Obstet. Gynecol. Reprod. Biol. 2016, 201, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Tozzi, R.; Gubbala, K.; Majd, H.S.; Campanile, R.G. Interval Laparoscopic En-Bloc Resection of the Pelvis (L-EnBRP) in patients with stage IIIC-IV ovarian cancer: Description of the technique and surgical outcomes. Gynecol. Oncol. 2016, 142, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Bergamini, A.; Ferrandina, G.; Candiani, M.; Cormio, G.; Giorda, G.; Lauria, R.; Perrone, A.M.; Scarfone, G.; Breda, E.; Savarese, A.; et al. Laparoscopic surgery in the treatment of stage I adult granulosa cells tumors of the ovary: Results from the MITO-9 study. Eur. J. Surg. Oncol. 2018, 44, 766–770. [Google Scholar] [CrossRef] [PubMed]
- Wu, T.-I.; Lee, C.-L.; Liao, P.-J.; Huang, K.-G.; Chang, T.-C.; Chou, H.-H.; Wang, C.-J.; Soong, Y.-K.; Hsueh, S.; Lai, C.-H. Survival impact of initial surgical approach in stage I ovarian cancer. Chang. Gung. Med. J. 2010, 33, 558–567. [Google Scholar]
- Jochum, F.; Aubry, G.; Pellerin, M.; Billard, C.; Faller, E.; Boisrame, T.; Lecointre, L.; Akladios, C. Relevance of minimally invasive surgery for epithelial ovarian cancer in well-selected patients: A propensity-matched comparison with traditional open surgery. 2020; in press. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Period | Study Design | Total MINORS * | Location | Histological Type | Number of Patients | Follow-Up, Months | Adjuvant Therapy, n (%) | Neoadjuvant Therapy, n (%) | Complete Resection, n (%) |
|---|---|---|---|---|---|---|---|---|---|---|
| Early ovarian cancer | ||||||||||
| Bergamini et al., 2018 | 1965–2017 | Retrospective | 18 | Multicenter Italy | Granulosa cells | MIS = 93 | 81 (10–450) | 25 (11%) | - | - |
| OS = 130 | ||||||||||
| Bogani et al., 2014 | 2003–2010 | Retrospective | 18 | Monocentric Italy | Epithelial | MIS = 35 | 64 (37–106) | 56 (84%) | - | - |
| OS = 32 | 100 (61–287) | |||||||||
| Ditto et al., 2016 | 2005–2015 | Retrospective and prospective | 19 | Monocentric Italy | Epithelial | MIS = 50 | 49.5 (64) | 59 (59%) | - | - |
| OS = 50 | 52.6 (31.7) | |||||||||
| Gallotta et al., 2016 | 2000–2013 | Retrospective | 17 | Monocentric Italy | Epithelial | MIS = 60 | 38 (24–48) | 126 (70%) | - | - |
| OS = 120 | ||||||||||
| Koo et al., 2014 | 2006–2012 | Retrospective | 18 | Multicenter Korea | All types | MIS = 24 | 31.7 (20.7) | 69 (90%) | - | - |
| OS = 53 | 31.1 (19.1) | |||||||||
| Lee et al., 2011 | 2005–2010 | Retrospective | 18 | Monocentric Korea | All types | MIS = 26 | 12 (1–42) | 82 (73%) | - | - |
| OS = 87 | 25 (1–74) | |||||||||
| Liu et al., 2014 | 2002–2012 | Retrospective | 16 | Monocentric China | All types | MIS = 35 | 36 to 84 | 66 (88%) | - | - |
| OS = 40 | ||||||||||
| Lu et al., 2016 | 2002–2014 | Retrospective | 19 | Monocentric China | Epithelial | MIS = 42 | 82 (16–152) | - | - | - |
| OS = 50 | 82 (16–152) | |||||||||
| Melamed et al., 2016 | 2010–2012 | Retrospective | 20 | Multicenter USA | Epithelial | MIS = 1096 | 28.7 (20.4–38.9) | 1230 (56%) | - | - |
| OS = 1096 | 29.3 (20.6–39.3) | |||||||||
| Minig et al., 2016 | 2006–2014 | Retrospective | 17 | Multicenter Spain and Argentina | Epithelial | MIS = 50 | 25.9 (11.2–38.5) | 66 (61%) | - | - |
| OS = 58 | 34.3 (32.8–49) | |||||||||
| Wu et al., 2009 | 1984–2006 | Retrospective | 18 | Multicenter Taiwan | Epithelial | MIS = 34 | 48.5 (3–174.5) | 152 (78%) | - | - |
| OS = 174 | 67 (2–276) | |||||||||
| Advanced ovarian cancer | ||||||||||
| Alletti et al., 2016 | 2010–2014 | Retrospective | 17 | Monocentric Italy | High grade serous | MIS = 30 | 28 | 95 (100%) | 95 (100%) | 91 (96%) |
| OS = 65 | ||||||||||
| Brown et al., 2018 | 2006–2017 | Retrospective | 19 | Monocentric USA | Epithelial | MIS = 53 | - | - | 157 (100%) | 76 (48%) |
| OS = 104 | ||||||||||
| Ceccaroni et al., 2017 | 2007–2015 | Prospective | 19 | Monocentric Italy | All types | MIS = 21 | 47.3 (12–72) | 66 (100%) | 0 | 58 (88%) |
| OS = 45 | 52.3 (5–117) | |||||||||
| Favero et al., 2015 | 2011–2014 | Prospective | 20 | Monocentric Brazil | High grade serous | MIS = 10 | 20 (12–26) | 21 (100%) | 21 (100%) | 21 (100%) |
| OS = 11 | 36 (24–48) | |||||||||
| Jochum et al., 2020 | 2010–2018 | Retrospective | 19 | Monocentric France | Epithelial | MIS = 41 | 31.0 (16.0–52.0) | 67 (82%) | 45 (55%) | 82 (100%) |
| OS = 41 | 32.0 (23.0–61.0) | |||||||||
| Magrina et al., 2011 | 2002–2008 | Retrospective | 17 | Monocentric USA | Epithelial | MIS = 27 | 52.8 (2.4–110.4) | 106 (73%) | 36 (25%) | 92 (63%) |
| OS = 119 | 34.8 (0–128.4) | |||||||||
| Melamed et al., 2017 | 2010–2012 | Retrospective | 19 | Multicenter USA | Epithelial | MIS = 540 | 32.0 | - | 3161 (100%) | 919 (49%) |
| OS = 2621 | ||||||||||
| Tozzi et al., 2016 | 2008–2016 | Prospective | 19 | Multicenter Italy and United Kingdom | All type | MIS = 18 | - | - | 50 (100%) | 49 (98%) |
| OS = 32 | - | |||||||||
| Metaregression | k | Exponentiated Slope Coefficient (95% CI) | p Value |
|---|---|---|---|
| Five-year mortality | |||
| Metaregression by adjuvant therapy, % | |||
| Early stage | 6 | 0.01 (−0.04 to 0.07) | 0.55 |
| Overall | 8 | −0.00 (−0.05 to 0.05) | 0.99 |
| Metaregression by neoadjuvant therapy, % | |||
| Advanced stage | 3 | 0.01 (−0.08 to 0.09) | 0.51 |
| Metaregression by complete resection, % | |||
| Advanced stage | 3 | −0.00 (−0.12 to 0.11) | 0.77 |
| Three-year mortality | |||
| Metaregression by adjuvant therapy, % | |||
| Early stage | 7 | −0.01 (−0.04 to 0.02) | 0.53 |
| Advanced stage | 4 | −0.05 (−0.20 to 0.09) | 0.24 |
| Overall | 11 | −0.02 (−0.04 to 0.00) | 0.06 |
| Metaregression by neoadjuvant therapy, % | |||
| Advanced stage | 5 | 0.01 (−0.01 to 0.02) | 0.21 |
| Metaregression by complete resection, % | |||
| Advanced stage | 6 | −0.04 (−0.06 to −0.02) | 0.01 |
| Five-year recurrence | |||
| Metaregression by adjuvant therapy, % | |||
| Early stage | 6 | 0.00 (−0.02 to 0.03) | 0.69 |
| Overall | 8 | 0.00 (−0.01 to 0.01) | 0.78 |
| Metaregression by neoadjuvant therapy, % | |||
| Advanced stage | 3 | −0.01 (−0.04 to 0.03) | 0.25 |
| Meta-regression by complete resection, % | |||
| Advanced stage | 3 | 0.01 (−0.02 to 0.03) | 0.14 |
| Three-year recurrence | |||
| Metaregression by adjuvant therapy, % | |||
| Early stage | 6 | −0.01 (−0.03 to 0.02) | 0.58 |
| Advanced stage | 3 | 0.03 (−0.04 to 0.10) | 0.12 |
| Overall | 9 | −0.00 (−0.02 to 0.01) | 0.66 |
| Metaregression by neoadjuvant therapy, % | |||
| Advanced stage | 4 | −0.00 (−0.02 to 0.02) | 0.73 |
| Metaregression by complete resection, % | |||
| Advanced stage | 4 | 0.01 (−0.03 to 0.04) | 0.55 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jochum, F.; Vermel, M.; Faller, E.; Boisrame, T.; Lecointre, L.; Akladios, C. Three and Five-Year Mortality in Ovarian Cancer after Minimally Invasive Compared to Open Surgery: A Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 2507. https://doi.org/10.3390/jcm9082507
Jochum F, Vermel M, Faller E, Boisrame T, Lecointre L, Akladios C. Three and Five-Year Mortality in Ovarian Cancer after Minimally Invasive Compared to Open Surgery: A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2020; 9(8):2507. https://doi.org/10.3390/jcm9082507
Chicago/Turabian StyleJochum, Floriane, Muriel Vermel, Emilie Faller, Thomas Boisrame, Lise Lecointre, and Cherif Akladios. 2020. "Three and Five-Year Mortality in Ovarian Cancer after Minimally Invasive Compared to Open Surgery: A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 9, no. 8: 2507. https://doi.org/10.3390/jcm9082507