
HPV-Negative Cervical Cancer: A Narrative Review

 , ,
, ,  ,
,  , and
, and
Abstract
:1. Introduction
2. Methods
3. HPV-Negative CC Prevalence and Histotypes
3.1. Pathology of NHPVA
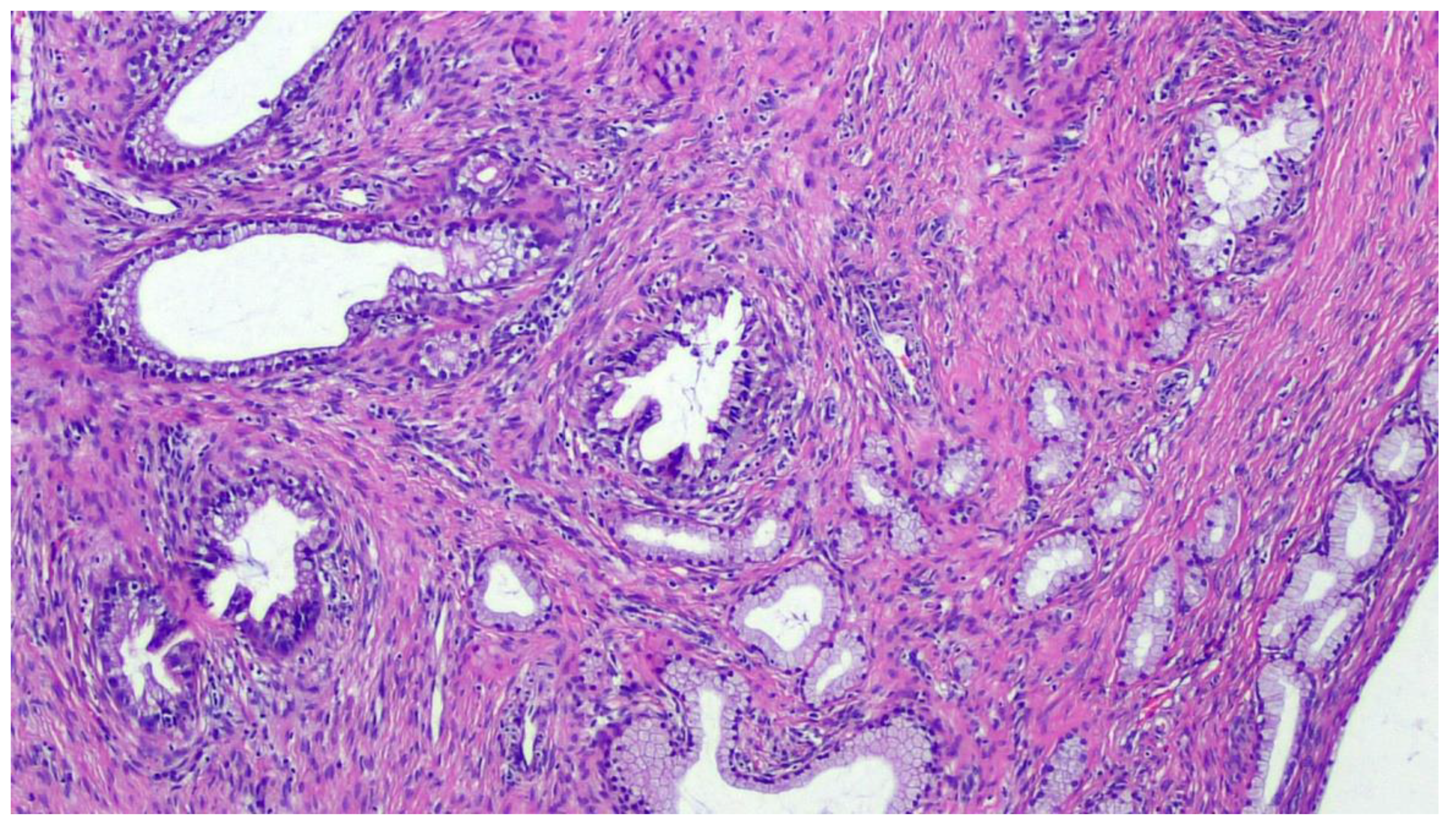
3.1.1. Gastric-Type Endocervical ADC
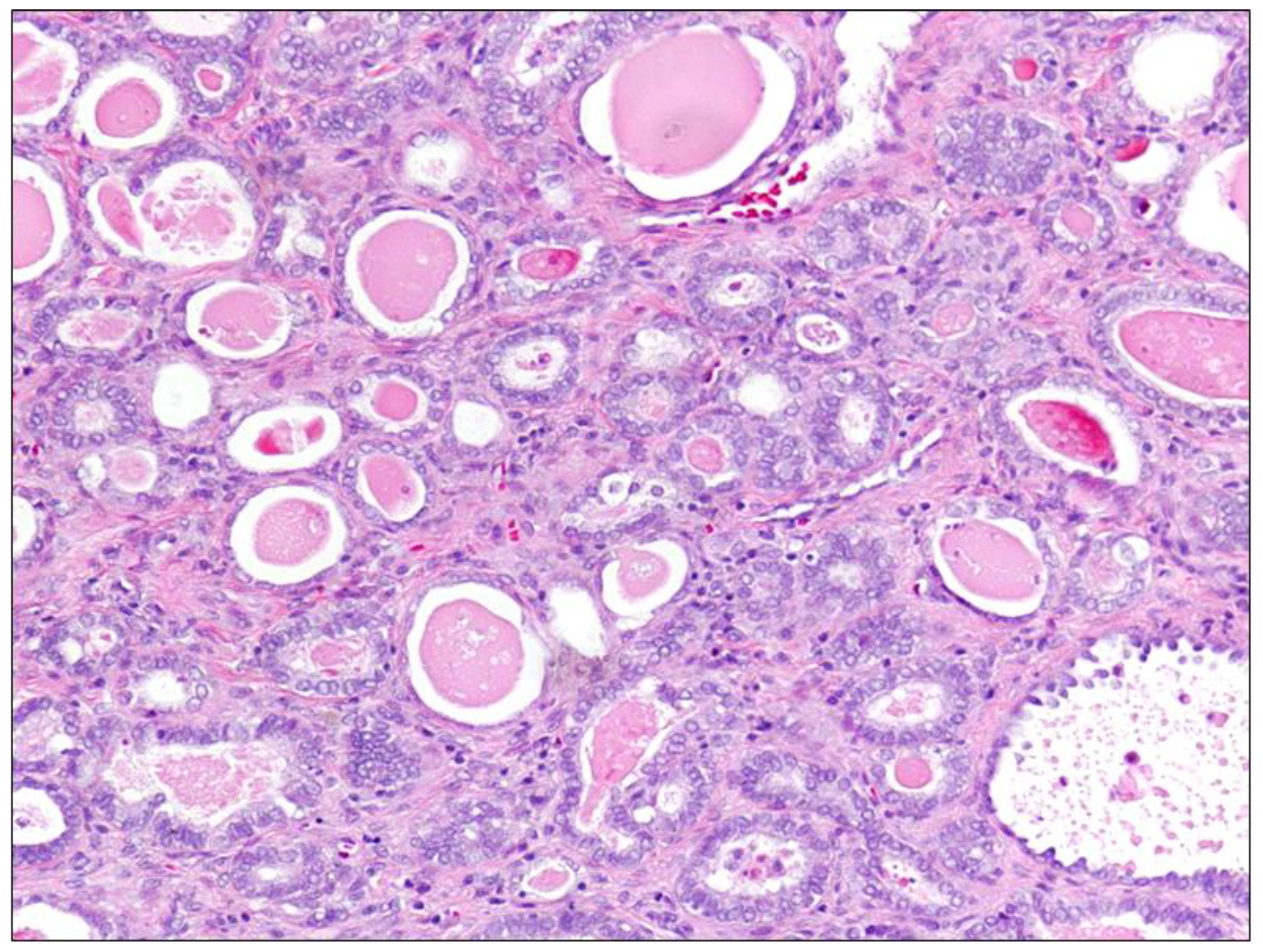
3.1.2. Mesonephric Endocervical ADC
3.1.3. Clear Cell Carcinoma
3.2. Other Adenocarcinomas of the Uterine Cervix: Serous, Endometrioid
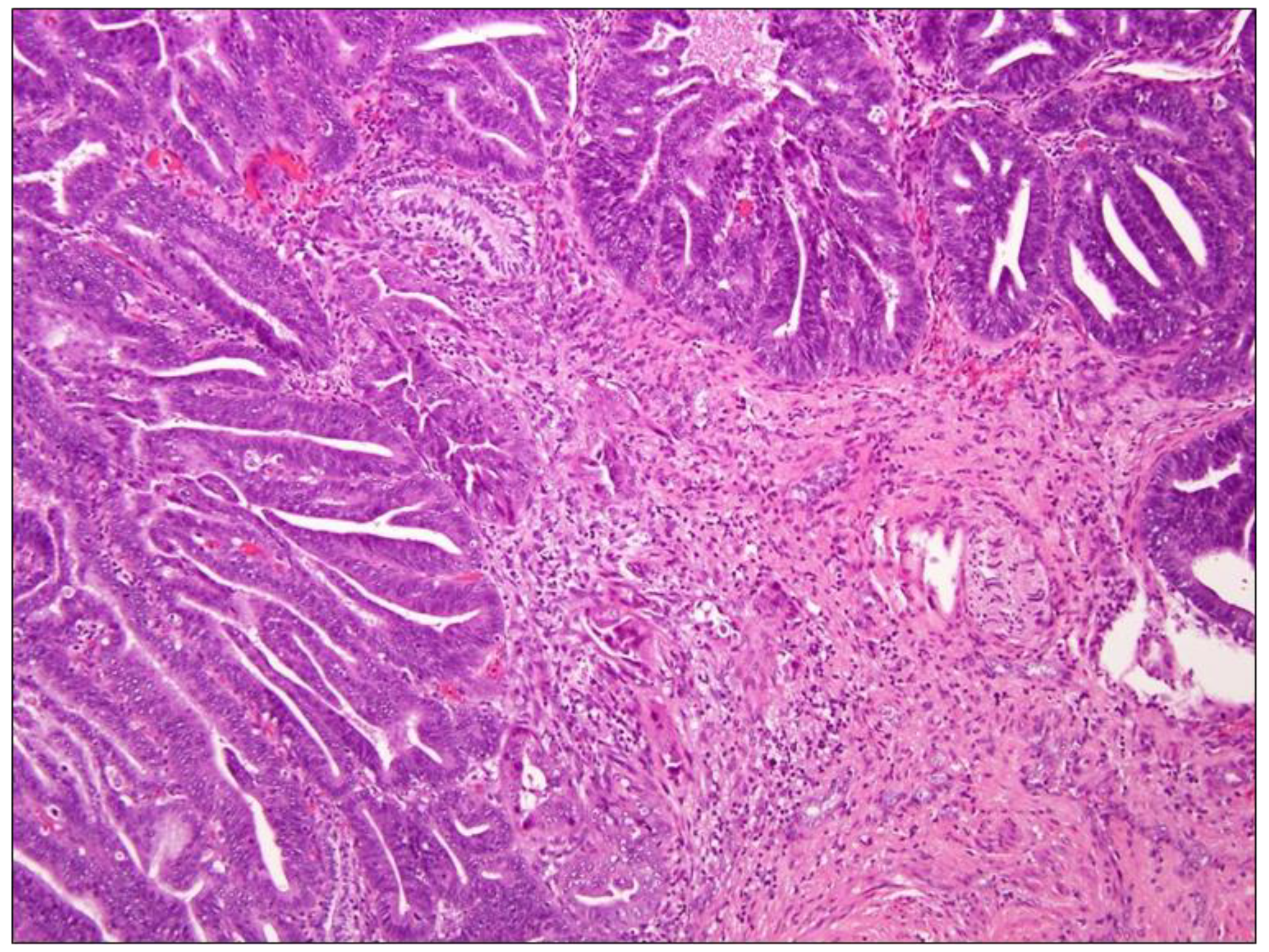
3.2.1. Endometrioid ADC
3.2.2. Serous Carcinoma
4. NHPVA Pathways
5. HPV Tests
5.1. Molecular Diagnostics
5.2. p16 Immunohistochemistry
5.3. Limitations of HPV Tests
5.4. False-Negative Tests
6. Treatment
7. Prognosis
Other Locations of HPV-Dependent and Independent Carcinomas
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Adegoke, O.; Kulasingam, S.; Virnig, B. Cervical Cancer Trends in the United States: A 35-Year Population-Based Analysis. J. Womens Health 2012, 21, 1031–1037. [Google Scholar] [CrossRef]
- Arbyn, M.; Weiderpass, E.; Bruni, L.; de Sanjosé, S.; Saraiya, M.; Ferlay, J.; Bray, F. Estimates of incidence and mortality of cervical cancer in 2018: A worldwide analysis. Lancet Glob. Health 2020, 8, e191–e203. [Google Scholar] [CrossRef] [Green Version]
- Chong, G.O.; Lee, Y.H.; Han, H.S.; Lee, H.J.; Park, J.Y.; Hong, D.G.; Cho, Y. L Prognostic value of pre-treatment human papilloma virus DNA status in cervical cancer. Gynecol. Oncol. 2018, 148, 97–102. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Carunchio, L.; Soveral, I.; Steenbergen, R.D.M.; Torné, A.; Martinez, S.; Fusté, P.; Pahisa, J.; Marimon, L.; Ordi, J.; Del Pino, M. HPV-negative carcinoma of the uterine cervix: A distinct type of cervical cancer with poor prognosis. BJOG 2014, 122, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Arezzo, F.; La Forgia, D.; Venerito, V.; Moschetta, M.; Tagliafico, A.S.; Lombardi, C.; Loizzi, V.; Cicinelli, E.; Cormio, G. A Machine Learning Tool to Predict the Response to Neoadjuvant Chemotherapy in Patients with Locally Advanced Cervical Cancer. Appl. Sci. 2021, 11, 823. [Google Scholar] [CrossRef]
- Park, K.J.; Kiyokawa, T.; Soslow, R.A.; Lamb, C.A.; Oliva, E.; Zivanovic, O.; Juretzka, M.M.; Pirog, E.C. Unusual endocervical adenocarcinomas: An immunohistochemical analysis with molecular detection of human papillomavirus. Am. J. Surg. Pathol. 2011, 35, 633–646. [Google Scholar] [CrossRef] [PubMed]
- Monsonego, J. Global challenges of cervical cancer prevention. Eur. J. Gynaecol. Oncol. 2000, 21, 533–539. [Google Scholar] [PubMed]
- De Martel, C.; Plummer, M.; Vignat, J.; Franceschi, S. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int. J. Cancer 2017, 141, 664–670. [Google Scholar] [CrossRef] [Green Version]
- Pirog, E.C. Cervical Adenocarcinoma: Diagnosis of Human Papillomavirus-Positive and Human Papillomavirus-Negative Tumors. Arch. Pathol. Lab. Med. 2017, 141, 1653–1667. [Google Scholar] [CrossRef] [Green Version]
- Holl, K.; Nowakowski, A.M.; Powell, N.; McCluggage, W.G.; Pirog, E.C.; Collas De Souza, S.; Tjalma, W.A.; Rosenlund, M.; Fiander, A.; Castro Sánchez, M.; et al. Human papillomavirus prevalence and type-distribution in cervical glandular neoplasias: Results from a European multinational epidemiological study. Int. J. Cancer 2015, 137, 2858–2868. [Google Scholar] [CrossRef] [Green Version]
- Stolnicu, S.; Barsan, I.; Hoang, L.; Patel, P.; Terinte, C.; Pesci, A.; Aviel-Ronen, S.; Kiyokawa, T.; Alvarado-Cabrero, I.; Pike, M.C.; et al. International Endocervical Adenocarcinoma Criteria and Classification (IECC): A New Pathogenetic Classification for Invasive Adenocarcinomas of the Endocervix. Am. J. Surg. Pathol. 2018, 42, 214–226. [Google Scholar] [CrossRef] [PubMed]
- Tjalma, W. HPV negative cervical cancers and primary HPV screening. Facts Views Vis. Obgyn 2018, 10, 107–113. [Google Scholar] [PubMed]
- De Sanjose, S.; Quint, W.G.; Alemany, L.; Geraets, D.T.; Klaustermeier, J.E.; Lloveras, B.; Tous, S.; Felix, A.; Bravo, L.E.; Shin, H.R.; et al. Human papillomavirus genotype attribution in invasive cervical cancer: A retrospective cross-sectional worldwide study. Lancet Oncol. 2010, 11, 1048–1056. [Google Scholar] [CrossRef]
- Pirog, E.C.; Lloveras, B.; Molijn, A.; Tous, S.; Guimera, N.; Alejo, M.; Clavero, O.; Klaustermeier, J.; Jenkins, D.; Quint, W.G.; et al. HPV prevalence and genotypes in different histological subtypes of cervical adenocarcinoma, a worldwide analysis of 760 cases. Mod. Pathol. 2014, 27, 1559–1567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersson, S.; Larson, B.; Hjerpe, A.; Silfversward, C.; Sallstrom, J.; Wilander, E.; Rylander, E. Adenocarcinoma of the uterine cervix: The presence of human papillomavirus and the method of detection. Acta Obstet. Gynecol. Scand. 2003, 82, 960–965. [Google Scholar] [CrossRef]
- Clifford, G.; Franceschi, S. Members of the human papillomavirus type 18 family (alpha-7 species) share a common association with adenocarcinoma of the cervix. Int. J. Cancer 2007, 122, 1684–1685. [Google Scholar] [CrossRef]
- Tornesello, M.L.; Losito, S.; Benincasa, G.; Fulciniti, F.; Botti, G.; Greggi, S.; Buonaguro, L.; Buonaguro, F. Human papillomavirus (HPV) genotypes and HPV16 variants and risk of adenocarcinoma and squamous cell carcinoma of the cervix. Gynecol. Oncol. 2011, 121, 32–42. [Google Scholar] [CrossRef]
- Mikami, Y.; Hata, S.; Melamed, J.; Fujiwara, K.; Manabe, T. Lobular endocervical glandular hyperplasia is a metaplastic process with a pyloric gland phenotype. Histopathology 2001, 39, 364–372. [Google Scholar] [CrossRef]
- McCluggage, W.G. New developments in endocervical glandular lesions. Histopathology 2012, 62, 138–160. [Google Scholar] [CrossRef]
- Cree, I.A.; White, V.A.; Indave, B.I.; Lokuhetty, D. Revising the WHO classification: Female genital tract tumours. Histopathology 2019, 76, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Carleton, C.; Hoang, L.; Sah, S.; Kiyokawa, T.; Karamurzin, Y.S.; Talia, K.L.; Park, K.J.; McCluggage, W.G. A Detailed Immunohistochemical Analysis of a Large Series of Cervical and Vaginal Gastric-type Adenocarcinomas. Am. J. Surg. Pathol. 2016, 40, 636–644. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikami, Y.; McCluggage, W.G. Endocervical glandular lesions exhibiting gastric differentiation: An emerging spectrum of benign, premalignant, and malignant lesions. Adv. Anat. Pathol. 2013, 20, 227–237. [Google Scholar] [CrossRef] [PubMed]
- Turashvili, G.; Morency, E.G.; Kracun, M.; DeLair, D.F.; Chiang, S.; Soslow, R.A.; Park, K.J.; Murali, R. Morphologic Features of Gastric-type Cervical Adenocarcinoma in Small Surgical and Cytology Specimens. Int. J. Gynecol. Pathol. 2019, 38, 263–275. [Google Scholar] [CrossRef] [PubMed]
- Kenny, S.L.; McBride, H.A.; Jamison, J.; McCluggage, W.G. Mesonephric adenocarcinomas of the uterine cervix and corpus: HPV-negative neoplasms that are commonly PAX8, CA125, and HMGA2 positive and that may be immunoreactive with TTF1 and hepatocyte nuclear factor 1-beta. Am. J. Surg. Pathol. 2012, 36, 799–807. [Google Scholar] [CrossRef]
- Pirog, E.C.; Kleter, B.; Olgac, S.; Bobkiewicz, P.; Lindeman, J.; Quint, W.G.; Richart, R.M.; Isacson, C. Prevalence of human papillomavirus DNA in different histological subtypes of cervical adenocarcinoma. Am. J. Pathol. 2000, 157, 1055–1062. [Google Scholar] [CrossRef] [Green Version]
- Seay, K.; Bustamante, B.; Khutti, S.; Frimer, M. A case of non-HPV related primary endometrioid adenocarcinoma of the cervix. Gynecol. Oncol. Rep. 2020, 32, 100579. [Google Scholar] [CrossRef]
- Park, K.J. Cervical adenocarcinoma: Integration of HPV status, pattern of invasion, morphology and molecular markers into classification. Histopathology 2019, 76, 112–127. [Google Scholar] [CrossRef]
- Barreto, C.L.; Martins, D.B.; de Lima Filho, J.L.; Magalhaes, V. Detection of human Papillomavirus in biopsies of patients with cervical cancer, and its association with prognosis. Arch. Gynecol. Obstet. 2013, 288, 643–648. [Google Scholar] [CrossRef]
- Tommasino, M.; Accardi, R.; Caldeira, S.; Dong, W.; Malanchi, I.; Smet, A.; Zehbe, I. The role of TP53 in Cervical carcinogenesis. Hum. Mutat. 2003, 21, 307–312. [Google Scholar] [CrossRef] [PubMed]
- Nicolás, I.; Marimon, L.; Barnadas, E.; Saco, A.; Rodríguez-Carunchio, L.; Fusté, P.; Martí, C.; Rodriguez-Trujillo, A.; Torne, A.; Del Pino, M.; et al. HPV-negative tumors of the uterine cervix. Mod. Pathol. 2019, 32, 1189–1196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ueno, S.; Sudo, T.; Oka, N.; Wakahashi, S.; Yamaguchi, S.; Fujiwara, K.; Mikami, Y.; Nishimura, R. Absence of human papillomavirus infection and activation of PI3K-AKT pathway in cervical clear cell carcinoma. Int. J. Gynecol. Cancer 2013, 23, 1084–1091. [Google Scholar] [CrossRef]
- Mirkovic, J.; Sholl, L.M.; Garcia, E.; I Lindeman, N.; E Macconaill, L.; Hirsch, M.S.; Cin, P.D.; Gorman, M.; A Barletta, J.; Nucci, M.R.; et al. Targeted genomic profiling reveals recurrent KRAS mutations and gain of chromosome 1q in mesonephric carcinomas of the female genital tract. Mod. Pathol. 2015, 28, 1504–1514. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meijer, C.J.; Berkhof, J.; Castle, P.E.; Hesselink, A.T.; Franco, E.L.; Ronco, G.; Arbyn, M.; Bosch, F.X.; Cuzick, J.; Dillner, J.; et al. Guidelines for human papillomavirus DNA test requirements for primary cervical cancer screening in women 30 years and older. Int. J. Cancer 2009, 124, 516–520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Poljak, M.; Cuzick, J.; Kocjan, B.J.; Iftner, T.; Dillner, J.; Arbyn, M. Nucleic acid tests for the detection of alpha human papillomaviruses. Vaccine 2012, 30 (Suppl. 5), F100–F106. [Google Scholar] [CrossRef]
- Villa, L.L.; Denny, L. CHAPTER 7 Methods for detection of HPV infection and its clinical utility. Int. J. Gynecol. Obstet. 2006, 94 (Suppl. 1), S71–S80. [Google Scholar] [CrossRef]
- Prigge, E.S.; Arbyn, M.; von Knebel Doeberitz, M.; Reuschenbach, M. Diagnostic accuracy of p16(INK4a) immunohistochemistry in oropharyngeal squamous cell carcinomas: A systematic review and meta-analysis. Int. J. Cancer 2017, 140, 1186–1198. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jordan, R.C.; Lingen, M.W.; Perez-Ordonez, B.; He, X.; Pickard, R.; Koluder, M.; Jiang, B.; Wakely, P.; Xiao, W.; Gillison, M.L. Validation of methods for oropharyngeal cancer HPV status determination in US cooperative group trials. Am. J. Surg. Pathol. 2012, 36, 945–954. [Google Scholar] [CrossRef] [PubMed]
- Walboomers, J.M.; Jacobs, M.V.; Manos, M.M.; Bosch, F.X.; Kummer, J.A.; Shah, K.V.; Snijders, P.J.; Peto, J.; Meijer, C.J.; Muñoz, N. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J. Pathol. 1999, 189, 12–19. [Google Scholar] [CrossRef]
- Tjalma, W.; Trinh, X.; Rosenlund, M.; Makar, A.; Kridelka, F.; Rosillon, D.; Van Dam, P.; De Souza, S.C.; Holl, K.; Simon, P.; et al. A cross-sectional, multicentre, epidemiological study on human papillomavirus (HPV) type distribution in adult women diagnosed with invasive cervical cancer in Belgium. Facts Views Vis. Obgyn 2015, 7, 101–108. [Google Scholar]
- Petry, K.U.; Liebrich, C.; Luyten, A.; Zander, M.; Iftner, T. Surgical staging identified false HPV-negative cases in a large series of invasive cervical cancers. Papillomavirus Res. 2017, 4, 85–89. [Google Scholar] [CrossRef]
- Kaliff, M.; Karlsson, M.G.; Sorbe, B.; Bohr Mordhorst, L.; Helenius, G.; Lillsunde-Larsson, G. HPV-negative Tumors in a Swedish Cohort of Cervical Cancer. Int. J. Gynecol. Pathol. 2020, 39, 279–288. [Google Scholar] [CrossRef] [PubMed]
- Arbyn, M.; Snijders, P.J.; Meijer, C.J.; Berkhof, J.; Cuschieri, K.; Kocjan, B.J.; Poljak, M. Which high-risk HPV assays fulfil criteria for use in primary cervical cancer screening? Clin. Microbiol. Infect. 2015, 21, 817–826. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rebolj, M.; Preisler, S.; Ejegod, D.M.; Rygaard, C.; Lynge, E.; Bonde, J. Disagreement between human papillomavirus assays: An unexpected challenge for the choice of an assay in primary cervical screening. PLoS ONE 2014, 9, e86835. [Google Scholar] [CrossRef] [PubMed]
- Snijders, P.J.; van den Brule, A.J.; Meijer, C.J. The clinical relevance of human papillomavirus testing: Relationship between analytical and clinical sensitivity. J. Pathol. 2003, 201, 1–6. [Google Scholar] [CrossRef]
- Rebolj, M.; Bonde, J.; Ejegod, D.; Preisler, S.; Rygaard, C.; Lynge, E. A daunting challenge: Human Papillomavirus assays and cytology in primary cervical screening of women below age 30years. Eur. J. Cancer 2015, 51, 1456–1466. [Google Scholar] [CrossRef] [Green Version]
- De Thurah, L.; Bonde, J.; Lam, J.U.H.; Rebolj, M. Concordant testing results between various human papillomavirus assays in primary cervical cancer screening: Systematic review. Clin. Microbiol. Infect. 2018, 24, 29–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jedpiyawongse, A.; Homcha-em, P.; Karalak, A.; Srivatanakul, P. Immunohistochemical overexpression of p16 protein associated with cervical cancer in Thailand. Asian Pac. J. Cancer Prev. 2008, 9, 625–630. [Google Scholar] [PubMed]
- Alos, L.; Moyano, S.; Nadal, A.; Alobid, I.; Blanch, J.L.; Ayala, E.; Lloveras, B.; Quint, W.; Cardesa, A.; Ordi, J. Human papillomaviruses are identified in a subgroup of sinonasal squamous cell carcinomas with favorable outcome. Cancer 2009, 115, 2701–2709. [Google Scholar] [CrossRef]
- Larque, A.B.; Hakim, S.; Ordi, J.; Nadal, A.; Diaz, A.; Del Pino, M.; Marimon, L.; Alobid, I.; Cardesa, A.; Alos, L. High-risk human papillomavirus is transcriptionally active in a subset of sinonasal squamous cell carcinomas. Mod. Pathol. 2013, 27, 343–351. [Google Scholar] [CrossRef]
- Sheng, Z.; Minato, H.; Sasagawa, T.; Nakada, S.; Kinoshita, E.; Kurose, N.; Nojima, T.; Makinoda, S. Detection of high-risk human papillomavirus subtypes in cervical glandular neoplasia by in situ hybridization. Int. J. Clin. Exp. Pathol. 2013, 6, 2168–2177. [Google Scholar]
- Evans, M.F.; Matthews, A.; Kandil, D.; Adamson, C.S.; Trotman, W.E.; Cooper, K. Discrimination of ‘driver’ and ‘passenger’ HPV in tonsillar carcinomas by the polymerase chain reaction, chromogenic in situ hybridization, and p16(INK4a) immunohistochemistry. Head Neck Pathol. 2011, 5, 344–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ren, H.; Pors, J.; Chow, C.; Ta, M.; Stolnicu, S.; Soslow, R.; Huntsman, D.; Hoang, L. Evaluation of human papillomavirus (HPV) prediction using the International Endocervical Adenocarcinoma Criteria and Classification system, compared to p16 immunohistochemistry and HPV RNA in-situ hybridization. J. Pathol. Transl. Med. 2020, 54, 480–488. [Google Scholar] [CrossRef] [PubMed]
- Alemany, L.; Pérez, C.; Tous, S.; Llombart-Bosch, A.; Lloveras, B.; Lerma, E.; Guarch, R.; Andújar, M.; Pelayo, A.; Alejo, M.; et al. Human papillomavirus genotype distribution in cervical cancer cases in Spain. Implications for prevention. Gynecol. Oncol. 2012, 124, 512–517. [Google Scholar] [CrossRef]
- Baay, M.F.D.; Tjalma, W.A.A.; Weyler, J.; Goovaerts, G.; Buytaert, P.; Van Marck, E.A.E.; Lardon, F.; Vermorken, J.B.l. Human papillomavirus infection in the female population of Antwerp, Belgium: Prevalence in healthy women, women with premalignant lesions and cervical cancer. Eur. J. Gynaecol. Oncol. 2001, 22, 204–208. [Google Scholar] [CrossRef]
- Igidbashian, S.; Schettino, M.T.; Boveri, S.; Barberis, M.; Sandri, M.T.; Carinelli, S.; Cannone, M.; Sideri, M. Tissue genotyping of 37 in situ and invasive cervical cancer with a concomitant negative HC2 HPV DNA test. J. Low. Genit. Tract Dis. 2014, 18, 87–91. [Google Scholar] [CrossRef]
- Del Pino, M.; Rodriguez-Carunchio, L.; Alonso, I.; Torne, A.; Rodriguez, A.; Fuste, P.; Castillo, P.; Nonell, R.; Abu-Lhiga, N.; Ordi, J. Clinical, colposcopic and pathological characteristics of cervical and vaginal high-grade lesions negative for HPV by Hybrid Capture 2. Gynecol. Oncol. 2011, 122, 515–520. [Google Scholar] [CrossRef] [PubMed]
- Marth, C.; Landoni, F.; Mahner, S.; McCormack, M.; Gonzalez-Martin, A.; Colombo, N. Cervical cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2017, 28 (Suppl. 4), iv72–iv83. [Google Scholar] [CrossRef] [PubMed]
- Landoni, F.; Maneo, A.; Cormio, G.; Perego, P.; Milani, R.; Caruso, O.; Mangioni, C. Class II versus class III radical hysterectomy in stage IB-IIA cervical cancer: A prospective randomized study. Gynecol. Oncol. 2001, 80, 3–12. [Google Scholar] [CrossRef]
- Chai, Y.; Wang, T.; Wang, J.; Yang, Y.; Gao, Y.; Gao, J.; Gao, S.; Wang, Y.; Zhou, X.; Liu, Z. Radical hysterectomy with adjuvant radiotherapy versus radical radiotherapy for FIGO stage IIB cervical cancer. BMC Cancer 2014, 14, 63. [Google Scholar] [CrossRef] [Green Version]
- Fischerova, D.; Cibula, D. The role of ultrasound in primary workup of cervical cancer staging (ESGO, ESTRO, ESP cervical cancer guidelines). Ceska Gynekol. 2019, 84, 40–48. [Google Scholar]
- Loizzi, V.; Cormio, G.; Vicino, M.; Selvaggi, L. Neoadjuvant chemotherapy: An alternative option of treatment for locally advanced cervical cancer. Gynecol. Obstet. Investig. 2008, 65, 96–103. [Google Scholar] [CrossRef] [PubMed]
- Loizzi, V.; Del Vecchio, V.; Crupano, F.M.; Minicucci, V.; Fumarulo, V.V.; Resta, L.; Vimercati, A.; Bettocchi, S.; Cicinelli, E.; Cormio, G. A phase II study: Dose-dense carboplatin and paclitaxel as neoadjuvant chemotherapy in locally advanced cervical cancer. J. Chemother. 2018, 30, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Selvaggi, L.; Loizzi, V.; Di Gilio, A.R.; Nardelli, C.; Cantatore, C.; Cormio, G. Neoadjuvant chemotherapy in cervical cancer: A 67 patients experience. NT J. Gynecol. Cancer 2006, 16, 631–637. [Google Scholar] [CrossRef]
- Shimada, M.; Tokunaga, H.; Kigawa, J.; Yaegashi, N. Impact of Histopathological Risk Factors on the Treatment of Stage IB-IIB Uterine Cervical Cancer. Ohoku J. Exp. Med. 2020, 252, 339–351. [Google Scholar] [CrossRef]
- Tao, X.; Zheng, B.; Yin, F.; Zeng, Z.; Li, Z.; Griffith, C.C.; Luo, B.; Ding, X.; Zhou, X.; Zhao, C. Polymerase Chain Reaction Human Papillomavirus (HPV) Detection and HPV Genotyping in Invasive Cervical Cancers with Prior Negative HC2 Test Results. Am. J. Clin. Pathol. 2017, 147, 477–483. [Google Scholar] [CrossRef] [Green Version]
- Zampronha, R.D.A.C.; Freitas-Junior, R.; Murta, E.F.C.; Michelin, M.A.; Barbaresco, A.A.; Adad, S.J.; de Oliveira, A.M.; Rassi, A.B.; Oton, G.J.B. Human papillomavirus types 16 and 18 and the prognosis of patients with stage I cervical cancer. Clinics 2013, 68, 809–814. [Google Scholar] [CrossRef]
- Pilch, H.; Gunzel, S.; Schaffer, U.; Tanner, B.; Brockerhoff, P.; Maeurer, M.; Hockel, M.; Hommel, G.; Knapstein, P.G. The presence of HPV DNA in cervical cancer: Correlation with clinico-pathologic parameters and prognostic significance: 10 years experience at the Department of Obstetrics and Gynecology of the Mainz University. Int. J. Gynecol. Cancer 2001, 11, 39–48. [Google Scholar] [CrossRef]
- Feng, D.; Xu, H.; Li, X.; Wei, Y.; Jiang, H.; Xu, H.; Luo, A.; Zhou, F. An association analysis between mitochondrial DNA content, G10398A polymorphism, HPV infection, and the prognosis of cervical cancer in the Chinese Han population. Tumor Biol. 2015, 37, 5599–5607. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Tan, Y.; Zhu, L.-X.; Zhou, L.-N.; Zeng, P.; Liu, Q.; Chen, M.-B.; Tian, Y. Prognostic value of HPV DNA status in cervical cancer before treatment: A systematic review and meta-analysis. Oncotarget 2017, 8, 66352–66359. [Google Scholar] [CrossRef] [Green Version]
- Alonso, I.; Felix, A.; Torné, A.; Fusté, V.; del Pino, M.; Castillo, P.; Balasch, J.; Pahisa, J.; Rios, J.; Ordi, J. Human papillomavirus as a favorable prognostic biomarker in squamous cell carcinomas of the vagina. Gynecol. Oncol. 2012, 125, 194–199. [Google Scholar] [CrossRef]
- Higgins, G.D.; Davy, M.; Roder, D.; Uzelin, D.M.; Phillips, G.E.; Burrell, C.J. Increased age and mortality associated with cervical carcinomas negative for human papillomavirus RNA. Lancet 1991, 338, 910–913. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| HPVA | NHPVA |
|---|---|
| Usual-type | Endometrioid adenocarcinoma |
| Villoglandular | Gastric-type adenocarcinoma |
| Mucinous | Serous carcinoma |
| Mucinous, intestinal type | Clear cell adenocarcinoma |
| Mucinous, signet ring cell type | Mesonephric carcinoma |
| Invasive stratified mucin-producting carcinoma (iSMILE) | Invasive adenocarcinoma NOS |
| Histotypes | % HPV Positive |
|---|---|
| SCC | 100 |
| ADS | up to 86 |
| ADC | |
| Usual type | 80–100 |
| Mucinous, Intestinal type | 83–100 |
| Villoglandular | 100 |
| Mucinous, signet ring cell type | 100 |
| Endometrioid | 0 |
| Gastric Type | 0 |
| Masonephric | 0 |
| Clear cell | 28 |
| Serous | 30 |
| Tecnique | Advantages | Disadvantages | |
|---|---|---|---|
| Hybrid Capture 2 (HC2) [34] | DNA hybrids are identified with RNA probes (13 types of HR-HPV: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68) | High sensitivity and high negative predictive value. Tests can be processed manually, semi-automatically, or be automated through use of a robot. | Lower specificity and cross-reactions with low-risk probes. This test cannot identify the HPV type or whether one or more HPV types are present (not designed to give a quantitative result). |
| Polymerase Chain Reaction (PCR) [35,36] | Different primer sets have been designed, targeting region L1 and enabling to differentiate, through specific probes, the most frequent types of high-, intermediate-, and low-risk HPV, plate hybridization of the biotinylated products previously amplified by PCR. | Very sensitive with a detection level down to one viral copy. | Susceptible to contamination. |
| Author | Year | CC Population | Type of HPV Test | Prevalence of NHPVA | Re-Analysed Cases | Type of HPV Test for Re-Analysis | Prevalence of NHPVA after Re-Analysis |
|---|---|---|---|---|---|---|---|
| Walboomers et al. [38] | 1999 | 932 | PCR | 66 (7.1%) | 55/66 | PCR | 38 (4.1%) |
| de Sanjose et al. [13] | 2010 | 10575 | PCR | 1586 (15%) | - | - | - |
| Rodriguez-Carunchio et al. [4] | 2015 | 1333 | ISH | 136 (10.2%) | 136/136 | PCR | 8 (0.6%) |
| Tjalma et al. [39] | 2015 | 255 | mix of different HPV tests * | 18 (7.1%) | - | - | - |
| Stolnicu et al. [11] | 2017 | 370 | ISH | 55 (14.8%) | - | - | - |
| Petry et al. [40] | 2017 | 350 | ISH | 10 (2.8%) | 10/10 | PCR | 1 (0.3%) |
| Tjalma et al. [12] | 2018 | 136 | mix of different HPV tests * | 20 (15%) | - | - | - |
| Nicolás et al. [30] | 2019 | 214 | PCR | 21 (10%) | - | - | - |
| Kaliff et al. [41] | 2020 | 209 | PCR | 37 (17.7%) | 37/37 | PCR | 20 (10%) |
| Author | Year | n. of NHPVA | Stage I | Stage II | Stage III | Stage IV |
|---|---|---|---|---|---|---|
| Stolnicu et al. [11] | 2017 | 55 | 29 (52%) | 23 (42%) | 3 (6%) | |
| Kaliff et al. [41] | 2020 | 37 | 10 (27%) | 19 (51%) | 4 (11%) | 4 (11%) |
| Early Stage (IA-IB1) | Advanced Stage (IB2-IV) | |||||
| Rodriguez-Carunchio et al. [4] | 2015 | 8 | 1 (12.5%) | 7 (87.5%) | ||
| Nicolás et al. [30] | 2019 | 21 | 2 (10%) | 19 (90%) |
| Author | Year | DFS NHPVA (Months) | DFS HPVA (Months) | OS NHPVA (Months) | OS HPVA (Months) |
|---|---|---|---|---|---|
| Rodriguez-Carunchio et al. [4] | 2015 | 51.9 (95% CI 12.2–91.7) | 109.9 (95% CI 98.2–121.5) | 67.7 (95% CI 20.0–106.9) | 108.9 (95% CI 97.7–120.0) |
| Nicolás et al. [30] | 2018 | 59.8 (95% CI 32.0–87.6) | 132.2 (95% CI 118.6–145.8) | 77.0 (95% CI 47.2–106.8) | 153.8 (95% CI 142.0–165.6) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arezzo, F.; Cormio, G.; Loizzi, V.; Cazzato, G.; Cataldo, V.; Lombardi, C.; Ingravallo, G.; Resta, L.; Cicinelli, E. HPV-Negative Cervical Cancer: A Narrative Review. Diagnostics 2021, 11, 952. https://doi.org/10.3390/diagnostics11060952
Arezzo F, Cormio G, Loizzi V, Cazzato G, Cataldo V, Lombardi C, Ingravallo G, Resta L, Cicinelli E. HPV-Negative Cervical Cancer: A Narrative Review. Diagnostics. 2021; 11(6):952. https://doi.org/10.3390/diagnostics11060952
Chicago/Turabian StyleArezzo, Francesca, Gennaro Cormio, Vera Loizzi, Gerardo Cazzato, Viviana Cataldo, Claudio Lombardi, Giuseppe Ingravallo, Leonardo Resta, and Ettore Cicinelli. 2021. "HPV-Negative Cervical Cancer: A Narrative Review" Diagnostics 11, no. 6: 952. https://doi.org/10.3390/diagnostics11060952