Radiotherapy-Induced High Neutrophil-to-Lymphocyte Ratio is a Negative Prognostic Factor in Patients with Breast Cancer

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Results
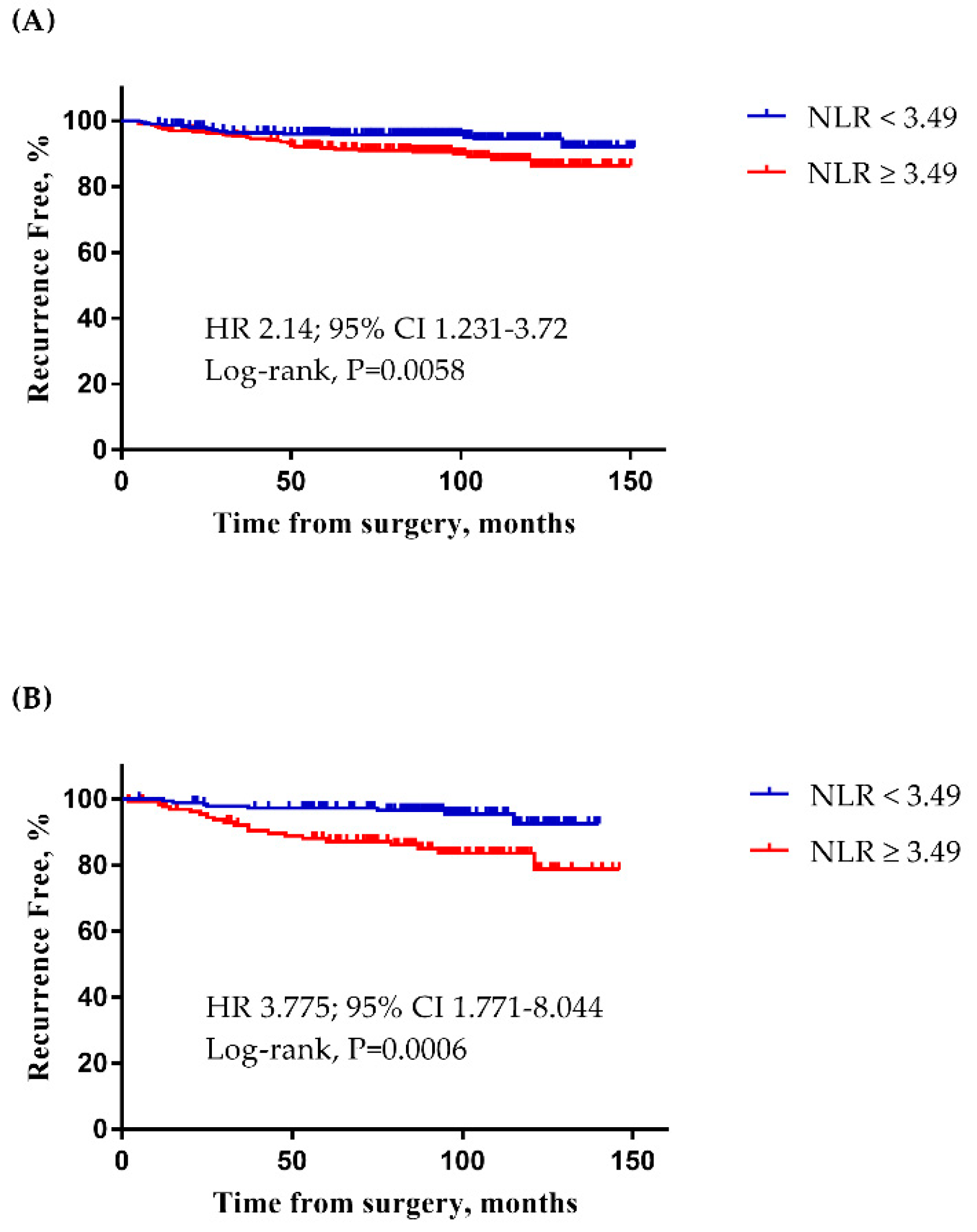
2.1. The Determination of the NLR Cut-Off Point
2.2. Characteristics of Patients with RT-Induced High NLR
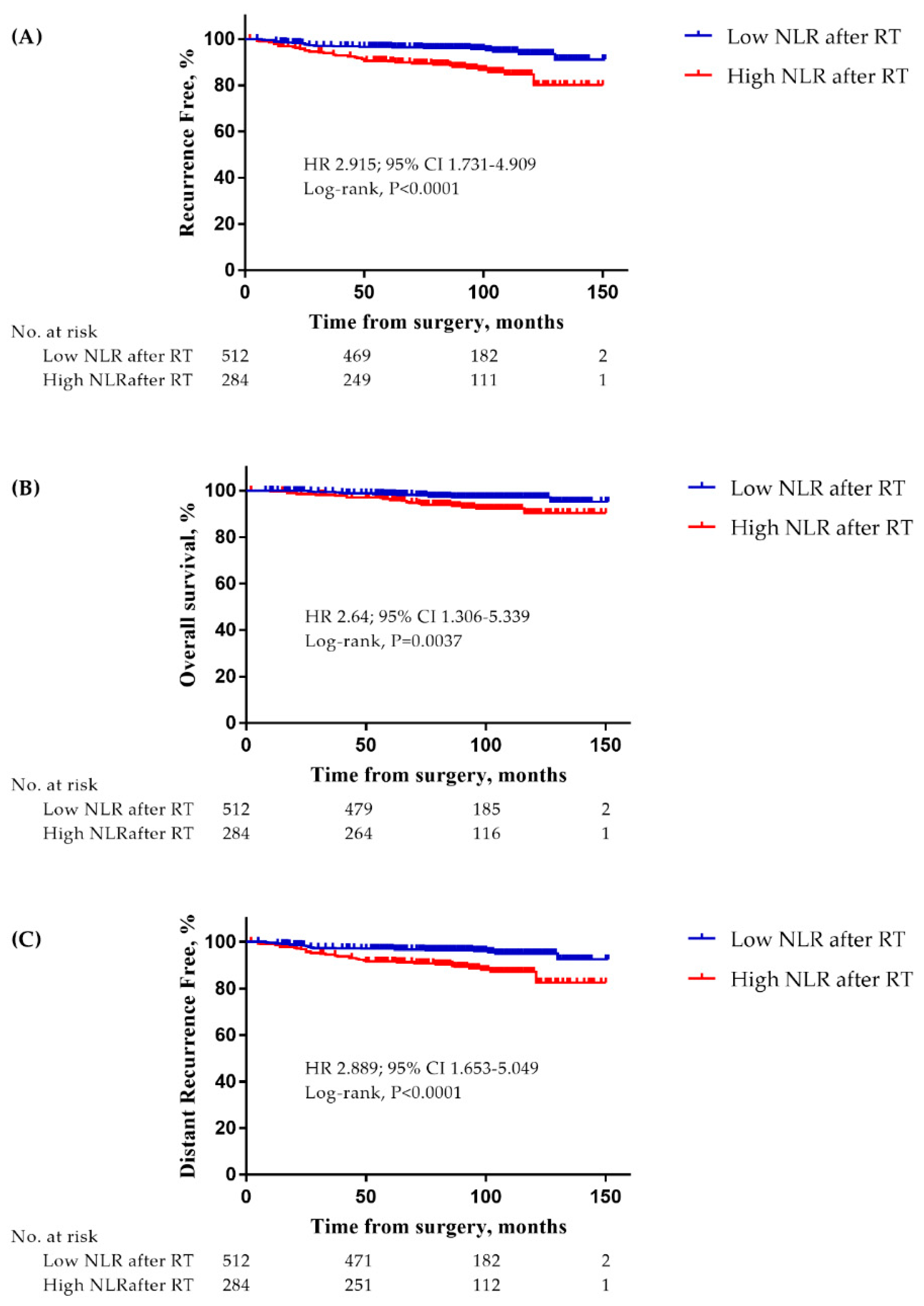
2.3. Prognostic Impact of RT-Induced High NLR
3. Discussion
4. Materials and Methods
4.1. Patients
4.2. Treatment and Blood Cell Count Examination
4.3. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Hanahan, D.; Weinberg, R.A. Hallmarks of cancer: The next generation. Cell 2011, 144, 646–674. [Google Scholar] [CrossRef] [Green Version]
- McKinstry, W.J.; Li, C.L.; Rasko, J.E.; Nicola, N.A.; Johnson, G.R.; Metcalf, D. Cytokine receptor expression on hematopoietic stem and progenitor cells. Blood 1997, 89, 65–71. [Google Scholar] [CrossRef] [Green Version]
- Steinbach, K.H.; Schick, P.; Trepel, F.; Raffler, H.; Dohrmann, J.; Heilgeist, G.; Heltzel, W.; Li, K.; Past, W.; van der Woerd-de Lange, J.A.; et al. Estimation of kinetic parameters of neutrophilic, eosinophilic, and basophilic granulocytes in human blood. Blut 1979, 39, 27–38. [Google Scholar] [CrossRef]
- Jamieson, T.; Clarke, M.; Steele, C.W.; Samuel, M.S.; Neumann, J.; Jung, A.; Huels, D.; Olson, M.F.; Das, S.; Nibbs, R.J.; et al. Inhibition of CXCR2 profoundly suppresses inflammation-driven and spontaneous tumorigenesis. J. Clin. Investig. 2012, 122, 3127–3144. [Google Scholar] [CrossRef]
- Antonio, N.; Bonnelykke-Behrndtz, M.L.; Ward, L.C.; Collin, J.; Christensen, I.J.; Steiniche, T.; Schmidt, H.; Feng, Y.; Martin, P. The wound inflammatory response exacerbates growth of pre-neoplastic cells and progression to cancer. EMBO J. 2015, 34, 2219–2236. [Google Scholar] [CrossRef]
- El-Hag, A.; Clark, R.A. Immunosuppression by activated human neutrophils. Dependence on the myeloperoxidase system. J. Immunol. 1987, 139, 2406–2413. [Google Scholar] [PubMed]
- Kusumanto, Y.H.; Dam, W.A.; Hospers, G.A.; Meijer, C.; Mulder, N.H. Platelets and granulocytes, in particular the neutrophils, form important compartments for circulating vascular endothelial growth factor. Angiogenesis 2003, 6, 283–287. [Google Scholar] [CrossRef] [PubMed]
- Jablonska, J.; Leschner, S.; Westphal, K.; Lienenklaus, S.; Weiss, S. Neutrophils responsive to endogenous IFN-beta regulate tumor angiogenesis and growth in a mouse tumor model. J. Clin. Investig. 2010, 120, 1151–1164. [Google Scholar] [CrossRef]
- Hofman, P.M. Pathobiology of the neutrophil-intestinal epithelial cell interaction: Role in carcinogenesis. World J. Gastroenterol. 2010, 16, 5790–5800. [Google Scholar] [CrossRef] [PubMed]
- Balkwill, F.; Mantovani, A. Inflammation and cancer: Back to Virchow? Lancet 2001, 357, 539–545. [Google Scholar] [CrossRef]
- Coussens, L.M.; Werb, Z. Inflammation and cancer. Nature 2002, 420, 860–867. [Google Scholar] [CrossRef] [PubMed]
- De Larco, J.E.; Wuertz, B.R.; Furcht, L.T. The potential role of neutrophils in promoting the metastatic phenotype of tumors releasing interleukin-8. Clin. Cancer Res. 2004, 10, 4895–4900. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ethier, J.L.; Desautels, D.; Templeton, A.; Shah, P.S.; Amir, E. Prognostic role of neutrophil-to-lymphocyte ratio in breast cancer: A systematic review and meta-analysis. Breast Cancer Res. 2017, 19, 2. [Google Scholar] [CrossRef] [Green Version]
- Ethier, J.L.; Desautels, D.N.; Templeton, A.J.; Oza, A.; Amir, E.; Lheureux, S. Is the neutrophil-to-lymphocyte ratio prognostic of survival outcomes in gynecologic cancers? A systematic review and meta-analysis. Gynecol. Oncol. 2017, 145, 584–594. [Google Scholar] [CrossRef]
- Haram, A.; Boland, M.R.; Kelly, M.E.; Bolger, J.C.; Waldron, R.M.; Kerin, M.J. The prognostic value of neutrophil-to-lymphocyte ratio in colorectal cancer: A systematic review. J. Surg. Oncol. 2017, 115, 470–479. [Google Scholar] [CrossRef]
- Tang, H.; Lu, W.; Li, B.; Li, C.; Xu, Y.; Dong, J. Prognostic significance of neutrophil-to-lymphocyte ratio in biliary tract cancers: A systematic review and meta-analysis. Oncotarget 2017, 8, 36857–36868. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wei, B.; Yao, M.; Xing, C.; Wang, W.; Yao, J.; Hong, Y.; Liu, Y.; Fu, P. The neutrophil lymphocyte ratio is associated with breast cancer prognosis: An updated systematic review and meta-analysis. OncoTargets Ther. 2016, 9, 5567–5575. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yin, Y.; Wang, J.; Wang, X.; Gu, L.; Pei, H.; Kuai, S.; Zhang, Y.; Shang, Z. Prognostic value of the neutrophil to lymphocyte ratio in lung cancer: A meta-analysis. Clinics 2015, 70, 524–530. [Google Scholar] [CrossRef]
- Szor, D.J.; Dias, A.R.; Pereira, M.A.; Ramos, M.; Zilberstein, B.; Cecconello, I.; Ribeiro-Junior, U. Prognostic Role of Neutrophil/Lymphocyte Ratio in Resected Gastric Cancer: A Systematic Review and Meta-analysis. Clinics (Sao Paulo) 2018, 73, e360. [Google Scholar] [CrossRef] [PubMed]
- McLaren, P.J.; Bronson, N.W.; Hart, K.D.; Vaccaro, G.M.; Gatter, K.M.; Thomas, C.R., Jr.; Hunter, J.G.; Dolan, J.P. Neutrophil-to-Lymphocyte and Platelet-to-Lymphocyte Ratios can Predict Treatment Response to Neoadjuvant Therapy in Esophageal Cancer. J. Gastrointest Surg. 2017, 21, 607–613. [Google Scholar] [CrossRef]
- Xu, J.; Ni, C.; Ma, C.; Zhang, L.; Jing, X.; Li, C.; Liu, Y.; Qu, X. Association of neutrophil/lymphocyte ratio and platelet/lymphocyte ratio with ER and PR in breast cancer patients and their changes after neoadjuvant chemotherapy. Clin. Transl. Oncol. 2017, 19, 989–996. [Google Scholar] [CrossRef] [PubMed]
- Shen, J.; Zhu, Y.; Wu, W.; Zhang, L.; Ju, H.; Fan, Y.; Zhu, Y.; Luo, J.; Liu, P.; Zhou, N.; et al. Prognostic Role of Neutrophil-to-Lymphocyte Ratio in Locally Advanced Rectal Cancer Treated with Neoadjuvant Chemoradiotherapy. Med. Sci. Monit. 2017, 23, 315–324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cannon, N.A.; Meyer, J.; Iyengar, P.; Ahn, C.; Westover, K.D.; Choy, H.; Timmerman, R. Neutrophil-lymphocyte and platelet-lymphocyte ratios as prognostic factors after stereotactic radiation therapy for early-stage non-small-cell lung cancer. J. Thorac. Oncol. 2015, 10, 280–285. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raben, M.; Walach, N.; Galili, U.; Schlesinger, M. The effect of radiation therapy on lymphocyte subpopulations in cancer patients. Cancer 1976, 37, 1417–1421. [Google Scholar] [CrossRef]
- Tisch, M.; Heimlich, F.; Daniel, V.; Opelz, G.; Maier, H. Cellular immune defect caused by postsurgical radiation therapy in patients with head and neck cancer. Otolaryngol. Head. Neck Surg. 1998, 119, 412–417. [Google Scholar] [CrossRef]
- Yovino, S.; Kleinberg, L.; Grossman, S.A.; Narayanan, M.; Ford, E. The etiology of treatment-related lymphopenia in patients with malignant gliomas: Modeling radiation dose to circulating lymphocytes explains clinical observations and suggests methods of modifying the impact of radiation on immune cells. Cancer Investig. 2013, 31, 140–144. [Google Scholar] [CrossRef] [Green Version]
- Rotstein, S.; Blomgren, H.; Petrini, B.; Wasserman, J.; Baral, E. Long term effects on the immune system following local radiation therapy for breast cancer. I. Cellular composition of the peripheral blood lymphocyte population. Int. J. Radiat. Oncol. Biol. Phys. 1985, 11, 921–925. [Google Scholar] [CrossRef]
- Chamberlain, S.M.; Short, J.H.; Nias, A.H. Recovery of lymphocyte status after radiotherapy. Clin. Radiol. 1980, 31, 427–432. [Google Scholar] [CrossRef]
- Dumitru, C.A.; Lang, S.; Brandau, S. Modulation of neutrophil granulocytes in the tumor microenvironment: Mechanisms and consequences for tumor progression. Semin. Cancer Biol. 2013, 23, 141–148. [Google Scholar] [CrossRef]
- Fridlender, Z.G.; Sun, J.; Kim, S.; Kapoor, V.; Cheng, G.; Ling, L.; Worthen, G.S.; Albelda, S.M. Polarization of tumor-associated neutrophil phenotype by TGF-beta: “N1” versus “N2” TAN. Cancer Cell 2009, 16, 183–194. [Google Scholar] [CrossRef] [Green Version]
- Takeshima, T.; Pop, L.M.; Laine, A.; Iyengar, P.; Vitetta, E.S.; Hannan, R. Key role for neutrophils in radiation-induced antitumor immune responses: Potentiation with G-CSF. Proc. Natl. Acad. Sci. USA 2016, 113, 11300–11305. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wisdom, A.J.; Hong, C.S.; Lin, A.J.; Xiang, Y.; Cooper, D.E.; Zhang, J.; Xu, E.S.; Kuo, H.-C.; Mowery, Y.M.; Carpenter, D.J.; et al. Neutrophils promote tumor resistance to radiation therapy. Proc. Natl. Acad. Sci. USA 2019, 116, 18584–18589. [Google Scholar] [CrossRef] [Green Version]
- Nakamura, N.; Kusunoki, Y.; Akiyama, M. Radiosensitivity of CD4 or CD8 Positive Human T-Lymphocytes by an in Vitro Colony Formation Assay. Radiat. Res. 1990, 123, 224–227. [Google Scholar] [CrossRef]
- Rostom, A.; Dube, C.; Lewin, G.; Tsertsvadze, A.; Barrowman, N.; Code, C.; Sampson, M.; Moher, D. Nonsteroidal anti-inflammatory drugs and cyclooxygenase-2 inhibitors for primary prevention of colorectal cancer: A systematic review prepared for the U.S. Preventive Services Task Force. Ann. Int. Med. 2007, 146, 376–389. [Google Scholar] [CrossRef] [PubMed]
- Venkatesulu, B.P.; Mallick, S.; Lin, S.H.; Krishnan, S. A systematic review of the influence of radiation-induced lymphopenia on survival outcomes in solid tumors. Crit. Rev. Oncol. Hematol. 2018, 123, 42–51. [Google Scholar] [CrossRef] [PubMed]
- Mike, V.; Currie, V.E.; Gee, T.S. Fatal neutropenia associated with long-term tamoxifen therapy. Lancet 1994, 344, 541–542. [Google Scholar] [CrossRef]
- International Adjuvant Therapy Organisation. Myelosuppression occurring after receiving tamoxifen for breast cancer. Br. J. Radiol. 1985, 58, 1220. [Google Scholar] [CrossRef] [PubMed]
- Choi, N.; Kim, J.H.; Chie, E.K.; Gim, J.; Kang, H.-C. A meta-analysis of the impact of neutrophil-to-lymphocyte ratio on treatment outcomes after radiotherapy for solid tumors. Medicine 2019, 98, e15369. [Google Scholar] [CrossRef] [PubMed]
- Harvey, J.M.; Clark, G.M.; Osborne, C.K.; Allred, D.C. Estrogen receptor status by immunohistochemistry is superior to the ligand-binding assay for predicting response to adjuvant endocrine therapy in breast cancer. J. Clin. Oncol. 1999, 17, 1474–1481. [Google Scholar] [CrossRef]
- Yin, J.; Tian, L. Joint confidence region estimation for area under ROC curve and Youden index. Stat. Med. 2014, 33, 985–1000. [Google Scholar] [CrossRef] [PubMed]
- Youden, W.J. Index for rating diagnostic tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | High NLR, n = 284 (%) | Low NLR, n = 512 (%) | p Value |
|---|---|---|---|
| Age, year | 0.369 | ||
| ≥50 | 142 (50.0) | 273 (53.3) | |
| <50 | 142 (50.0) | 239 (46.7) | |
| ER | 0.310 | ||
| Positive | 210 (73.9) | 395 (77.1) | |
| Negative | 74 (26.1) | 117 (22.9) | |
| PR a | 0.463 | ||
| Positive | 169 (59.5) | 317 (62.2) | |
| Negative | 115 (40.5) | 193 (37.8) | |
| HER2 a,b | 0.112 | ||
| Positive | 94 (33.3) | 199 (39.0) | |
| Negative | 188 (66.7) | 311 (61.0) | |
| NG a | 0.176 | ||
| I, II | 194 (77.9) | 329 (73.3) | |
| III | 55 (22.1) | 120 (26.7) | |
| HG a | 0.915 | ||
| I, II | 207 (76.1) | 370 (76.4) | |
| III | 65 (23.9) | 114 (23.6) | |
| Tumor size a, cm | 0.968 | ||
| ≤2 | 239 (84.8) | 430 (84.6) | |
| >2 | 43 (15.2) | 78 (15.4) | |
| LN metastasis | 0.001 | ||
| Negative | 225 (79.2) | 449 (87.7) | |
| Positive | 59 (20.8) | 63 (12.3) | |
| Subtype a | 0.284 | ||
| Luminal/HER2(−) | 146 (51.8) | 243 (47.8) | |
| HER2(+) | 94 (33.3) | 198 (39.0) | |
| TNBC | 42 (14.9) | 67 (13.2) | |
| Chemotherapy | 0.003 | ||
| Done | 145 (51.1) | 205 (40.0) | |
| Not done/unknown | 139 (48.9) | 307 (60.0) | |
| Regional nodal irradiation | <0.001 | ||
| Done | 104 (37.0) | 75 (14.8) | |
| Not done | 177 (63.0) | 431 (85.2) |
| Variables | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HRs (95% CIs) | p Value | HRs (95% CIs) | p Value | |
| Age, year | 0.946 | |||
| >50 | 1 | |||
| ≤50 | 0.983 (0.597–1.618) | |||
| NG | 0.019 | |||
| I, II | 1 | |||
| III | 1.920 (1.114–3.308) | |||
| HG | 0.063 | |||
| I, II | 1 | |||
| III | 1.649 (0.974–2.792) | |||
| ER | 0.004 | 0.004 | ||
| Negative | 1 | 1 | ||
| Positive | 0.469 (0.282–0.782) | 0.451 (0.260–0.780) | ||
| PR | 0.019 | |||
| Negative | 1 | |||
| Positive | 0.551 (0.334–0.907) | |||
| HER2 | 0.131 | |||
| Negative | 1 | |||
| Positive | 1.476 (0.890–2.447) | |||
| Tumor size, cm | 0.065 | |||
| ≤2 | 1 | |||
| >2 | 1.754 (0.966–3.183) | |||
| LN metastasis | <0.001 | 0.001 | ||
| Negative | 1 | 1 | ||
| Positive | 4.439 (2.660–7.407) | 2.774 (1.484–5.186) | ||
| Subtype | 0.066 | |||
| Luminal/HER2(−) | 1 | |||
| HER2(+) | 1.774 (1.014–3.104) | |||
| TNBC | 1.939 (0.965–3.896) | |||
| RT-induced high NLR | <0.001 | 0.008 | ||
| <3.49 | 1 | 1 | ||
| ≥3.49 | 2.918 (1.750–4.866) | 2.194 (1.230–3.912) | ||
| Regional nodal irradiation | <0.001 | 0.052 | ||
| Done | 1 | 1 | ||
| Not done | 3.869 (2.332–6.421) | 1.879 (0.993–3.553) | ||
| Chemotherapy | <0.001 | |||
| Done | 1 | |||
| Not done/unknown | 3.173 (1.853–5.435) | |||
| Variables | Univariate Analysis | Multivariate Analysis | ||
|---|---|---|---|---|
| HRs (95% CIs) | p Value | HRs (95% CIs) | p Value | |
| Age, year | 0.754 | |||
| >50 | 1 | |||
| ≤50 | 0.918 (0.538–1.565) | |||
| NG | 0.076 | |||
| I, II | 1 | |||
| III | 1.681 (0.946–2.987) | |||
| HG | 0.108 | |||
| I, II | 1 | |||
| III | 1.593 (0.904–2.807) | |||
| ER | 0.082 | |||
| Negative | 1 | |||
| Positive | 0.605 (0.344–1.066) | |||
| PR | 0.102 | |||
| Negative | 1 | |||
| Positive | 0.640 (0.375–1.093) | |||
| HER2 | 0.073 | |||
| Negative | 1 | |||
| Positive | 1.637 (0.955–2.805) | |||
| Tumor size, cm | 0.044 | |||
| ≤2 | 1 | |||
| >2 | 1.898 (1.016–3.544) | |||
| LN metastasis | <0.001 | 0.001 | ||
| Negative | 1 | 1 | ||
| Positive | 4.452 (2.574–7.700) | 2.860 (1.512–5.407) | ||
| Subtype | 0.191 | |||
| Luminal/HER2(−) | 1 | |||
| HER2(+) | 1.693 (0.951–3.014) | |||
| TNBC | 1.153 (0.492–2.698) | |||
| RT-induced high NLR | <0.001 | 0.004 | ||
| <3.49 | 1 | 1 | ||
| ≥3.49 | 2.891 (1.673–4.998) | 2.313 (1.299–4.120) | ||
| Regional nodal irradiation | <0.001 | 0.078 | ||
| Done | 1 | 1 | ||
| Not done | 3.452 (2.006–5.942) | 1.777 (0.938–3.366) | ||
| Chemotherapy | <0.001 | |||
| Done | 1 | |||
| Not done/unknown | 2.946 (1.665–5.213) | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoon, C.I.; Kim, D.; Ahn, S.G.; Bae, S.J.; Cha, C.; Park, S.; Park, S.; Kim, S.I.; Lee, H.S.; Park, J.Y.; et al. Radiotherapy-Induced High Neutrophil-to-Lymphocyte Ratio is a Negative Prognostic Factor in Patients with Breast Cancer. Cancers 2020, 12, 1896. https://doi.org/10.3390/cancers12071896
Yoon CI, Kim D, Ahn SG, Bae SJ, Cha C, Park S, Park S, Kim SI, Lee HS, Park JY, et al. Radiotherapy-Induced High Neutrophil-to-Lymphocyte Ratio is a Negative Prognostic Factor in Patients with Breast Cancer. Cancers. 2020; 12(7):1896. https://doi.org/10.3390/cancers12071896
Chicago/Turabian StyleYoon, Chang Ik, Dooreh Kim, Sung Gwe Ahn, Soong June Bae, Chihwan Cha, Soeun Park, Seho Park, Seung Il Kim, Hye Sun Lee, Ju Young Park, and et al. 2020. "Radiotherapy-Induced High Neutrophil-to-Lymphocyte Ratio is a Negative Prognostic Factor in Patients with Breast Cancer" Cancers 12, no. 7: 1896. https://doi.org/10.3390/cancers12071896