
Current Status and Future Perspectives of Perioperative Therapy for Resectable Biliary Tract Cancer: A Multidisciplinary Review

 , , , , ,
, , , , ,
Abstract
:Simple Summary
Abstract
1. Introduction
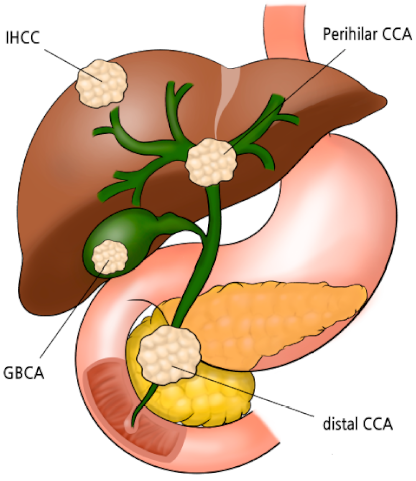
2. Surgical Considerations
2.1. IH-CCA
2.2. GBCA
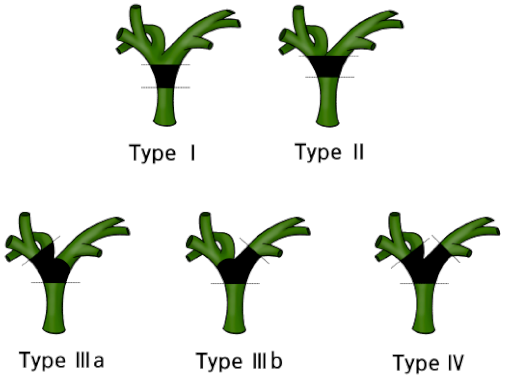
2.3. Perihilar CCA
2.4. Distal CCA
3. Clinical Outcomes and Recurrence Patterns among Patients with Resected BTC
4. Adjuvant Chemotherapy
4.1. Meta-Analysis
4.2. Randomized Trials
4.2.1. BILCAP Trial
4.2.2. PRODIGE 12 Trial
4.2.3. BCAT Trial
4.3. Interpretation of Conflicting Results and Future Perspectives
4.4. Ongoing Adjuvant Chemotherapy Trials
5. Neoadjuvant Chemotherapy
6. Adjuvant Radiation Therapy
7. Endpoints of Perioperative Therapy Clinical Trials
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Banales, J.M.; Marin, J.J.G.; Lamarca, A.; Rodrigues, P.M.; Khan, S.A.; Roberts, L.R.; Cardinale, V.; Carpino, G.; Andersen, J.B.; Braconi, C.; et al. Cholangiocarcinoma 2020: The next horizon in mechanisms and management. Nat. Rev. Gastroenterol. Hepatol. 2020, 17, 577–588. [Google Scholar] [CrossRef] [PubMed]
- Jung, K.-W.; Won, Y.-J.; Hong, S.; Kong, H.-J.; Lee, E.S. Prediction of Cancer Incidence and Mortality in Korea, 2020. Cancer Res. Treat. 2020, 52, 351–358. [Google Scholar] [CrossRef]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef]
- Valle, J.; Wasan, H.; Palmer, D.H.; Cunningham, D.; Anthoney, A.; Maraveyas, A.; Madhusudan, S.; Iveson, T.; Hughes, S.; Pereira, S.P.; et al. Cisplatin plus Gemcitabine versus Gemcitabine for Biliary Tract Cancer. N. Engl. J. Med. 2010, 362, 1273–1281. [Google Scholar] [CrossRef] [Green Version]
- Park, J.O.; Oh, D.-Y.; Hsu, C.; Chen, J.-S.; Chen, L.-T.; Orlando, M.; Kim, J.S.; Lim, H.Y. Gemcitabine Plus Cisplatin for Advanced Biliary Tract Cancer: A Systematic Review. Cancer Res. Treat. 2015, 47, 343–361. [Google Scholar] [CrossRef]
- Kim, B.J.; Hyung, J.; Yoo, C.; Park, S.-J.; Lee, S.S.; Song, T.J.; Seo, D.W.; Cho, H.; Ryoo, B.-Y.; Chang, H.-M. Prognostic factors in patients with advanced biliary tract cancer treated with first-line gemcitabine plus cisplatin: Retrospective analysis of 740 patients. Cancer Chemother. Pharmacol. 2017, 80, 209–215. [Google Scholar] [CrossRef] [PubMed]
- Okusaka, T.; Nakachi, K.; Fukutomi, A.; Mizuno, N.; Ohkawa, S.; Funakoshi, A.; Nagino, M.; Kondo, S.; Nagaoka, S.; Funai, J.; et al. Gemcitabine alone or in combination with cisplatin in patients with biliary tract cancer: A comparative multicentre study in Japan. Br. J. Cancer 2010, 103, 469–474. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, B.J.; Yoo, C.; Kim, K.-P.; Hyung, J.; Park, S.J.; Ryoo, B.-Y.; Chang, H.-M. Efficacy of fluoropyrimidine-based chemotherapy in patients with advanced biliary tract cancer after failure of gemcitabine plus cisplatin: Retrospective analysis of 321 patients. Br. J. Cancer 2017, 116, 561–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Abou-Alfa, G.K.; Macarulla, T.; Javle, M.M.; Kelley, R.K.; Lubner, S.J.; Adeva, J.; Cleary, J.M.; Catenacci, D.V.; Borad, M.J.; Bridgewater, J.; et al. Ivosidenib in IDH1-mutant, chemotherapy-refractory cholangiocarcinoma (ClarIDHy): A multicentre, randomised, double-blind, placebo-controlled, phase 3 study. Lancet Oncol. 2020, 21, 796–807. [Google Scholar] [CrossRef]
- Abou-Alfa, G.K.; Sahai, V.; Hollebecque, A.; Vaccaro, G.; Melisi, D.; Al-Rajabi, R.; Paulson, A.S.; Borad, M.J.; Gallinson, D.; Murphy, A.G.; et al. Pemigatinib for previously treated, locally advanced or metastatic cholangiocarcinoma: A multicentre, open-label, phase 2 study. Lancet Oncol. 2020, 21, 671–684. [Google Scholar] [CrossRef]
- Jeong, H.; Jeong, J.H.; Kim, K.-P.; Lee, S.S.; Oh, D.W.; Park, D.H.; Song, T.J.; Park, Y.; Hong, S.-M.; Ryoo, B.-Y.; et al. Feasibility of HER2-Targeted Therapy in Advanced Biliary Tract Cancer: A Prospective Pilot Study of Trastuzumab Biosimilar in Combination with Gemcitabine Plus Cisplatin. Cancers 2021, 13, 161. [Google Scholar] [CrossRef]
- Lamarca, A.; Barriuso, J.; McNamara, M.G.; Valle, J.W. Molecular targeted therapies: Ready for “prime time” in biliary tract cancer. J. Hepatol. 2020, 73, 170–185. [Google Scholar] [CrossRef] [Green Version]
- Primrose, J.N.; Fox, R.P.; Palmer, D.H.; Malik, H.Z.; Prasad, R.; Mirza, D.; Anthony, A.; Corrie, P.; Falk, S.; Finch-Jones, M.; et al. Capecitabine compared with observation in resected biliary tract cancer (BILCAP): A randomised, controlled, multicentre, phase 3 study. Lancet Oncol. 2019, 20, 663–673. [Google Scholar] [CrossRef] [Green Version]
- Edeline, J.; Benabdelghani, M.; Bertaut, A.; Watelet, J.; Hammel, P.; Joly, J.-P.; Boudjema, K.; Fartoux, L.; Bouhier-Leporrier, K.; Jouve, J.-L.; et al. Gemcitabine and Oxaliplatin Chemotherapy or Surveillance in Resected Biliary Tract Cancer (PRODIGE 12-ACCORD 18-UNICANCER GI): A Randomized Phase III Study. J. Clin. Oncol. 2019, 37, 658–667. [Google Scholar] [CrossRef] [PubMed]
- Ebata, T.; Hirano, S.; Konishi, M.; Uesaka, K.; Tsuchiya, Y.; Ohtsuka, M.; Kaneoka, Y.; Yamamoto, M.; Ambo, Y.; Shimizu, Y.; et al. Randomized clinical trial of adjuvant gemcitabine chemotherapy versus observation in resected bile duct cancer. BJS 2018, 105, 192–202. [Google Scholar] [CrossRef]
- Si, A.; Li, J.; Yang, Z.; Xia, Y.; Yang, T.; Lei, Z.; Cheng, Z.; Pawlik, T.M.; Lau, W.Y.; Shen, F. Impact of Anatomical Versus Non-anatomical Liver Resection on Short- and Long-Term Outcomes for Patients with Intrahepatic Cholangiocarcinoma. Ann. Surg. Oncol. 2019, 26, 1841–1850. [Google Scholar] [CrossRef]
- Zhang, X.-F.; Bagante, F.; Chakedis, J.; Moris, D.; Beal, E.W.; Weiss, M.; Popescu, I.; Marques, H.P.; Aldrighetti, L.; Maithel, S.K.; et al. Perioperative and Long-Term Outcome for Intrahepatic Cholangiocarcinoma: Impact of Major Versus Minor Hepatectomy. J. Gastrointest. Surg. 2017, 21, 1841–1850. [Google Scholar] [CrossRef]
- De Jong, M.C.; Nathan, H.; Sotiropoulos, G.C.; Paul, A.; Alexandrescu, S.; Marques, H.; Pulitano, C.; Barroso, E.; Clary, B.M.; Aldrighetti, L.; et al. Intrahepatic Cholangiocarcinoma: An International Multi-Institutional Analysis of Prognostic Factors and Lymph Node Assessment. J. Clin. Oncol. 2011, 29, 3140–3145. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- DeOliveira, M.L.; Cunningham, S.C.; Cameron, J.L.; Kamangar, F.; Winter, J.M.; Lillemoe, K.D.; Choti, M.A.; Yeo, C.J.; Schulick, R.D. Cholangiocarcinoma. Ann. Surg. 2007, 245, 755–762. [Google Scholar] [CrossRef] [PubMed]
- Bagante, F.; Gani, F.; Spolverato, G.; Xu, L.; Alexandrescu, S.; Marques, H.P.; Lamelas, J.; Aldrighetti, L.; Gamblin, T.C.; Maithel, S.K.; et al. Intrahepatic Cholangiocarcinoma: Prognosis of Patients Who Did Not Undergo Lymphadenectomy. J. Am. Coll. Surg. 2015, 221, 1031–1040.e4. [Google Scholar] [CrossRef]
- Shimada, M.; Yamashita, Y.; Aishima, S.; Shirabe, K.; Takenaka, K.; Sugimachi, K. Value of lymph node dissection during resection of intrahepatic cholangiocarcinoma. BJS 2001, 88, 1463–1466. [Google Scholar] [CrossRef]
- Zhang, X.; Chakedis, J.; Bagante, F.; Chen, Q.; Beal, E.W.; Lv, Y.; Weiss, M.; Popescu, I.; Marques, H.P.; Aldrighetti, L.; et al. Trends in use of lymphadenectomy in surgery with curative intent for intrahepatic cholangiocarcinoma. BJS 2018, 105, 857–866. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.J.; Chun, Y.S. Intrahepatic cholangiocarcinoma: The AJCC/UICC 8th edition updates. Chin. Clin. Oncol. 2018, 7, 52. [Google Scholar] [CrossRef] [PubMed]
- Okami, J.; Dono, K.; Sakon, M.; Tsujie, M.; Hayashi, N.; Fujiwara, Y.; Nagano, H.; Umeshita, K.; Nakamori, S.; Monden, M. Patterns of regional lymph node involvement in intrahepatic cholangiocarcinoma of the left lobe. J. Gastrointest. Surg. 2003, 7, 850–856. [Google Scholar] [CrossRef]
- Zhang, X.-F.; Xue, F.; Dong, D.-H.; Weiss, M.; Popescu, I.; Marques, H.P.; Aldrighetti, L.; Maithel, S.K.; Pulitano, C.; Bauer, T.W.; et al. Number and Station of Lymph Node Metastasis After Curative-intent Resection of Intrahepatic Cholangiocarcinoma Impact Prognosis. Ann. Surg. 2020. [Google Scholar] [CrossRef]
- FuksJean, D.; Regimbeau, J.M.; Le Treut, Y.-P.; Bachellier, P.; Raventos, A.; Pruvot, F.-R.; Chiche, L.; Farges, O. Incidental Gallbladder Cancer by the AFC-GBC-2009 Study Group. World J. Surg. 2011, 35, 1887–1897. [Google Scholar] [CrossRef]
- Lee, S.E.; Korean Pancreas Surgery Club; Jang, J.-Y.; Kim, S.-W.; Han, H.-S.; Kim, H.-J.; Yun, S.-S.; Cho, B.-H.; Yu, H.C.; Lee, W.J.; et al. Surgical Strategy for T1 Gallbladder Cancer: A Nationwide Multicenter Survey in South Korea. Ann. Surg. Oncol. 2014, 21, 3654–3660. [Google Scholar] [CrossRef]
- Lee, H.; Choi, D.W.; Park, J.Y.; Youn, S.; Kwon, W.; Heo, J.S.; Choi, S.H.; Jang, K.-T. Surgical Strategy for T2 Gallbladder Cancer According to Tumor Location. Ann. Surg. Oncol. 2014, 22, 2779–2786. [Google Scholar] [CrossRef] [PubMed]
- Abramson, M.A.; Pandharipande, P.; Ruan, D.; Gold, J.S.; Whang, E.E. Radical resection for T1b gallbladder cancer: A decision analysis. HPB 2009, 11, 656–663. [Google Scholar] [CrossRef] [Green Version]
- Kim, H.S.; Park, J.W.; Kim, H.; Han, Y.; Kwon, W.; Kim, S.-W.; Hwang, Y.J.; Kim, S.G.; Kwon, H.J.; Vinuela, E.; et al. Optimal surgical treatment in patients with T1b gallbladder cancer: An international multicenter study. J. Hepato Biliary Pancreat. Sci. 2018, 25, 533–543. [Google Scholar] [CrossRef]
- Kim, N.H.; Kim, S.H.; Choi, G.H.; Kang, C.M.; Kim, K.S.; Choi, J.S.; Lee, W.J. Role of Cholecystectomy and Lymph Node Dissection in Patients with T2 Gallbladder Cancer. World J. Surg. 2013, 37, 2635–2640. [Google Scholar] [CrossRef]
- D’Angelica, M.; Dalal, K.M.; DeMatteo, R.P.; Fong, Y.; Blumgart, L.H.; Jarnagin, W.R. Analysis of the Extent of Resection for Adenocarcinoma of the Gallbladder. Ann. Surg. Oncol. 2008, 16, 806–816. [Google Scholar] [CrossRef] [PubMed]
- Mizumoto, R.; Suzuki, H. Surgical anatomy of the hepatic hilum with special reference to the caudate lobe. World J. Surg. 1988, 12, 2–10. [Google Scholar] [CrossRef]
- Lee, S.G.; Song, G.W.; Hwang, S.; Ha, T.Y.; Moon, D.B.; Jung, D.H.; Kim, K.H.; Ahn, C.S.; Kim, M.H.; Sung, K.B.; et al. Surgical treatment of hilar cholangiocarcinoma in the new era: The Asan experience. J. Hepato Biliary Pancreat. Sci. 2010, 17, 476–489. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, H.; Kimura, F.; Yoshidome, H.; Ohtsuka, M.; Kato, A.; Yoshitomi, H.; Furukawa, K.; Miyazaki, M. Aggressive Surgical Resection for Hilar Cholangiocarcinoma of the Left-Side Predominance. Ann. Surg. 2010, 251, 281–286. [Google Scholar] [CrossRef] [PubMed]
- Ito, F.; Cho, C.S.; Rikkers, L.F.; Weber, S.M. Hilar Cholangiocarcinoma: Current Management. Ann. Surg. 2009, 250, 210–218. [Google Scholar] [CrossRef] [PubMed]
- Ikeyama, T.; Nagino, M.; Oda, K.; Ebata, T.; Nishio, H.; Nimura, Y. Surgical Approach to Bismuth Type I and II Hilar Cholangiocarcinomas. Ann. Surg. 2007, 246, 1052–1057. [Google Scholar] [CrossRef]
- Nagino, M.; Kamiya, J.; Arai, T.; Nishio, H.; Ebata, T.; Nimura, Y. “Anatomic” Right Hepatic Trisectionectomy (Extended Right Hepatectomy) With Caudate Lobectomy for Hilar Cholangiocarcinoma. Ann. Surg. 2006, 243, 28–32. [Google Scholar] [CrossRef]
- Makuuchi, M.; Thai, B.L.; Takayasu, K.; Takayama, T.; Kosuge, T.; Gunvén, P.; Yamazaki, S.; Hasegawa, H.; Ozaki, H. Preoperative portal embolization to increase safety of major hepatectomy for hilar bile duct carcinoma: A preliminary report. Surgery 1990, 107, 521–527. [Google Scholar]
- Ribero, D.; Abdalla, E.K.; Madoff, D.C.; Donadon, M.; Loyer, E.M.; Vauthey, J.-N. Portal vein embolization before major hepatectomy and its effects on regeneration, resectability and outcome. BJS 2007, 94, 1386–1394. [Google Scholar] [CrossRef] [Green Version]
- Farges, O.; Belghiti, J.; Kianmanesh, R.; Regimbeau, J.M.; Santoro, R.; Vilgrain, V.; Denys, A.; Sauvanet, A. Portal Vein Embolization Before Right Hepatectomy. Ann. Surg. 2003, 237, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Hemming, A.W.; Reed, A.I.; Howard, R.J.; Fujita, S.; Hochwald, S.N.; Caridi, J.G.; Hawkins, I.F.; Vauthey, J.-N. Preoperative Portal Vein Embolization for Extended Hepatectomy. Ann. Surg. 2003, 237, 686–693. [Google Scholar] [CrossRef]
- Tran, K.T.C.; Smeenk, H.G.; van Eijck, C.H.J.; Kazemier, G.; Hop, W.C.; Greve, J.W.G.; Terpstra, O.T.; Zijlstra, J.A.; Klinkert, P.; Jeekel, H. Pylorus Preserving Pancreaticoduodenectomy Versus Standard Whipple Procedure. Ann. Surg. 2004, 240, 738–745. [Google Scholar] [CrossRef] [PubMed]
- Yeo, C.J.; Cameron, J.L.; Lillemoe, K.D.; Sohn, T.A.; Campbell, K.A.; Sauter, P.K.; Coleman, J.; Abrams, R.A.; Hruban, R.H. Pancreaticoduodenectomy With or Without Distal Gastrectomy and Extended Retroperitoneal Lymphadenectomy for Periampullary Adenocarcinoma, Part 2. Ann. Surg. 2002, 236, 355–368. [Google Scholar] [CrossRef] [PubMed]
- Sasaki, R.; Takahashi, M.; Funato, O.; Nitta, H.; Murakami, M.; Kawamura, H.; Suto, T.; Kanno, S.; Saito, K. Prognostic significance of lymph node involvement in middle and distal bile duct cancer. Surgery 2001, 129, 677–683. [Google Scholar] [CrossRef]
- Jarnagin, W.R.; Ruo, L.; Little, S.A.; Klimstra, D.S.; I Dangelica, M.; DeMatteo, R.P.; Wagman, R.; Blumgart, L.H.; Fong, Y. Patterns of initial disease recurrence after resection of gallbladder carcinoma and hilar cholangiocarcinoma. Cancer 2003, 98, 1689–1700. [Google Scholar] [CrossRef]
- Horgan, A.M.; Amir, E.; Walter, T.; Knox, J.J. Adjuvant Therapy in the Treatment of Biliary Tract Cancer: A Systematic Review and Meta-Analysis. J. Clin. Oncol. 2012, 30, 1934–1940. [Google Scholar] [CrossRef]
- Study Group of Surgical Adjuvant Therapy for Carcinomas of the Pancreas and Biliary Tract; Takada, T.; Amano, H.; Yasuda, H.; Nimura, Y.; Matsushiro, T.; Kato, H.; Nagakawa, T.; Nakayama, T. Is postoperative adjuvant chemotherapy useful for gallbladder carcinoma? Cancer 2002, 95, 1685–1695. [Google Scholar] [CrossRef]
- Cao, H.S.T.; Zhang, Q.; Sada, Y.H.; Chai, C.; Curley, S.A.; Massarweh, N.N.; Curley, S.A. The role of surgery and adjuvant therapy in lymph node-positive cancers of the gallbladder and intrahepatic bile ducts. Cancer 2018, 124, 74–83. [Google Scholar] [CrossRef] [Green Version]
- Chae, H.; Kim, D.; Yoo, C.; Kim, K.-P.; Jeong, J.H.; Chang, H.-M.; Lee, S.S.; Park, D.H.; Song, T.J.; Hwang, S.; et al. Therapeutic relevance of targeted sequencing in management of patients with advanced biliary tract cancer: DNA damage repair gene mutations as a predictive biomarker. Eur. J. Cancer 2019, 120, 31–39. [Google Scholar] [CrossRef] [PubMed]
- Yoo, C.; Oh, D.-Y.; Choi, H.J.; Kudo, M.; Ueno, M.; Kondo, S.; Chen, L.-T.; Osada, M.; Helwig, C.; Dussault, I.; et al. Phase I study of bintrafusp alfa, a bifunctional fusion protein targeting TGF-β and PD-L1, in patients with pretreated biliary tract cancer. J. Immunother. Cancer 2019, 8, e000564. [Google Scholar] [CrossRef] [PubMed]
- Yoo, C.; Hwang, I.; Song, T.J.; Lee, S.S.; Jeong, J.H.; Park, D.H.; Seo, D.W.; Lee, S.K.; Kim, M.-H.; Byun, J.H.; et al. FOLFIRINOX in borderline resectable and locally advanced unresectable pancreatic adenocarcinoma. Ther. Adv. Med Oncol. 2020, 12, 1758835920953294. [Google Scholar] [CrossRef]
- Yoo, C.; Lee, S.S.; Song, K.B.; Jeong, J.H.; Hyung, J.; Park, D.H.; Song, T.J.; Seo, D.W.; Lee, S.K.; Kim, M.-H.; et al. Neoadjuvant modified FOLFIRINOX followed by postoperative gemcitabine in borderline resectable pancreatic adenocarcinoma: A Phase 2 study for clinical and biomarker analysis. Br. J. Cancer 2020, 123, 362–368. [Google Scholar] [CrossRef]
- Shroff, R.T.; Javle, M.M.; Xiao, L.; Kaseb, A.O.; Varadhachary, G.R.; Wolff, R.A.; Raghav, K.P.S.; Iwasaki, M.; Masci, P.; Ramanathan, R.K.; et al. Gemcitabine, Cisplatin, and nab-Paclitaxel for the Treatment of Advanced Biliary Tract Cancers. JAMA Oncol. 2019, 5, 824–830. [Google Scholar] [CrossRef] [PubMed]
- Yoo, C.; Han, B.; Kim, H.S.; Kim, K.-P.; Kim, D.; Jeong, J.H.; Lee, J.-L.; Kim, T.W.; Kim, J.H.; Choi, D.R.; et al. Multicenter Phase II Study of Oxaliplatin, Irinotecan, and S-1 as First-line Treatment for Patients with Recurrent or Metastatic Biliary Tract Cancer. Cancer Res. Treat. 2018, 50, 1324–1330. [Google Scholar] [CrossRef] [Green Version]
- Oh, D.-Y.; Lee, K.-H.; Lee, D.-W.; Kim, T.Y.; Bang, J.-H.; Nam, A.-R.; Lee, Y.; Zhang, Q.; Rebelatto, M.; Li, W.; et al. Phase II study assessing tolerability, efficacy, and biomarkers for durvalumab (D) ± tremelimumab (T) and gemcitabine/cisplatin (GemCis) in chemo-naïve advanced biliary tract cancer (aBTC). J. Clin. Oncol. 2020, 38, 4520. [Google Scholar] [CrossRef]
- Ren, B.; Guo, Q.; Yang, Y.; Liu, L.; Wei, S.; Chen, W.; Tian, Y. A meta-analysis of the efficacy of postoperative adjuvant radiotherapy versus no radiotherapy for extrahepatic cholangiocarcinoma and gallbladder carcinoma. Radiat. Oncol. 2020, 15, 10–15. [Google Scholar] [CrossRef]
- Wang, S.J.; Fuller, C.D.; Kim, J.-S.; Sittig, D.F.; Jr, C.R.T.; Ravdin, P.M. Prediction Model for Estimating the Survival Benefit of Adjuvant Radiotherapy for Gallbladder Cancer. J. Clin. Oncol. 2008, 26, 2112–2117. [Google Scholar] [CrossRef]
- Mitin, T.; Enestvedt, C.K.; Jemal, A.; Sineshaw, H.M. Limited Use of Adjuvant Therapy in Patients With Resected Gallbladder Cancer Despite a Strong Association With Survival. J. Natl. Cancer Inst. 2017, 109, 2112–2119. [Google Scholar] [CrossRef] [Green Version]
- Hoehn, R.S.; Wima, K.; Ertel, A.E.; Meier, A.; Ahmad, S.A.; Shah, S.A.; Abbott, D.E. Adjuvant Chemotherapy and Radiation Therapy is Associated with Improved Survival for Patients with Extrahepatic Cholangiocarcinoma. Ann. Surg. Oncol. 2015, 22, 1133–1139. [Google Scholar] [CrossRef]
- Nassour, I.; Mokdad, A.A.; Porembka, M.R.; Choti, M.A.; Polanco, P.M.; Mansour, J.C.; Minter, R.M.; Wang, S.C.; Yopp, A.C. Adjuvant Therapy Is Associated with Improved Survival in Resected Perihilar Cholangiocarcinoma: A Propensity Matched Study. Ann. Surg. Oncol. 2018, 25, 1193–1201. [Google Scholar] [CrossRef]
- Ben-Josef, E.; Guthrie, K.A.; El-Khoueiry, A.B.; Corless, C.L.; Zalupski, M.M.; Lowy, A.M.; Jr, C.R.T.; Alberts, S.R.; Dawson, L.A.; Micetich, K.C.; et al. SWOG S0809: A Phase II Intergroup Trial of Adjuvant Capecitabine and Gemcitabine Followed by Radiotherapy and Concurrent Capecitabine in Extrahepatic Cholangiocarcinoma and Gallbladder Carcinoma. J. Clin. Oncol. 2015, 33, 2617–2622. [Google Scholar] [CrossRef] [Green Version]
- Shroff, R.T.; Kennedy, E.B.; Bachini, M.; Bekaii-Saab, T.; Crane, C.; Edeline, J.; El-Khoueiry, A.; Feng, M.; Katz, M.H.; Primrose, J.; et al. Adjuvant Therapy for Resected Biliary Tract Cancer: ASCO Clinical Practice Guideline. J. Clin. Oncol. 2019, 37, 1015–1027. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Valle, J.W.; Borbath, I.; Khan, S.A.; Huguet, F.; Gruenberger, T.; Arnold, D. Biliary cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2016, 27, v28–v37. [Google Scholar] [CrossRef] [PubMed]
- Moriwaki, T.; Yamamoto, Y.; Gosho, M.; Kobayashi, M.; Sugaya, A.; Yamada, T.; Endo, S.; Hyodo, I. Correlations of survival with progression-free survival, response rate, and disease control rate in advanced biliary tract cancer: A meta-analysis of randomised trials of first-line chemotherapy. Br. J. Cancer 2016, 114, 881–888. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Variables | BILCAP Trial | PRODIGE 12 Trial | BCAT Trial | |||
|---|---|---|---|---|---|---|
| Treatment | CAP | Observation | GEMOX | Observation | GEM | Observation |
| Patient number | 223 | 224 | 95 | 99 | 117 | 108 |
| Age, median (range) | 62 (55–68) | 64 (55–69) | 63 (33–83) | 63 (41–80) | ≥70 years: 56% | ≥70 years: 43% |
| Gender, male/female | 50%/50% | 50%/50% | 60%/40% | 50%/50% | 66%/34% | 76%/24% |
| Primary tumor site | ||||||
| IH-CCA | 43 (19%) | 41 (18%) | 41 (43%) | 45 (46%) | 0 | 0 |
| Perihilar CCA | 65 (29%) | 63 (28%) | 10 (11%) | 5 (5%) | 51 (44%) | 51 (47%) |
| Distal CCA | 76 (34%) | 80 (36%) | 27 (28%) | 28 (28%) | 66 (56%) | 57 (53%) |
| GBCA | 39 (17%) | 40 (18%) | 17 (18%) | 21 (21%) | 0 | 0 |
| Resection status | ||||||
| R0 | 139 (62%) | 140 (63%) | 82 (86%) | 87 (88%) | 106 (91%) | 94 (87%) |
| R1 | 84 (38%) | 84 (38%) | 13 (14%) | 12 (12%) | 11 (9%) | 14 (13%) |
| Nodal status | ||||||
| Negative | 115 (52%) | 121 (54%) | 49 (52%) | 48 (48%) | 75 (64%) | 72 (67%) |
| Positive | 108 (48%) | 102 (46%) | 35 (37%) | 36 (36%) | 42 (36%) | 36 (33%) |
| Missing | 0 | 1 (<1%) | 11 (12%) | 15 (15%) | ||
| Variables | BILCAP Trial (ITT) | BILCAP Trial (PP) | PRODIGE 12 Trial | BCAT Trial | ||||
|---|---|---|---|---|---|---|---|---|
| Treatment | CAP | Observation | CAP | Observation | GEMOX | Observation | GEM | Observation |
| Median OS, months (95% CI) | 51.1 (34.6–59.1) | 36.4 (29.7–44.5) | 53 (40-not reached) | 36 (30–44) | 75.8 (34.4-not reached) | 50.8 (38.0-not reached) | 62.3 | 63.8 |
| HR (95% CI) | 0.81 (0.63–1.04) | p = 0.097 | 0.75 (0.58–0.97) | p = 0.028 | 1.08 (0.70–1.66) | p = 0.74 | 1.01 (0.70–1.45) | p = 0.964 |
| Median RFS, months (95% CI) | 24.4 (18.6–35.9) | 17.5 (12.0–23.8) | 25.9 (19.8–46.3) | 17.4 (12.0–23.7) | 30.4 (15.4–43.0) | 18.5 (12.6–38.2) | 36.0 | 39.9 |
| HR (95% CI) | 0.75 (0.58–0.98) | p = 0.033 | 0.70 (0.54–0.92) | p = 0.0093 | 0.88 (0.62–1.25) | 0.48 | 0.93 (0.66–1.32) | p = 0.693 |
| Registered Number | Country | Phase | Number of Target Patients | Target Disease | Investigational Arm | Control Arm | Primary Endpoint |
|---|---|---|---|---|---|---|---|
| Adjuvant chemotherapy | |||||||
| NCT02170090 (ACTICCA-1) | Germany/ Netherland/UK/ Austrailia | III | 781 | IH-CCA, EH-CCA, GBCA | GemCis | Observation → CAP | DFS |
| NCT02548195 | China | III | 286 | IH-CCA | GEMOX | GEM | DFS |
| UMIN000011688 (JCOG1202, ASCOT) | Japan | III | 440 | IH-CCA, EH-CCA, GBCA, ampullary cancer | S-1 | Observation | OS |
| NCT03079427 (STAMP) | Korea | II | 100 | LN-positive EH-CCA | GemCis | CAP | DFS |
| NCT04401709 | Korea | III | 490 | IH-CCA, EH-CCA, GBCA | GEM+CAP | CAP | DFS |
| Neoadjuvant chemotherapy | |||||||
| NCT03673072 (GAIN) | Germany | III | 300 | Incidental GBCA | GemCis | Upfront surgery | OS |
| NCT04308174 (DEBATE) | Korea | II | 45 | IH-CCA, EH-CCA, GBCA | Durvalumab + GemCis | GemCis | R0 resection rate |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoo, C.; Shin, S.H.; Park, J.-O.; Kim, K.-P.; Jeong, J.H.; Ryoo, B.-Y.; Lee, W.; Song, K.-B.; Hwang, D.-W.; Park, J.-h.; et al. Current Status and Future Perspectives of Perioperative Therapy for Resectable Biliary Tract Cancer: A Multidisciplinary Review. Cancers 2021, 13, 1647. https://doi.org/10.3390/cancers13071647
Yoo C, Shin SH, Park J-O, Kim K-P, Jeong JH, Ryoo B-Y, Lee W, Song K-B, Hwang D-W, Park J-h, et al. Current Status and Future Perspectives of Perioperative Therapy for Resectable Biliary Tract Cancer: A Multidisciplinary Review. Cancers. 2021; 13(7):1647. https://doi.org/10.3390/cancers13071647
Chicago/Turabian StyleYoo, Changhoon, Sang Hyun Shin, Joon-Oh Park, Kyu-Pyo Kim, Jae Ho Jeong, Baek-Yeol Ryoo, Woohyung Lee, Ki-Byung Song, Dae-Wook Hwang, Jin-hong Park, and et al. 2021. "Current Status and Future Perspectives of Perioperative Therapy for Resectable Biliary Tract Cancer: A Multidisciplinary Review" Cancers 13, no. 7: 1647. https://doi.org/10.3390/cancers13071647