
Sense of Coherence Predicts Physical Activity Maintenance and Health-Related Quality of Life: A 3-Year Longitudinal Study on Cardiovascular Patients

 ,
,  , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Measures
2.2.1. Physical Activity
2.2.2. Sense of Coherence
2.2.3. Health-Related Quality of Life
2.3. Data Analysis
3. Results
3.1. Preliminary Analysis
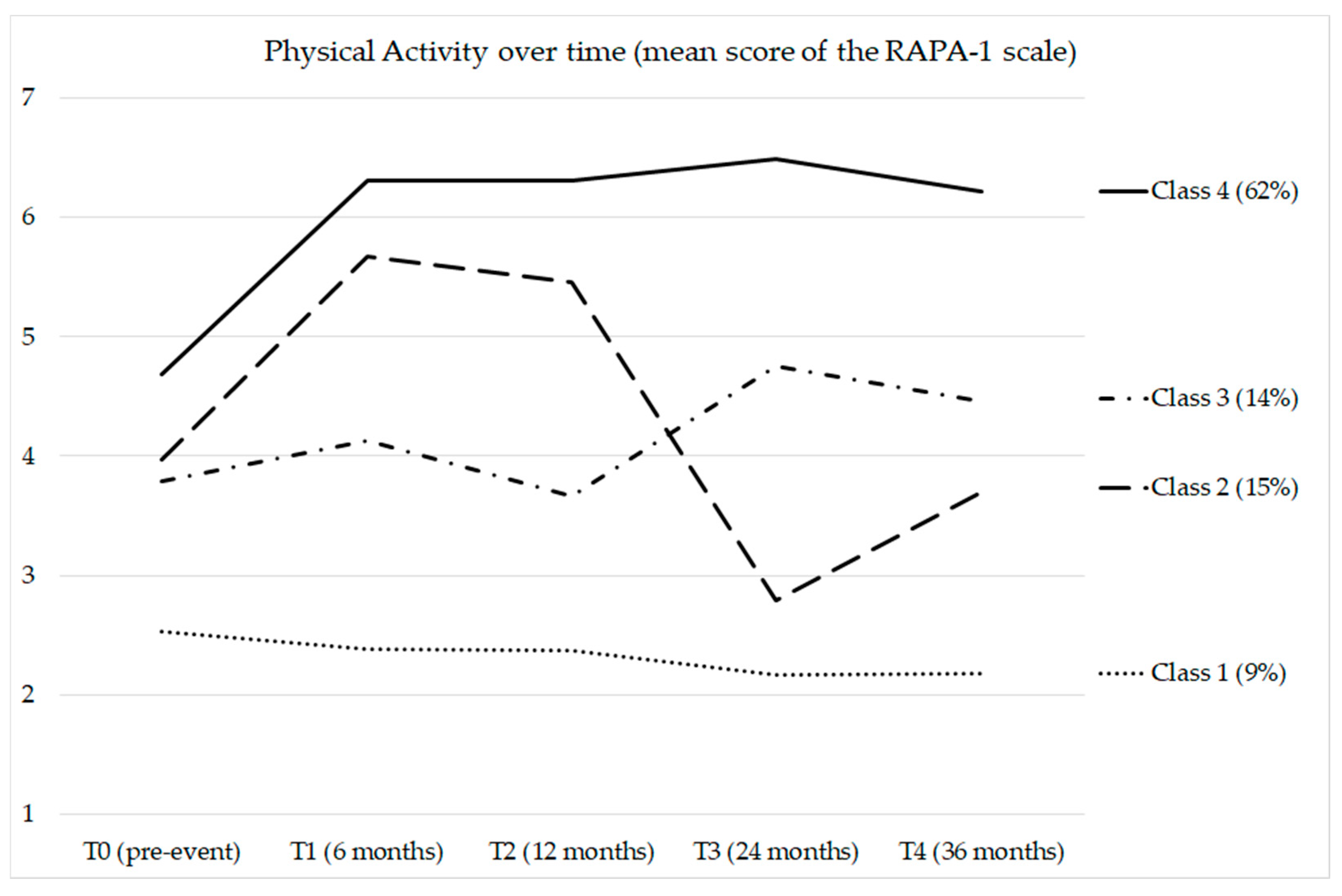
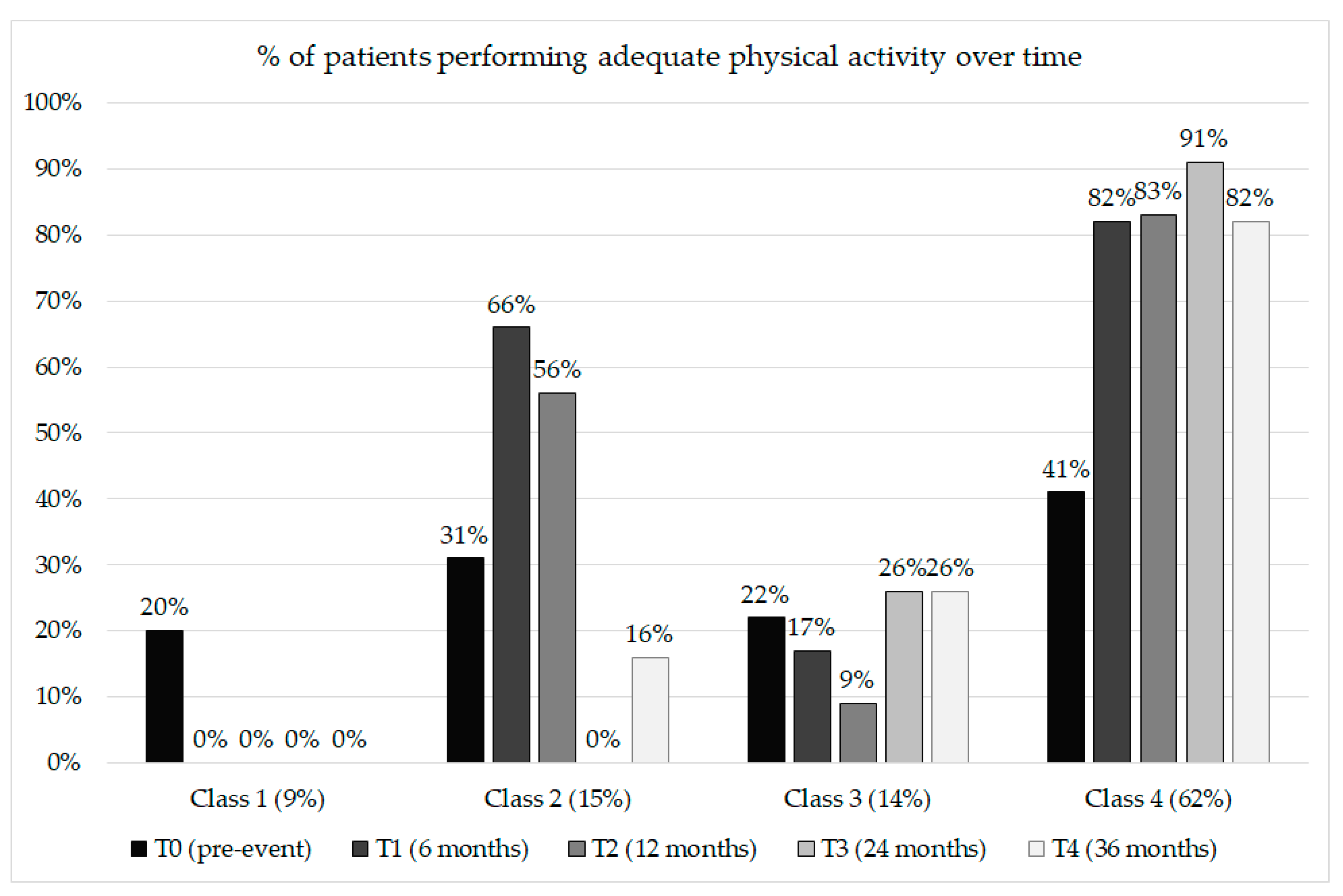
3.2. Longitudinal Profiles of Physical Activity
3.3. Prediction of the Probability of Belonging to the Target Physical Activity Profile
3.4. Prediction of HRQoL at the Final Follow-Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: Executive Summary. J. Am. Coll. Cardiol. 2019, 74, 1376–1414. [Google Scholar] [CrossRef] [PubMed]
- Timmis, A.; Townsend, N.; Gale, C.P.; Torbica, A.; Lettino, M.; Petersen, S.E.; Mossialos, E.A.; Maggioni, A.P.; Kazakiewicz, D.; May, H.T.; et al. European Society of Cardiology: Cardiovascular Disease Statistics 2019. Eur. Heart J. 2019, 41, 12–85. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Global Action Plan for the Prevention and Control of Noncommunicable Diseases 2013–2020. 2013. Available online: https://www.who.int/publications/i/item/9789241506236 (accessed on 15 February 2022).
- Yusuf, S.; Hawken, S.; Ounpuu, S.; Dans, T.; Avezum, A.; Lanas, F.; McQueen, M.; Budaj, A.; Pais, P.; Varigos, J.; et al. Effect of Potentially Modifiable Risk Factors Associated with Myocardial Infarction in 52 Countries (the INTERHEART Study): Case-Control Study. Lancet 2004, 364, 937–952. [Google Scholar] [CrossRef]
- Yusuf, S.; Joseph, P.; Rangarajan, S.; Islam, S.; Mente, A.; Hystad, P.; Brauer, M.; Kutty, V.R.; Gupta, R.; Wielgosz, A.; et al. Modifiable risk factors, cardiovascular disease, and mortality in 155 722 individuals from 21 high-income, middle-income, and low-income countries (PURE): A prospective cohort study. Lancet 2020, 395, 795–808. [Google Scholar] [CrossRef] [Green Version]
- Hamer, M.; O’Donovan, G.; Murphy, M. Physical Inactivity and the Economic and Health Burdens Due to Cardiovascular Disease: Exercise as Medicine. Adv. Exp. Med. Biol. 2017, 999, 3–18. [Google Scholar] [CrossRef] [PubMed]
- Christian, A.H.; Cheema, A.F.; Smith, S.C.; Mosca, L. Predictors of quality of life among women with coronary heart disease. Qual. Life Res. 2007, 16, 363–373. [Google Scholar] [CrossRef]
- Hawkes, A.L.; Patrao, T.A.; Ware, R.; Atherton, J.J.; Taylor, C.B.; Oldenburg, B.F. Predictors of physical and mental health-related quality of life outcomes among myocardial infarction patients. BMC Cardiovasc. Disord. 2013, 13, 69. [Google Scholar] [CrossRef] [Green Version]
- Wardoku, R.; Blair, C.; Demmer, R.; Prizment, A. Association between physical inactivity and health-related quality of life in adults with coronary heart disease. Maturitas 2019, 128, 36–42. [Google Scholar] [CrossRef]
- Conraads, V.M.; Deaton, C.; Piotrowicz, E.; Santaularia, N.; Tierney, S.; Piepoli, M.F.; Pieske, B.; Schmid, J.P.; Dickstein, K.; Ponikowski, P.P.; et al. Adherence of heart failure patients to exercise: Barriers and possible solutions: A position statement of the Study Group on Exercise Training in Heart Failure of the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2012, 14, 451–458. [Google Scholar] [CrossRef]
- Kotseva, K.; De Backer, G.; De Bacquer, D.; Rydén, L.; Hoes, A.; Grobbee, D.; Maggioni, A.; Marques-Vidal, P.; Jennings, C.; Abreu, A.; et al. Lifestyle and Impact on Cardiovascular Risk Factor Control in Coronary Patients across 27 Countries: Results from the European Society of Cardiology ESC-EORP EUROASPIRE V Registry. Eur. J. Prev. Cardiol. 2019, 26, 824–835. [Google Scholar] [CrossRef]
- Greco, A.; Brugnera, A.; Adorni, R.; D’Addario, M.; Fattirolli, F.; Franzelli, C.; Giannattasio, C.; Maloberti, A.; Zanatta, F.; Steca, P. Protein Intake and Physical Activity in Newly Diagnosed Patients with Acute Coronary Syndrome: A 5-Year Longitudinal Study. Nutrients 2021, 13, 634. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Patao, C.; Chuang, J.; Wong, N.D. Cardiovascular Risk Factor Control and Adherence to Recommended Lifestyle and Medical Therapies in Persons with Coronary Heart Disease (from the National Health and Nutrition Examination Survey 2007-2010). Am. J. Cardiol. 2013, 112, 1126–1132. [Google Scholar] [CrossRef] [PubMed]
- Mozaffarian, D.; Benjamin, E.J.; Go, A.S.; Arnett, D.K.; Blaha, M.J.; Cushman, M.; Das, S.R.; de Ferranti, S.; Després, J.P.; Fullerton, H.J.; et al. Stroke Statistics Subcommittee. Heart Disease and Stroke Statistics-2016 Update: A Report from the American Heart Association. Circulation 2016, 133, e38–e360. [Google Scholar] [CrossRef] [PubMed]
- Steca, P.; Pancani, L.; Cesana, F.; Fattirolli, F.; Giannattasio, C.; Greco, A.; D’Addario, M.; Monzani, D.; Cappelletti, E.R.; Magrin, M.E.; et al. Changes in physical activity among coronary and hypertensive patients: A longitudinal study using the Health Action Process Approach. Psychol. Health 2017, 32, 361–380. [Google Scholar] [CrossRef] [PubMed]
- Riera-Sampol, A.; Bennasar-Veny, M.; Tauler, P.; Nafría, M.; Colom, M.; Aguilo, A. Association between Depression, Lifestyles, Sleep Quality, and Sense of Coherence in a Population with Cardiovascular Risk. Nutrients 2021, 13, 585. [Google Scholar] [CrossRef]
- Rosenfeld, C.S. Sex-dependent differences in voluntary physical activity: Physical activity and sex differences. J. Neurosci. Res. 2017, 95, 279–290. [Google Scholar] [CrossRef] [Green Version]
- Wittmer, M.; Volpatti, M.; Piazzalonga, S.; Hoffmann, A. Expectation, satisfaction, and predictors of dropout in cardiac rehabilitation. Eur. J. Prev. Cardiol. 2012, 19, 1082–1088. [Google Scholar] [CrossRef]
- Murray, J.; Craigs, C.L.; Hill, K.M.; Honey, S.; House, A. A Systematic Review of Patient Reported Factors Associated with Uptake and Completion of Cardiovascular Lifestyle Behaviour Change. BMC Cardiovasc. Disord. 2012, 12, 120. [Google Scholar] [CrossRef] [Green Version]
- Kubzansky, L.D.; Huffman, J.C.; Boehm, J.K.; Hernandez, R.; Kim, E.S.; Koga, H.K.; Feig, E.H.; Lloyd-Jones, D.M.; Seligman, M.E.P.; Labarthe, D.R. Positive Psychological Well-Being and Cardiovascular Disease: JACC Health Promotion Series. J. Am. Coll. Cardiol. 2018, 72, 1382–1396. [Google Scholar] [CrossRef]
- Antonovsky, A. Health, Stress, and Coping: New Perspectives on Mental and Physical Well-Being; Jossey-Bass Publishers: San Francisco, CA, USA, 1979. [Google Scholar]
- Eriksson, M.; Lindstrom, B. Antonovsky’s Sense of Coherence Scale and the Relation with Health: A Systematic Review. J. Epidemiol. Commun. Health 2006, 60, 376–381. [Google Scholar] [CrossRef]
- Bergman, E.; Malm, D.; Karlsson, J.E.; Berterö, C. Longitudinal study of patients after myocardial infarction: Sense of coherence, quality of life, and symptoms. Heart Lung 2009, 38, 129–140. [Google Scholar] [CrossRef] [PubMed]
- Kattainen, E.; Meriläinen, P.; Sintonen, H. Sense of coherence and health-related quality of life among patients undergoing coronary artery bypass grafting or angioplasty. Eur. J. Cardiovasc. Nurs. 2006, 5, 21–30. [Google Scholar] [CrossRef] [PubMed]
- Silarova, B.; Nagyova, I.; Rosenberger, J.; Studencan, M.; Ondusova, D.; Reijneveld, S.A.; van Dijk, J.P. Sense of coherence as an independent predictor of health-related quality of life among coronary heart disease patients. Qual. Life Res. 2012, 21, 1863–1871. [Google Scholar] [CrossRef] [Green Version]
- Adorni, R.; Zanatta, F.; D’Addario, M.; Atella, F.; Costantino, E.; Iaderosa, C.; Petarle, G.; Steca, P. Health-Related Lifestyle Profiles in Healthy Adults: Associations with Sociodemographic Indicators, Dispositional Optimism, and Sense of Coherence. Nutrients 2021, 13, 3778. [Google Scholar] [CrossRef] [PubMed]
- Thomas, K.; Nilsson, E.; Festin, K.; Henriksson, P.; Lowén, M.; Löf, M.; Kristenson, M. Associations of Psychosocial Factors with Multiple Health Behaviors: A Population-Based Study of Middle-Aged Men and Women. Int. J. Environ. Res. Public Health 2020, 17, 1239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wainwright, N.W.J.; Surtees, P.G.; Welch, A.A.; Luben, R.N.; Khaw, K.-T.; Bingham, S.A. Sense of Coherence, Lifestyle Choices and Mortality. J. Epidemiol. Commun. Health 2008, 62, 829–831. [Google Scholar] [CrossRef]
- Myers, V.; Drory, Y.; Gerber, Y. Israel Study Group on First Acute Myocardial Infarction. Sense of coherence predicts post-myocardial infarction trajectory of leisure time physical activity: A prospective cohort study. BMC Public Health 2011, 11, 708. [Google Scholar] [CrossRef] [Green Version]
- Karlsson, I.; Berglin, E.; Larsson, P.A. Sense of coherence: Quality of life before and after coronary artery bypass surgery—a longitudinal study. J. Adv. Nurs. 2000, 31, 1383–1392. [Google Scholar] [CrossRef]
- Calabrò, P.; Gragnano, F.; Di Maio, M.; Patti, G.; Antonucci, E.; Cirillo, P.; Gresele, P.; Palareti, G.; Pengo, V.; Pignatelli, P.; et al. Epidemiology and Management of Patients with Acute Coronary Syndromes in Contemporary Real-World Practice: Evolving Trends from the EYESHOT Study to the START-ANTIPLATELET Registry. Angiology 2018, 69, 795–802. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Lawrence Erlbaum Associates Inc.: Mahwah, NJ, USA, 1988. [Google Scholar]
- Faul, F.; Erdfelder, E.; Lang, A.-G.; Buchner, A. G*Power 3: A Flexible Statistical Power Analysis Program for the Social, Behavioral, and Biomedical Sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Topolski, T.D.; LoGerfo, J.; Patrick, D.L.; Williams, B.; Walwick, J.; Patrick, M.B. The Rapid Assessment of Physical Activity (RAPA) among Older Adults. Prev. Chronic Dis. 2006, 3, A118. [Google Scholar] [PubMed]
- Antonovsky, A. The Structure and Properties of the Sense of Coherence Scale. Soc. Sci. Med. 1993, 36, 725–733. [Google Scholar] [CrossRef]
- Barni, D.; Tagliabue, S. Sense of coherence scale di Antonovsky: Un contributo alla validazione italiana. TPM Test. Psicometria Metodol. 2005, 3, 151–166. [Google Scholar]
- Rabin, R.; de Charro, F. EQ-5D: A measure of health status from the EuroQol Group. Ann. Med. 2001, 33, 337–343. [Google Scholar] [CrossRef]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 7th ed.; Muthén and Muthén: Los Angeles, CA, USA, 2015. [Google Scholar]
- Hair, J.; Black, W.C.; Babin, B.J.; Anderson, R.E. Multivariate Data Analysis, 7th ed.; Pearson Educational International: London, UK, 2010. [Google Scholar]
- Nylund, K.L.; Asparouhov, T.; Muthén, B.O. Deciding on the number of classes in latent class analysis and growth mixture modeling: A Monte Carlo simulation study. Struct. Equ. Modeling A Multidiscip. J. 2007, 14, 535–569. [Google Scholar] [CrossRef]
- Willett, J.B.; Sayer, A.G. Using covariance structure analysis to detect correlates and predictors of individual change over time. Psychol. Bull. 1994, 116, 363. [Google Scholar] [CrossRef]
- Celeux, G.; Soromenho, G. An entropy criterion for assessing the number of clusters in a mixture model. J. Classif. 1996, 13, 195–212. [Google Scholar] [CrossRef] [Green Version]
- Lo, Y.; Mendell, N.R.; Rubin, D.B. Testing the number of components in a normal mixture. Biometrika 2001, 88, 767–778. [Google Scholar] [CrossRef]
- Hansen, W.B.; Tobler, N.S.; Graham, J.W. Attrition in substance abuse prevention research: A metaanalysis of 85 longitudinally followed cohorts. Eval. Rev. 1990, 14, 677–685. [Google Scholar] [CrossRef]
- Arbuckle, J.L.; Marcoulides, G.A.; Schumacker, R.E. Full information estimation in the presence of incomplete data. Adv. Struct. Equ. Modeling Issues Tech. 1996, 243, 277. [Google Scholar]
- Donders, A.R.; van der Heijden, G.J.; Stijnen, T.; Moons, K.G. Review: A gentle introduction to imputation of missing values. J. Clin. Epidemiol. 2006, 59, 1087–1091. [Google Scholar] [CrossRef] [PubMed]
- Little, R.J.A. Modeling the drop-out mechanism in repeated-measures studies. J. Am. Stat. Assoc. 1995, 90, 1112–1121. [Google Scholar] [CrossRef]
- Muthén, B. Latent Variable Analysis: Growth Mixture Modeling and Related Techniques for Longitudinal Data. In Handbook of Quantitative Methodology for the Social Sciences; Kaplan, D., Ed.; Sage: Newbury Park, CA, USA, 2004; pp. 345–368. [Google Scholar]
- Muthén, B.; Shedden, K. Finite mixture modeling with mixture outcomes using the EM algorithm. Biometrics 1999, 55, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Schafer, J.L.; Graham, J.W. Missing data: Our view of the state of the art. Psychol. Methods 2002, 7, 147–177. [Google Scholar] [CrossRef] [PubMed]
- Kristman, V.; Manno, M.; Côté, P. Loss to follow-up in cohort studies: How much is too much? Eur. J. Epidemiol. 2004, 19, 751–760. [Google Scholar] [CrossRef] [PubMed]
- Munyombwe, T.; Hall, M.; Dondo, T.B.; Alabas, O.A.; Gerard, O.; West, R.M.; Pujades-Rodriguez, M.; Hall, A.; Gale, C.P. Quality of Life Trajectories in Survivors of Acute Myocardial Infarction: A National Longitudinal Study. Heart 2020, 106, 33–39. [Google Scholar] [CrossRef]
- Sciomer, S.; Moscucci, F.; Maffei, S.; Gallina, S.; Mattioli, A. Prevention of cardiovascular risk factors in women: The lifestyle paradox and stereotypes we need to defeat. Eur. J. Prev. Cardiolog. 2019, 26, 609–610. [Google Scholar] [CrossRef]
- Zhang, Y.; Yang, J.; Hou, W.; Arcan, C. Obesity Trends and Associations with Types of Physical Activity and Sedentary Behavior in US Adults: National Health and Nutrition Examination Survey, 2007-2016. Obesity 2021, 29, 240–250. [Google Scholar] [CrossRef]
- Staniute, M.; Bunevicius, A.; Brozaitiene, J.; Bunevicius, R. Relationship of health-related quality of life with fatigue and exercise capacity in patients with coronary artery disease. Eur. J. Cardiovasc. Nurs. 2014, 13, 338–344. [Google Scholar] [CrossRef]
- Meader, N.; King, K.; Moe-Byrne, T.; Wright, K.; Graham, H.; Petticrew, M.; Power, C.; White, M.; Sowden, A.J. A systematic review on the clustering and co-occurrence of multiple risk behaviours. BMC Public Health 2016, 16, 657. [Google Scholar] [CrossRef] [Green Version]
- Price, J.H.; Khubchandani, J.; Webb, F.J. Poverty and Health Disparities: What Can Public Health Professionals Do? Health Promot. Pr. 2018, 19, 170–174. [Google Scholar] [CrossRef]
- Reyes, M.-F.; Satorres, E.; Meléndez, J.C. Resilience and Socioeconomic Status as Predictors of Life Satisfaction and Psychological Well-Being in Colombian Older Adults. J. Appl. Gerontol. 2020, 39, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Geng, L. Effects of Socioeconomic Status on Physical and Psychological Health: Lifestyle as a Mediator. Int. J. Environ. Res. Public Health 2019, 16, 281. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prince, S.A.; Adamo, K.B.; Hamel, M.E.; Hardt, J.; Gorber, S.C.; Tremblay, M. A Comparison of Direct versus Self-Report Measures for Assessing Physical Activity in Adults: A Systematic Review. Int. J. Behav. Nutr. Phys. Act. 2008, 5, 1–24. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wunsch, K.; Kienberger, K.; Niessner, C. Changes in Physical Activity Patterns Due to the COVID-19 Pandemic: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 2250. [Google Scholar] [CrossRef] [PubMed]
- Van Bakel, B.M.A.; Bakker, E.A.; de Vries, F.; Thijssen, D.H.J.; Eijsvogels, T.M.H. Changes in Physical Activity and Sedentary Behaviour in Cardiovascular Disease Patients during the COVID-19 Lockdown. Int. J. Environ. Res. Public Health 2021, 18, 11929. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Sociodemographic Variables | |
|---|---|
| Age, mean (SD; range) | 57.1 (7.87; 34–77) |
| Gender, n (%) | |
| Male | 231 (84%) |
| Female | 44 (16%) |
| Working status, n (%) | |
| working | 163 (59.3%) |
| not working | 112 (40.7%) |
| Educational level, n (%) | |
| less than high school | 141 (51.3%) |
| high school or higher | 134 (48.7%) |
| Marital status, n (%) | |
| single\widowed\divorced | 78 (28.4%) |
| married | 197 (71.6%) |
| Clinical Variables | |
|---|---|
| Clinical Presentation, n (%) | |
| Non-ST elevation myocardial infarction (NSTEMI) | 54 (19.8) |
| ST-elevation myocardial infarction (STEMI) | 196 (71.8) |
| Unstable Angina | 23 (8.5) |
| Percutaneous coronary intervention, n (%) | 258 (94.5) |
| Patients with at least one stent, n (%) | 263 (96) |
| Risk factors, n (%) | |
| Hypertension | 127 (46.5) |
| Dyslipidemia | 143 (52.4) |
| Smoking History | 180 (66.4) |
| Diabetes | 47 (17.2) |
| Obesity | 43 (15.8) |
| Family History of CVD | 108 (39.3) |
| Physical Inactivity | 20 (7.3) |
| Body Mass Index, mean (SD) | 27.2 (4.1) |
| Systolic Blood Pressure (SBP), mean (SD) | 115.9 (13.9) |
| Diastolic Blood Pressure (DBP), mean (SD) | 72.9 (8.5) |
| Number of Classes | BIC | E | LMRT | p | BLR | p |
|---|---|---|---|---|---|---|
| 1 | 4773.11 | |||||
| 2 | 4516.77 | 0.77 | 284.43 | 0.249 | 284.43 | 0.000 |
| 3 | 4473.01 | 0.79 | 71.84 | 0.017 | 71.84 | 0.000 |
| 4 | 4447.78 | 0.78 | 53.31 | 0.032 | 53.31 | 0.000 |
| 5 | 4448.08 | 0.82 | 27.79 | 0.155 | 27.79 | 0.000 |
| Physical Activity: Mean Score (SD) and % of Adequateness | ||||||||
|---|---|---|---|---|---|---|---|---|
| Class | n (%) | Mean Age at t0 (SD) | n Men (%) | t0 | t1 | t2 | t3 | t4 |
| 1 | 25 (9) | 56.9 (7.9) | 20 (80) | 2.53 (1.84) 20% | 2.38 (1.20) 0% | 2.37 (0.99) 0% | 2.17 (0.85) 0% | 2.18 (1.22) 0% |
| 2 | 42 (15) | 58.1 (7.8) | 30 (71) | 3.98 (1.71) 31% | 5.67 (1.26) 66% | 5.45 (1.37) 56% | 2.79 (0.95) 0% | 3.70 (1.66) 16% |
| 3 | 37 (14) | 57.9 (7.4) | 29 (78) | 3.79 (1.83) 22% | 4.13 (1.69) 17% | 3.67 (1.52) 9% | 4.75 (1.09) 26% | 4.46 (1.65) 26% |
| 4 | 171 (62) | 56.6 (8.0) | 152 (89) | 4.68 (1.99) 41% | 6.30 (1.13) 82% | 6.31 (1.01) 83% | 6.49 (0.70) 91% | 6.22 (1.18) 82% |
| 95% Confidence Interval | |||||
|---|---|---|---|---|---|
| Predictor | t | p | Standardized β | Lower | Upper |
| Age | −1.32 | 0.187 | −0.08 | −0.20 | 0.04 |
| Gender (male–female) | 2.14 | 0.033 | 0.35 | 0.03 | 0.67 |
| Obesity (no–yes) | 2.11 | 0.036 | 0.34 | 0.02 | 0.66 |
| SOC | 3.19 | 0.002 | 0.19 | 0.07 | 0.31 |
| 95% Confidence Interval | |||||
|---|---|---|---|---|---|
| Predictor | t | p | Standardized β | Lower | Upper |
| Prob. of class 4 | 2.17 | 0.031 | 0.16 | 0.01 | 0.31 |
| SOC | 3.67 | <0.001 | 0.27 | 0.13 | 0.3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Adorni, R.; Greco, A.; D’Addario, M.; Zanatta, F.; Fattirolli, F.; Franzelli, C.; Maloberti, A.; Giannattasio, C.; Steca, P. Sense of Coherence Predicts Physical Activity Maintenance and Health-Related Quality of Life: A 3-Year Longitudinal Study on Cardiovascular Patients. Int. J. Environ. Res. Public Health 2022, 19, 4700. https://doi.org/10.3390/ijerph19084700
Adorni R, Greco A, D’Addario M, Zanatta F, Fattirolli F, Franzelli C, Maloberti A, Giannattasio C, Steca P. Sense of Coherence Predicts Physical Activity Maintenance and Health-Related Quality of Life: A 3-Year Longitudinal Study on Cardiovascular Patients. International Journal of Environmental Research and Public Health. 2022; 19(8):4700. https://doi.org/10.3390/ijerph19084700
Chicago/Turabian StyleAdorni, Roberta, Andrea Greco, Marco D’Addario, Francesco Zanatta, Francesco Fattirolli, Cristina Franzelli, Alessandro Maloberti, Cristina Giannattasio, and Patrizia Steca. 2022. "Sense of Coherence Predicts Physical Activity Maintenance and Health-Related Quality of Life: A 3-Year Longitudinal Study on Cardiovascular Patients" International Journal of Environmental Research and Public Health 19, no. 8: 4700. https://doi.org/10.3390/ijerph19084700