Reduced and Normalized Carbohydrate Antigen 19-9 Concentrations after Neoadjuvant Chemotherapy Have Comparable Prognostic Performance in Patients with Borderline Resectable and Locally Advanced Pancreatic Cancer

 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Patients and Study Design
2.2. Statistical Analyses
3. Results
3.1. Patient Characteristics
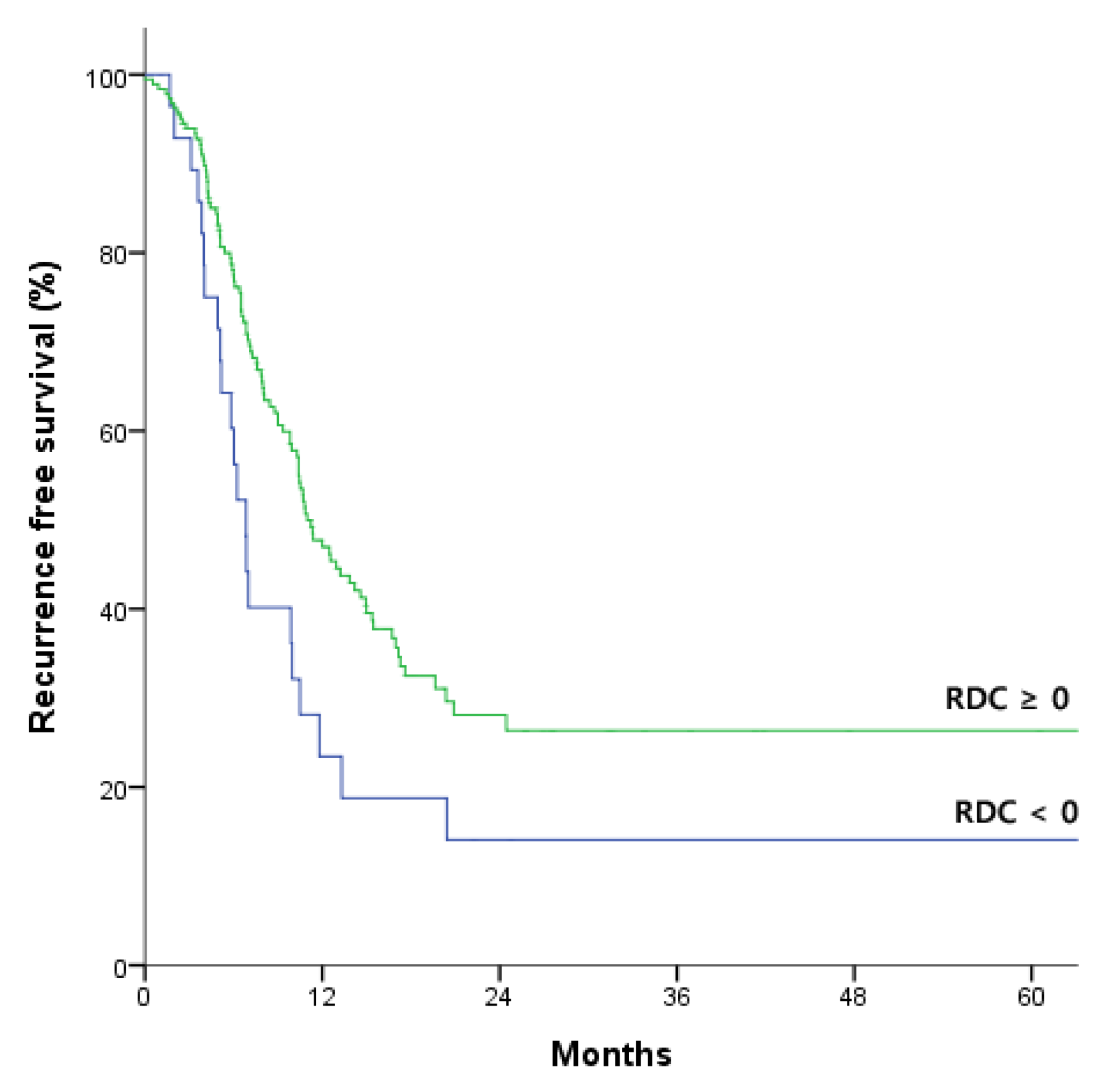
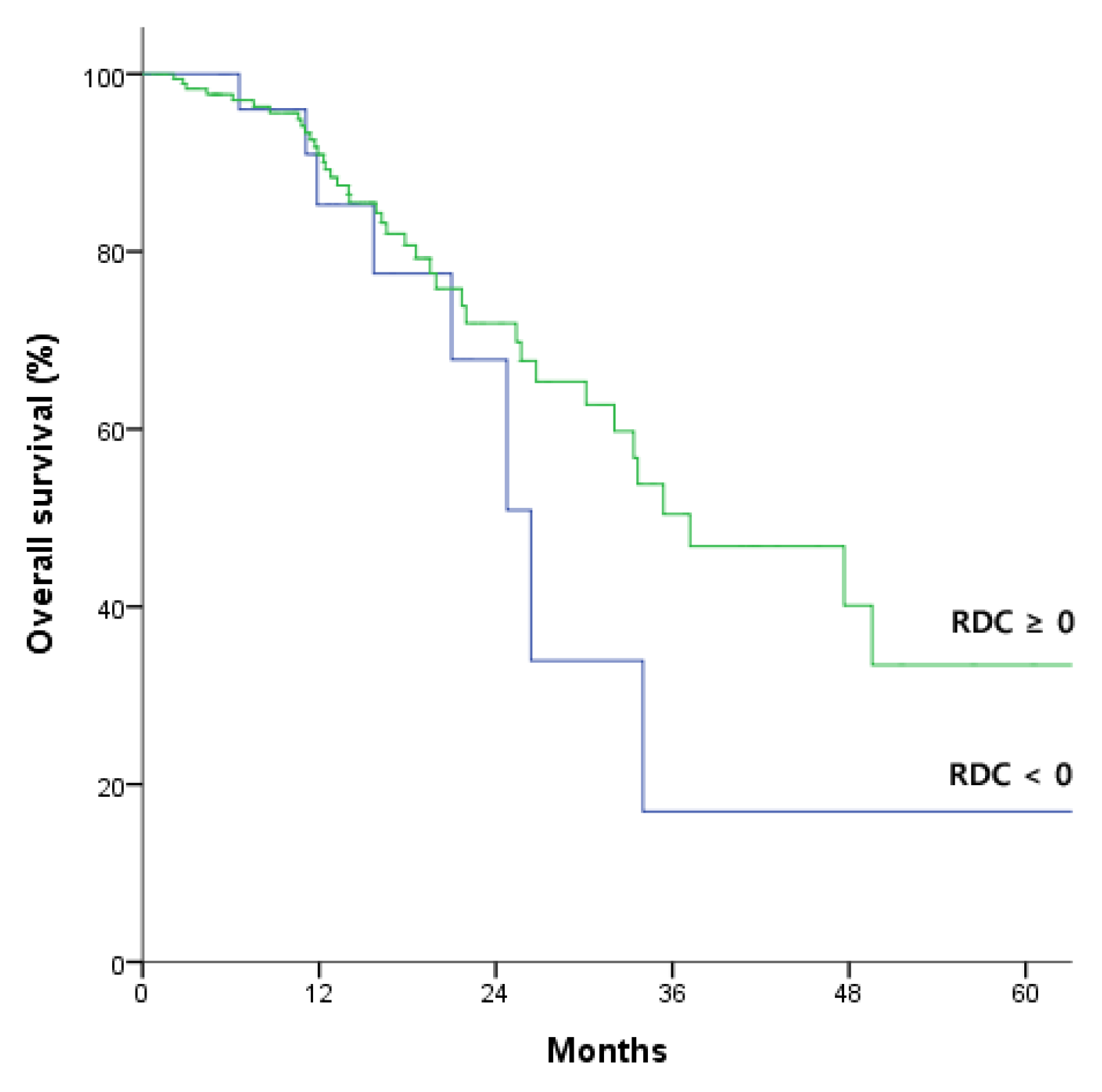
3.2. Prognostic Implications of RDC Based on CA19-9 Concentration before NACT
3.3. Establishment of Prognostic Model for Survival and Recurrence in Patients with pre-NACT 37–1000 U/mL
3.4. Comparative Prognostic Performance of Reduced and Normalized CA 19-9 after NACT and after Surgery
3.5. Prognostic Models in Patients with Borderline Resectable Pancreatic Cancer and Locally Advanced Pancreatic Cancer
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Kaufmann, B.; Hartmann, D.; D’Haese, J.G.; Stupakov, P.; Radenkovic, D.; Gloor, B.; Friess, H. Neoadjuvant Treatment for Borderline Resectable Pancreatic Ductal Adenocarcinoma. Dig. Surg. 2019, 36, 455–461. [Google Scholar] [CrossRef] [PubMed]
- Hoshimoto, S.; Hishinuma, S.; Shirakawa, H.; Tomikawa, M.; Ozawa, I.; Wakamatsu, S.; Hoshi, S.; Hoshi, N.; Hirabayashi, K.; Ogata, Y. Reassessment of the clinical significance of portal-superior mesenteric vein invasion in borderline resectable pancreatic cancer. Eur. J. Surg. Oncol. 2017, 43, 1068–1075. [Google Scholar] [CrossRef] [PubMed]
- Yoo, C.; Shin, S.H.; Kim, K.P.; Jeong, J.H.; Chang, H.M.; Kang, J.H.; Lee, S.S.; Park, D.H.; Song, T.J.; Seo, D.W.; et al. Clinical Outcomes of Conversion Surgery after Neoadjuvant Chemotherapy in Patients with Borderline Resectable and Locally Advanced Unresectable Pancreatic Cancer: A Single-Center, Retrospective Analysis. Cancers 2019, 11, 278. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jang, J.Y.; Han, Y.; Lee, H.; Kim, S.W.; Kwon, W.; Lee, K.H.; Oh, D.Y.; Chie, E.K.; Lee, J.M.; Heo, J.S.; et al. Oncological Benefits of Neoadjuvant Chemoradiation with Gemcitabine Versus Upfront Surgery in Patients With Borderline Resectable Pancreatic Cancer: A Prospective, Randomized, Open-label, Multicenter Phase 2/3 Trial. Ann. Surg. 2018, 268, 215–222. [Google Scholar] [CrossRef]
- Hackert, T.; Ulrich, A.; Buchler, M.W. Borderline resectable pancreatic cancer. Cancer Lett. 2016, 375, 231–237. [Google Scholar] [CrossRef]
- Kieler, M.; Unseld, M.; Bianconi, D.; Schindl, M.; Kornek, G.V.; Scheithauer, W.; Prager, G.W. Impact of New Chemotherapy Regimens on the Treatment Landscape and Survival of Locally Advanced and Metastatic Pancreatic Cancer Patients. J. Clin. Med. 2020, 9, 648. [Google Scholar] [CrossRef] [Green Version]
- Tang, K.; Lu, W.; Qin, W.; Wu, Y. Neoadjuvant therapy for patients with borderline resectable pancreatic cancer: A systematic review and meta-analysis of response and resection percentages. Pancreatology 2016, 16, 28–37. [Google Scholar] [CrossRef]
- Aldakkak, M.; Christians, K.K.; Krepline, A.N.; George, B.; Ritch, P.S.; Erickson, B.A.; Johnston, F.M.; Evans, D.B.; Tsai, S. Pre-treatment carbohydrate antigen 19-9 does not predict the response to neoadjuvant therapy in patients with localized pancreatic cancer. HPB (Oxf.) 2015, 17, 942–952. [Google Scholar] [CrossRef] [Green Version]
- Tsai, S.; George, B.; Wittmann, D.; Ritch, P.S.; Krepline, A.N.; Aldakkak, M.; Barnes, C.A.; Christians, K.K.; Dua, K.; Griffin, M.; et al. Importance of Normalization of CA19-9 Levels Following Neoadjuvant Therapy in Patients With Localized Pancreatic Cancer. Ann. Surg. 2020, 271, 740–747. [Google Scholar] [CrossRef]
- Luo, G.; Fan, Z.; Cheng, H.; Jin, K.; Guo, M.; Lu, Y.; Yang, C.; Fan, K.; Huang, Q.; Long, J.; et al. New observations on the utility of CA19-9 as a biomarker in Lewis negative patients with pancreatic cancer. Pancreatology 2018, 18, 971–976. [Google Scholar] [CrossRef]
- Parra-Robert, M.; Santos, V.M.; Canis, S.M.; Pla, X.F.; Fradera, J.M.A.; Porto, R.M. Relationship Between CA 19.9 and the Lewis Phenotype: Options to Improve Diagnostic Efficiency. Anticancer. Res. 2018, 38, 5883–5888. [Google Scholar] [CrossRef] [PubMed]
- Tempero, M.A.; Malafa, M.P.; Al-Hawary, M.; Asbun, H.; Bain, A.; Behrman, S.W.; Benson, A.B., 3rd; Binder, E.; Cardin, D.B.; Cha, C.; et al. Pancreatic Adenocarcinoma, Version 2.2017, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Cancer Netw. 2017, 15, 1028–1061. [Google Scholar] [CrossRef] [PubMed]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: Revised RECIST guideline (version 1.1). Eur. J. Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef] [PubMed]
- S, N.K.; Serra, S.; Dhani, N.; Hafezi-Bakhtiari, S.; Szentgyorgyi, E.; Vajpeyi, R.; Chetty, R. Regression grading in neoadjuvant treated pancreatic cancer: An interobserver study. J. Clin. Pathol. 2017, 70, 237–243. [Google Scholar] [CrossRef]
- Tzeng, C.W.; Fleming, J.B.; Lee, J.E.; Xiao, L.; Pisters, P.W.; Vauthey, J.N.; Abdalla, E.K.; Wolff, R.A.; Varadhachary, G.R.; Fogelman, D.R.; et al. Defined clinical classifications are associated with outcome of patients with anatomically resectable pancreatic adenocarcinoma treated with neoadjuvant therapy. Ann. Surg. Oncol. 2012, 19, 2045–2053. [Google Scholar] [CrossRef]
- Hartwig, W.; Strobel, O.; Hinz, U.; Fritz, S.; Hackert, T.; Roth, C.; Buchler, M.W.; Werner, J. CA19-9 in potentially resectable pancreatic cancer: Perspective to adjust surgical and perioperative therapy. Ann. Surg. Oncol. 2013, 20, 2188–2196. [Google Scholar] [CrossRef]
- Combs, S.E.; Habermehl, D.; Kessel, K.A.; Bergmann, F.; Werner, J.; Naumann, P.; Jager, D.; Buchler, M.W.; Debus, J. Prognostic impact of CA 19-9 on outcome after neoadjuvant chemoradiation in patients with locally advanced pancreatic cancer. Ann. Surg. Oncol. 2014, 21, 2801–2807. [Google Scholar] [CrossRef]
- Boone, B.A.; Steve, J.; Zenati, M.S.; Hogg, M.E.; Singhi, A.D.; Bartlett, D.L.; Zureikat, A.H.; Bahary, N.; Zeh, H.J., 3rd. Serum CA 19-9 response to neoadjuvant therapy is associated with outcome in pancreatic adenocarcinoma. Ann. Surg. Oncol. 2014, 21, 4351–4358. [Google Scholar] [CrossRef]
- Humphris, J.L.; Chang, D.K.; Johns, A.L.; Scarlett, C.J.; Pajic, M.; Jones, M.D.; Colvin, E.K.; Nagrial, A.; Chin, V.T.; Chantrill, L.A.; et al. The prognostic and predictive value of serum CA19.9 in pancreatic cancer. Ann. Oncol. 2012, 23, 1713–1722. [Google Scholar] [CrossRef]
- Ferrone, C.R.; Finkelstein, D.M.; Thayer, S.P.; Muzikansky, A.; Fernandez-delCastillo, C.; Warshaw, A.L. Perioperative CA19-9 levels can predict stage and survival in patients with resectable pancreatic adenocarcinoma. J. Clin. Oncol. 2006, 24, 2897–2902. [Google Scholar] [CrossRef] [Green Version]
- Luo, G.; Liu, C.; Guo, M.; Cheng, H.; Lu, Y.; Jin, K.; Liu, L.; Long, J.; Xu, J.; Lu, R.; et al. Potential Biomarkers in Lewis Negative Patients With Pancreatic Cancer. Ann. Surg. 2017, 265, 800–805. [Google Scholar] [CrossRef] [PubMed]
- Katz, M.H.; Varadhachary, G.R.; Fleming, J.B.; Wolff, R.A.; Lee, J.E.; Pisters, P.W.; Vauthey, J.N.; Abdalla, E.K.; Sun, C.C.; Wang, H.; et al. Serum CA 19-9 as a marker of resectability and survival in patients with potentially resectable pancreatic cancer treated with neoadjuvant chemoradiation. Ann. Surg. Oncol. 2010, 17, 1794–1801. [Google Scholar] [CrossRef] [PubMed]
- Xia, B.T.; Fu, B.; Wang, J.; Kim, Y.; Ahmad, S.A.; Dhar, V.K.; Levinsky, N.C.; Hanseman, D.J.; Habib, D.A.; Wilson, G.C.; et al. Does radiologic response correlate to pathologic response in patients undergoing neoadjuvant therapy for borderline resectable pancreatic malignancy? J. Surg. Oncol. 2017, 115, 376–383. [Google Scholar] [CrossRef] [PubMed]
- Mellon, E.A.; Jin, W.H.; Frakes, J.M.; Centeno, B.A.; Strom, T.J.; Springett, G.M.; Malafa, M.P.; Shridhar, R.; Hodul, P.J.; Hoffe, S.E. Predictors and survival for pathologic tumor response grade in borderline resectable and locally advanced pancreatic cancer treated with induction chemotherapy and neoadjuvant stereotactic body radiotherapy. Acta Oncol. 2017, 56, 391–397. [Google Scholar] [CrossRef] [Green Version]
- Cassinotto, C.; Sa-Cunha, A.; Trillaud, H. Radiological evaluation of response to neoadjuvant treatment in pancreatic cancer. Diagn. Interv. Imaging 2016, 97, 1225–1232. [Google Scholar] [CrossRef]
- Akita, H.; Takahashi, H.; Ohigashi, H.; Tomokuni, A.; Kobayashi, S.; Sugimura, K.; Miyoshi, N.; Moon, J.H.; Yasui, M.; Omori, T.; et al. FDG-PET predicts treatment efficacy and surgical outcome of pre-operative chemoradiation therapy for resectable and borderline resectable pancreatic cancer. Eur. J. Surg. Oncol. 2017, 43, 1061–1067. [Google Scholar] [CrossRef]
- Kittaka, H.; Takahashi, H.; Ohigashi, H.; Gotoh, K.; Yamada, T.; Tomita, Y.; Hasegawa, Y.; Yano, M.; Ishikawa, O. Role of (18)F-fluorodeoxyglucose positron emission tomography/computed tomography in predicting the pathologic response to preoperative chemoradiation therapy in patients with resectable T3 pancreatic cancer. World J. Surg. 2013, 37, 169–178. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| n (%) or Mean ± SD | |
|---|---|
| Age (years) | 59.7 ± 8.6 |
| Sex (M/F) | 115 (51.1)/110 (48.9) |
| ASA score (I/II/III) | 15 (6.7)/189 (84)/19 (8.4) |
| BRPC/LAPC | 122 (54.2)/103 (45.8) |
| Invasion (SMV/SMA/Both) | 96 (42.7)/27 (12)/95 (42.3) |
| NACT regimen | |
| Gemcitabine based | 58 (25.8) |
| FOLFIRINOX based | 167 (74.2) |
| NACT cycle | 6.5 ± 3.3 |
| Concurrent neoadjuvant radiotherapy | 7 (3.1) |
| CA19-9 before NACT (U/mL) | 676.5 ± 3142.3 |
| CA19-9 after NACT (U/mL) | 188.4 ± 522.1 |
| Median relative change of CA19-9 during NACT | 0.62 (interquartile range: 0.21–0.85) |
| CA19-9 7 days after surgery (U/mL) | 166.0 ± 1500.4 |
| Preoperative response on CT (PR/SD) | 67 (29.8)/158 (70.2) |
| Operation time | 315.2 ± 97.4 |
| Operation (PD/DP/TP/Palliative surgery) | 138 (61.3)/67 (29.8)/16 (7.1)/4 (1.7) |
| Intraoperative transfusion | 37 (16.4) |
| Vessel resection (vein/artery) | 95 (57.8)/41 (18.2) |
| Adjacent organ resection | 19 (8.4) |
| Postoperative complication | 44 (19.6) |
| Differentiation (CR/WD/MD/PD/UD) | 5 (2.2)/26 (11.6)/172 (76.4)/16 (7.1)/2 (0.9) |
| T-stage (CR/1/2/3/4), AJCC 8th | 5 (2.2)/63 (28.0)/124 (55.1)/29 (12.9)/4 (1.8) |
| N-stage (0/1/2), AJCC 8th | 122 (54.2)/80 (35.6)/23 (10.2) |
| Resection margin (R0/R1) | 173 (76.9)/48 (21.3) |
| CA19-9 before NACT | HR | 95% CI | p-Value | |
|---|---|---|---|---|
| Overall survival | <37 U/mL (n = 62) | 0.851 | 0.100–7.241 | 0.882 |
| 37–1000 U/m (n = 133) | 0.262 | 0.092–0.748 | 0.012 | |
| >1000 U/mL (n = 26) | 8.075 | 0.163–399.699 | 0.294 | |
| Recurrence free survival | <37 U/mL (n = 62) | 0.708 | 0.222–2.257 | 0.560 |
| 37–1000 U/mL (n = 133) | 0.290 | 0.134–0.628 | 0.002 | |
| >1000 U/mL (n = 26) | 1.016 | 0.211–4.888 | 0.985 |
| Univariate Analysis | Multivariate Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Variables | HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age | 1.019 | 0.978–1.062 | 0.368 | ||||
| Sex | 0.884 | 0.434–1.801 | 0.734 | ||||
| Partial response on preoperative CT | 1.076 | 0.792–1.460 | 0.640 | ||||
| Adjacent vein resection | 2.121 | 1.028–4.377 | 0.042 | 1.923 | 0.897–4.122 | 0.093 | |
| Cell differentiation | WD,MD/PD,UD | 3.202 | 1.243–8.245 | 0.016 | |||
| T-stage (AJCC 8th) | 1,2/3,4 | 1.124 | 0.500–2.524 | 0.777 | |||
| N-stage (AJCC 8th) | N0 (ref) | 1 | 0.560 | ||||
| N1 | 1.144 | 0.524–2.496 | 0.736 | ||||
| N2 | 1.806 | 0.649–5.021 | 0.257 | ||||
| Tumor regression grade | 0,1/2,3 | 1.139 | 0.403–3.219 | 0.806 | |||
| Lympho-vascular invasion | 1.637 | 0.802–3.342 | 0.175 | ||||
| Perineural invasion | 1.306 | 0.531–3.209 | 0.561 | ||||
| RDC | 0.262 | 0.092–0.748 | 0.012 | 0.262 | 0.093–0.739 | 0.011 | |
| R1 resection | 1.366 | 0.621–3.004 | 0.437 | ||||
| Intraoperative transfusion | 2.172 | 1.022–4.619 | 0.044 | 1.977 | 0.910–4.296 | 0.085 | |
| Univariate Analysis | MultivAriate Analysis | ||||||
|---|---|---|---|---|---|---|---|
| Variables | HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age | 0.987 | 0.965–1.010 | 0.263 | ||||
| Sex | 1.161 | 0.745–1.808 | 0.509 | ||||
| Partial response on preoperative CT | 0.873 | 0.600–1.270 | 0.478 | ||||
| Adjacent vein resection | 1.687 | 1.075–2.649 | 0.023 | 1.612 | 1.021–2.545 | 0.040 | |
| Cell differentiation | WD,MD/PD,UD | 1.184 | 0.577–2.429 | 0.198 | |||
| Tumor regression grade | 0,1/2,3 | 1.531 | 0.800–2.930 | 0.198 | |||
| Lympho-vascular invasion | 1.337 | 0.847–2.110 | 0.212 | ||||
| Perineural invasion | 1.261 | 0.751–2.118 | 0.381 | ||||
| T-stage (AJCC 8th) | 1,2/3,4 | 0.923 | 0.568–1.501 | 0.747 | |||
| N-stage (AJCC 8th) | N0 (ref) | 0.159 | |||||
| N1 | 1.550 | 0.208–11.553 | 0.669 | ||||
| N2 | 1.883 | 0.984-3.607 | 0.056 | ||||
| RDC | 0.290 | 0.134–0.628 | 0.002 | 0.299 | 0.140–0.642 | 0.002 | |
| R1 resection | 1.459 | 0.873–2.437 | 0.150 | ||||
| Intraoperative transfusion | 1.171 | 0.667–2.056 | 0.583 | ||||
| Outcome | Prognostic Model | C-Index | 95% CI | p-Value (1 vs. 2) | p-Value (1 vs. 3) | AIC | 95% CI | p-Value (1 vs. 2) | p-Value (1 vs. 3) |
|---|---|---|---|---|---|---|---|---|---|
| Overall survival | Model 1 | 0.653 | 0.530–0.784 | 0.904 | 0.680 | 227.243 | 142.091–297.964 | 0.896 | 0.912 |
| Model 2 | 0.625 | 0.501–0.767 | 230.897 | 145.695–303.928 | |||||
| Model 3 | 0.613 | 0.523–0.760 | 233.114 | 148.409–305.646 | |||||
| Recurrence free survival | Model 1 | 0.604 | 0.534–0.676 | 0.812 | 0.592 | 636.138 | 546.638–726.578 | 0.900 | 0.924 |
| Model 2 | 0.584 | 0.532–0.654 | 640.246 | 548.808–727.833 | |||||
| Model 3 | 0.602 | 0.547–0.673 | 638.247 | 545.773–722.073 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, W.; Park, Y.; Kwon, J.W.; Jun, E.; Song, K.B.; Lee, J.H.; Hwang, D.W.; Yoo, C.; Kim, K.-p.; Jeong, J.H.; et al. Reduced and Normalized Carbohydrate Antigen 19-9 Concentrations after Neoadjuvant Chemotherapy Have Comparable Prognostic Performance in Patients with Borderline Resectable and Locally Advanced Pancreatic Cancer. J. Clin. Med. 2020, 9, 1477. https://doi.org/10.3390/jcm9051477
Lee W, Park Y, Kwon JW, Jun E, Song KB, Lee JH, Hwang DW, Yoo C, Kim K-p, Jeong JH, et al. Reduced and Normalized Carbohydrate Antigen 19-9 Concentrations after Neoadjuvant Chemotherapy Have Comparable Prognostic Performance in Patients with Borderline Resectable and Locally Advanced Pancreatic Cancer. Journal of Clinical Medicine. 2020; 9(5):1477. https://doi.org/10.3390/jcm9051477
Chicago/Turabian StyleLee, Woohyung, Yejong Park, Jae Woo Kwon, Eunsung Jun, Ki Byung Song, Jae Hoon Lee, Dae Wook Hwang, Changhoon Yoo, Kyu-pyo Kim, Jae Ho Jeong, and et al. 2020. "Reduced and Normalized Carbohydrate Antigen 19-9 Concentrations after Neoadjuvant Chemotherapy Have Comparable Prognostic Performance in Patients with Borderline Resectable and Locally Advanced Pancreatic Cancer" Journal of Clinical Medicine 9, no. 5: 1477. https://doi.org/10.3390/jcm9051477