Treatment of Locally Advanced Gastric Cancer (LAGC): Back to Lauren’s Classification in Pan–Cancer Analysis Era?

 ,
,  , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
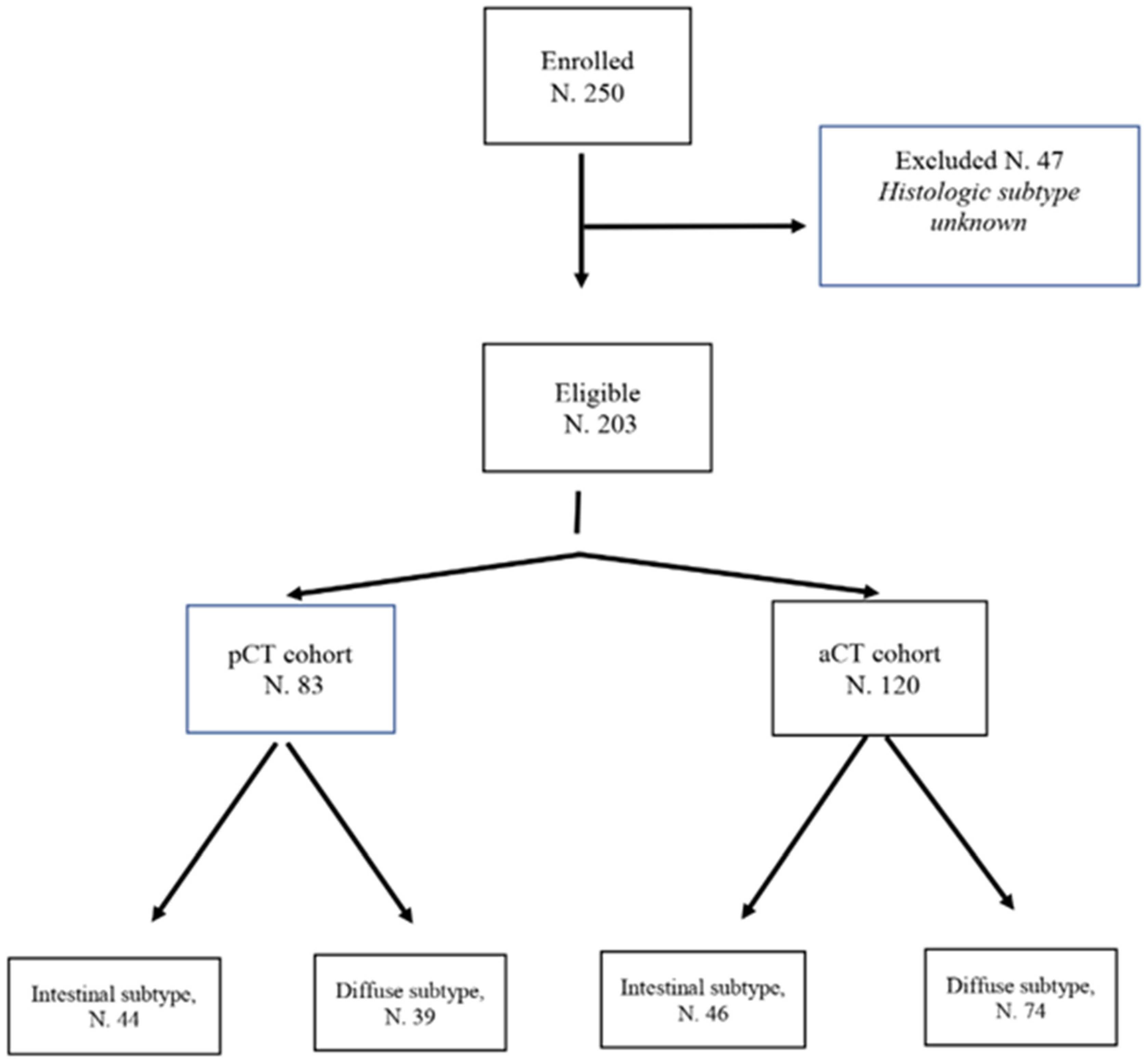
2.1. Study Population
2.2. Treatment Procedures
2.3. Statistical Analysis
3. Results
3.1. Patients Characteristics
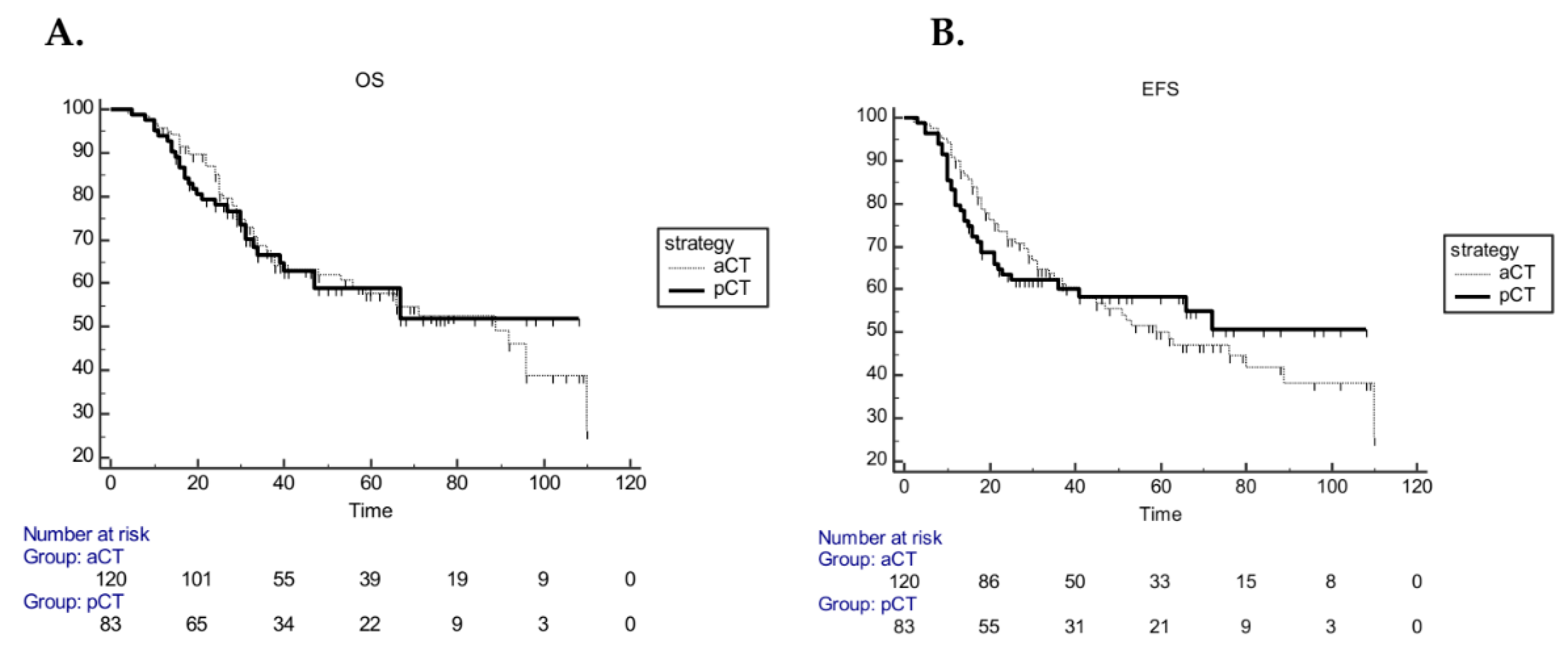
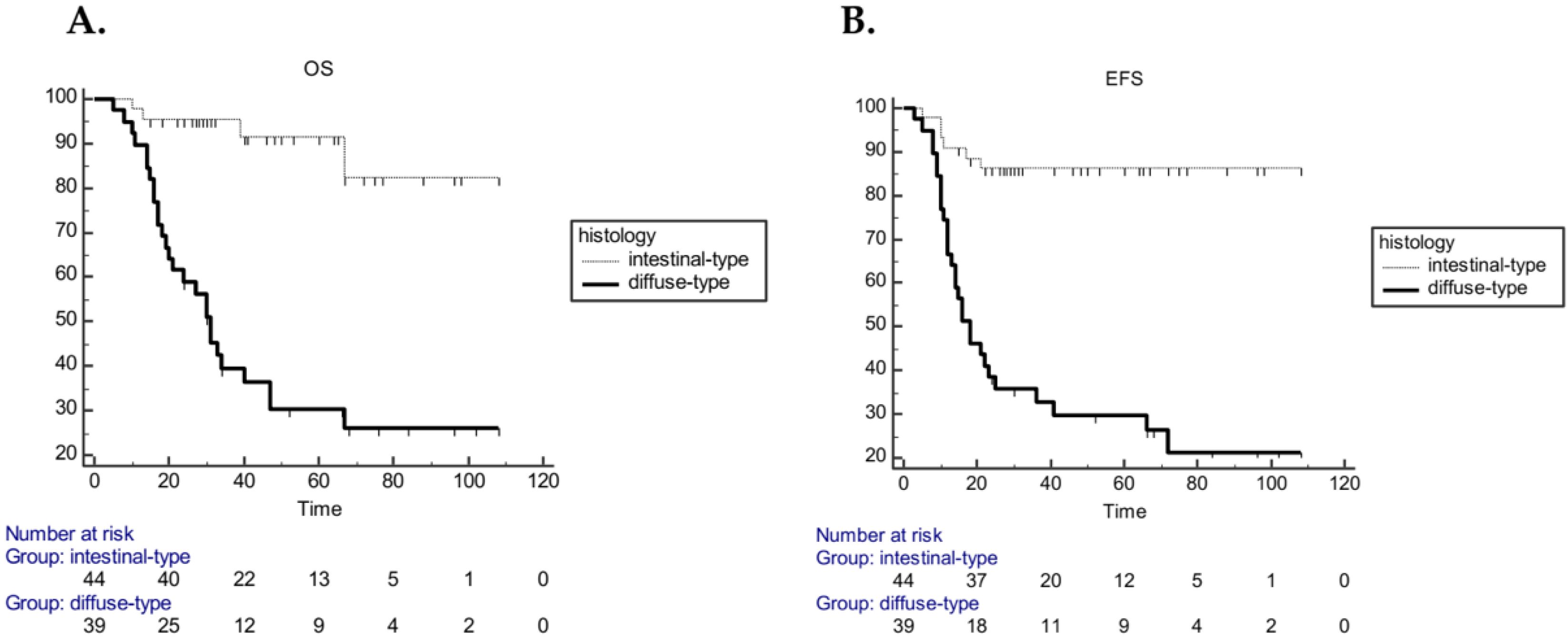
3.2. Outcome
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Ethical Approval and Consent to Participate
References
- Gee, D.W.; Rattner, D.W. Management of gastroesophageal tumors. Oncologist 2007, 12, 175–185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siewert, J.R.; Bottcher, K.; Roder, J.D.; Busch, R.; Hermanek, O.; Meyer, H.J. Prognostic relevance of systematic lymph node dissection in gastric carcinoma: German Gastric Carcinoma Study Group. Br. J. Surg. 1993, 80, 1015–1018. [Google Scholar] [CrossRef]
- Macdonald, J.S.; Smalley, S.R.; Benedetti, J.; Hundahl, S.A.; Estes, N.C.; Stemmermann, G.N.; Haller, D.G.; Ajani, J.A.; Gunderson, L.L.; Jessup, L.M.; et al. Chemoradiotherapy after surgery compared with surgery alone for adenocarcinoma of the stomach or gastroesophageal junction. N. Engl. J. Med. 2001, 345, 725–730. [Google Scholar] [CrossRef]
- Nakajima, T.; Nashimoto, A.; Kitamura, M.; Kito, T.; Iwanaga, T.; Okabayashi, K.; Goto, M. Adjuvant mitomycin and fluorouracil followed by oral uracil plus tegafur in serosa–negative gastric cancer: A randomised trial. The Lancet 1999, 354, 273–277. [Google Scholar] [CrossRef]
- Cascinu, S.; Labianca, R.; Barone, C.; Santoro, A.; Carnaghi, C.; Cassano, A.; Beretta, G.; Catalano, V.; Bertetto, O.; Barni, S.; et al. Adjuvant treatment of high-risk, radically resected gastric cancer patients with 5-fluorouracil, leucovorin, cisplatin, and epidoxorubicin in a randomized controlled trial. J. Natl. Cancer Inst. 2007, 99, 601–607. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Lim, D.H.; Kim, S.; Park, J.O.; Park, J.S.; Lim, H.Y.; Choi, M.G.; Sohn, T.S.; Noh, J.H.; Bae, J.M.; et al. Phase III trial comparing capecitabine plus cisplatin versus capecitabine plus cisplatin with concurrent capecitabine radiotherapy in completely resected gastric cancer with D2 lymph node dissection: The ARTIST trial. J. Clin. Oncol. 2012, 30, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Sakuramoto, S.; Sasako, M.; Yamaguchi, T.; Kinoshita, T.; Fujii, M.; Nashimoto, A.; Furukawa, H.; Nakajima, T.; Ohashi, Y.; Imamura, H.; et al. Adjuvant chemotherapy for gastric cancer with S-1, an oral fluoropyrimidine. N. Eng.l J. Med. 2007, 357, 1810–1820. [Google Scholar] [CrossRef]
- Bang, Y.J.; Kim, Y.W.; Yang, H.K.; Chung, H.C.; Park, Y.K.; Lee, K.W.; Kim, Y.H.; Noh, S.; Cho, J.Y.; Mok, Y.J.; et al. Adjuvant capecitabine and oxaliplatin for gastric cancer after D2 gastrectomy (CLASSIC): A phase 3 open-label, randomised controlled trial. The Lancet 2012, 379, 315–321. [Google Scholar] [CrossRef]
- Cunnigham, D.; Allum, W.H.; Stenning, S.P.; Thompson, J.N.; Van de Velde, C.J.; Nicolson, M.; Howard, S.J.; Lofts, F.J.; Falk, S.J.; Iveson, T.J.; et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N. Engl. J. Med. 2006, 355, 11–20. [Google Scholar] [CrossRef]
- Ychou, M.; Boige, V.; Pignon, J.P.; Conroy, T.; Bouchè, O.; Lebreton, G.; Ducourtieux, M.; Bedenn, L.; Fabre, L.M.; Saint-Aubert, B.; et al. Perioperative chemotherapy compared with surgery alone for resectable gastroesophageal adenocarcinoma: An FNCLCC and FFCD multicenter phase III trial. J. Clin. Oncol. 2011, 29, 1715–1721. [Google Scholar] [CrossRef]
- Macdonald, J.S.; Fleming, T.R.; Peterson, R.F.; Berenberg, J.L.; McClure, S.; Chapman, R.A.; McClure, S.; Chapman, R.A.; Eyre, H.J.; Solanki, D.; et al. Adjuvant chemotherapy with 5-FU, adriamycin, and mitomycin-C (FAM) versus surgery alone for patients with locally advanced gastric adenocarcinoma: A Southwest Oncology Group study. Ann. Surg. Oncol. 1995, 2, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Hermans, J.; Bonenkamp, J.J.; Boon, M.C.; Bunt, A.M.; Ohymana, S.; Sasako, M.; Van de Velde, C.J. Adjuvant therapy after curative resection for gastric cancer: Meta–analysis of randomized trials. J. Clin. Oncol. 1993, 11, 1441–1447. [Google Scholar] [CrossRef] [PubMed]
- GASTRIC (Global Advanced/Adjuvant Stomach Tumor Research International Collaboration) Group; Paoletti, X.; Oba, K.; Burrykowski, T.; Michiels, S.; Ohashi, Y.; Pignon, J.P.; Rougier, P.; Sakamoto, J.; Sargent, D.; et al. Benefit of adjuvant chemotherapy for resectable gastric cancer: A meta–analysis. JAMA 2010, 503, 1729–1737. [Google Scholar]
- Lee, C.; Jung, M.; Kim, H.S.; Jung, I.; Shin, D.B.; Kang, S.Y.; Zang, D.Y.; Kim, K.H.; Lee, M.H.; Kim, B.S.; et al. S-1 Based Doublet as an Adjuvant Chemotherapy for Curatively Resected Stage III Gastric Cancer: Results From the Randomized Phase III POST Trial. Cancer Res. Treat. 2019, 51, 1–11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al–Batran, S.E.; Homann, N.; Pauligk, C.; Goetze, T.O.; Meiler, J.; Kasper, S.; Kopp, H.G.; Mayer, F.; Haag, G.M.; Luley, K.; et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): A randomised, phase 2/3 trial. The Lancet 2019, 393, 1948–1957. [Google Scholar]
- Luu, C.; Thapa, R.; Woo, K.; Coppola, D.; Almhanna, K.; Pimiento, J.M.; Chen, D.T.; Marquez, D.D.; Hodul, P. Does histology really influence gastric cancer prognosis? J. Gastrointest Oncol. 2017, 8, 1026–1036. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lauren, P. The two histological main types of gastric carcinoma: Diffuse and so-called intestinal-type carcinoma. Acta. Pathol. Microbiol. Scand. 1965, 64, 31–49. [Google Scholar] [CrossRef]
- Bringeland, E.A.; Wasmuth, H.H.; Mjones, P.; Myklebust, T.A.; Gronbech, J.E. A population-based study on incidence rates, Lauren distribution, stage distribution, treatment, and long–term outcomes for gastric adenocarcinoma in Central Norway 2001–2011. Acta. Oncol. 2017, 56, 39–45. [Google Scholar] [CrossRef] [Green Version]
- Tan, I.B.; Ivanova, T.; Lim, K.H.; Ong, C.W.; Deng, N.; Lee, J.; Tan, S.H.; Wu, J.; Lee, M.H.; Ooi, C.H.; et al. Intrinsic subtypes of gastric cancer predict survival and respond differently to chemotherapy. Gastroenterology 2011, 141, 476–485. [Google Scholar] [CrossRef]
- Zheng, H.C.; Zheng, Y.S.; Xia, P.; Xu, X.Y.; Xing, Y.N.; Takahashi, H.; Guan, Y.; Takano, Y. The pathobiological behaviors and prognosis associated with Japanese gastric adenocarcinomas of pure WHO histological subtypes. Histol. Histopathol. 2010, 25, 445–452. [Google Scholar]
- Petrelli, F.; Berenato, R.; Turati, L.; Mennitto, A.; Steccanella, F.; Caporale, M.; Dallera, P.; de Braud, F.; Pezzica, E.; Di Bartolomeo, M.; et al. Prognostic value of diffuse versus intestinal histotype in patients with gastric cancer: A systematic review and meta–analysis. J. Gastrointest Oncol. 2017, 8, 148–163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- The Cancer Genoma Atlas Research Network. Comprehensive molecular characterization of gastric adenocarcinoma. Nature 2014, 513, 202–209. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mandard, A.M.; Dalibard, F.; Mandard, J.C.; Marnay, J.; Henry–Amar, M.; Petiot, J.F.; Roussel, A.; Jacob, J.H.; Segol, P.; Samama, G.; et al. Pathologic assessment of tumor regression after preoperative chemoradiotherapy of esophageal carcinoma. Clinicopathologic correlations. Cancer 1994, 73, 2680–2686. [Google Scholar] [CrossRef]
- Zheng, X.H.; Zhang, W.; Yang, L.; Du, C.X.; Li, N.; Xing, G.S.; Tain, Y.T.; Xie, Y.B. Role of D2 gastrectomy in gastric cancer with clinical para-aortic lymph node metastasis. World J. Gastroenterol. 2019, 25, 2338–2353. [Google Scholar] [CrossRef]
- Smalley, S.R.; Benedetti, J.K.; Haller, D.G.; Hundahi, S.A.; Estes, N.C.; Ajani, J.A.; Gunderson, L.L.; Goldman, B.; Martenson, L.A.; Jessup, M.; et al. Updated analysis of SWOG-directed Intergroup Study 0116: A phase III trial of adjuvant radiochemotherapy versus observation after curative gastric cancer resection. J. Clin. Oncol. 2012, 30, 2327–2333. [Google Scholar] [CrossRef]
- Iwasaki, Y.; Terashima, M.; Mizusawa, J.; Katayama, H.; Nakamura, K.; Katai, H.; Yoshikawa, T.; Ito, Y.; Kaji, M.; Kimura, Y.; et al. Randomized phase III trial of gastrectomy with or without neoadjuvant S–1 plus cisplatin for type 4 or large type 3 gastric cancer: Japan Clinical Oncology Group study (JCOG0501). JCO 2018, 36, 4046. [Google Scholar] [CrossRef]
- Li, Y.; Ma, F.H.; Xue, L.Y.; Tian, Y.T. Neoadjuvant chemotherapy vs upfront surgery for gastric signet ring cell carcinoma: A retrospective, propensity score-matched study. World J. Gastroenterol. 2020, 28, 818–882. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Perioperative Chemotherapy (No. 83) | Characteristic | Adjuvant Chemotherapy (No. 120) | ||||
|---|---|---|---|---|---|---|---|
| No. | Intestinal (No. 44) | Diffuse (No. 39) | No. | Intestinal (No. 46) | Diffuse (No. 74) | ||
| Tumor location | Tumor location | ||||||
| GEJ | 41 | 23 (27.7%) | 18 (21.7%) | GEJ | 28 | 13 (10.8%) | 15 (12.5%) |
| Stomach | 42 | 21 (25.3%) | 21 (25.3%) | Stomach | 92 | 33 (27.5%) | 59 (49.2%) |
| Signet-cell | 9 | - | 9 (10.8%) | Signet-cell | 18 | - | 18 (15.0%) |
| LVI | 25 | 8 (9.6%%) | 17 (20.4%) | LVI | 60 | 23 (19.1%) | 37 (30.8%) |
| Total gastrectomy | 41 | 19 (22.8%) | 22 (26.5%) | Total gastrectomy | 48 | 21 (17.5%) | 27 (32.5%) |
| R1 surgery | 4 | - | 4 (4.8%) | R1 surgery | 4 | - | 4 (3.3%) |
| T | T | ||||||
| yT0/T1 | 8 | 6 (7.2%) | 2 (2.4%) | pT0/T1 | 4 | 1 (0.8%) | 3 (2.5%) |
| yT2 | 16 | 12 (14.5%) | 4 (4.8%) | pT2 | 13 | 6 (5.0%) | 7 (5.9%) |
| yT3 | 38 | 21 (25.3%) | 17 (20.5%) | pT3 | 46 | 18 (15.0%) | 28 (23.3%) |
| yT4 | 21 | 5 (6.0%) | 16 (19.3%) | pT4 | 57 | 21 (17.5%) | 36 (30.0%) |
| N | N | ||||||
| yN0 | 32 | 27 (32.5%) | 5 (6.0%) | pN0 | 6 | 4 (3.3%) | 2 (1.7%) |
| yN1 | 15 | 8 (9.7%) | 7 (8.4%) | pN1 | 24 | 7 (5.8%) | 17 (14.2%) |
| yN2 | 16 | 5 (6.0%) | 11 (13.3%) | pN2 | 32 | 17 (14.2%) | 15 (12.5%) |
| yN3 | 20 | 4 (4.8%) | 16 (19.3%) | pN3 | 58 | 18 (15.0%) | 40 (33.3%) |
| TRG | |||||||
| TRG1 | 7 | 5 (6.0%) | 2 (2.4%) | ||||
| TRG2 | 7 | 7 (8.4%) | - | ||||
| TRG3 | 28 | 17 (20.5%) | 11 (13.3%) | ||||
| TRG4 | 34 | 15 (18.1%) | 19 (22.9%) | ||||
| TRG5 | 7 | - | 7 (8.4%) | ||||
| Treatment | Treatment | ||||||
| EOX/ECF | 51 | 22 (26.5%) | 29 (34.9%) | EOX/ECF | 49 | 14 (11.6%) | 35 (29.2%) |
| FOLFOX/CF | 32 | 22 (26.5%) | 10 (12.1%) | FOLFOX/CF | 32 | 15 (12.5%) | 17 (14.2%) |
| DeGramont | - | - | - | DeGramont | 39 | 17 (14.2%) | 22 (18.3%) |
| Radiotherapy | 24 | 4 (4.8%) | 20 (24.0%) | Radiotherapy | 52 | 18 (15%) | 34 (28.3%) |
| Variable | OS | EFS | ||
|---|---|---|---|---|
| HR (95% CI) for Mortality | p Value | HR (95% CI) for Progression | p Value | |
| pCT cohort | ||||
| Age | 0.6 (0.3–1.22) | 0.1 | 0.4 (0.21–0.82) | 0.01 |
| Grading | 2.7 (1.31–5.68) | 0.004 | 3.2 (1.5–6.5) | 0.0003 |
| Histology | 0.1 (0.05–0.21) | <0.0001 | 0.13 (0.07–0.27) | <0.0001 |
| LVI | 3.6 (1.55–8.34) | 0.0001 | 3.8 (1.72–8.62) | <0.0001 |
| Surgery R1 | 3.4 (0.71–16.9) | 0.006 | 3.59 (0.71–18.0) | 0.004 |
| Tumor location | 1.2 (0.61–2.53) | 0.53 | 1.16 (0.59–2.26) | 0.65 |
| N status | 4.71 (2.30–9.65) | 0.0012 | 3.66 (1.87–7.15) | 0.0017 |
| Doublet vs. triplet chemotherapy | 1.28 (0.64–2.54) | 0.48 | 1.22 (0.58–2.58) | 0.5 |
| Radiotherapy | 1.99 (0.91–4.1) | 0.06 | 1.7 (0.86–3.68) | 0.08 |
| aCT cohort | ||||
| Age | 1.70 (0.95–3.02) | 0.06 | 1.48 (0.87–2.54) | 0.12 |
| Grading | 1.31 (0.73–2.36) | 0.37 | 1.45 (0.83–2.52) | 0.19 |
| Histology | 1.28 (0.72–2.26) | 0.40 | 1.12 (0.65–1.91) | 0.67 |
| LVI | 1.31 (0.70–2.43) | 0.66 | 1.13 (0.63–2.0) | 0.66 |
| Surgery R1 | 4.04 (0.58–27.9) | 0.0033 | 13.2(0.61–28.01) | <0.0001 |
| Tumor location | 0.59 (0.29–1.21) | 0.09 | 0.55 (0.28–1.07) | 0.03 |
| N status | 1.5 (0.29–7.67) | 0.68 | 2.03 (0.49–8.34) | 0.46 |
| Doublet vs. triplet chemotherapy | 1.11 (0.60–2.03) | 0.72 | 1.16 (0.66–2.05) | 0.57 |
| Radiotherapy | 1.42 (0.82–2.47) | 0.19 | 1.44 (0.85–2.42) | 0.16 |
| Variable | OS | EFS | ||
|---|---|---|---|---|
| HR (95% CI) for Progression | p Value | HR (95% CI) for Mortality | p Value | |
| pCT | ||||
| Histology | 10.95 (3.31–36.24) | 0.0001 | 4.84 (1.76–13.29) | 0.0023 |
| LVI | 5.57 (2.18–14.26) | 0.0004 | 3.60 (1.56–8.32) | 0.0028 |
| aCT | ||||
| Tumor location | – | – | 0.47 (0.26–0.85) | 0.013 |
| Resection margin | 19.97 (7.04–56.59) | <0.001 | 4.036 (1.44–11.30) | 0.0082 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zurlo, I.V.; Basso, M.; Strippoli, A.; Calegari, M.A.; Orlandi, A.; Cassano, A.; Di Salvatore, M.; Garufi, G.; Bria, E.; Tortora, G.; et al. Treatment of Locally Advanced Gastric Cancer (LAGC): Back to Lauren’s Classification in Pan–Cancer Analysis Era? Cancers 2020, 12, 1749. https://doi.org/10.3390/cancers12071749
Zurlo IV, Basso M, Strippoli A, Calegari MA, Orlandi A, Cassano A, Di Salvatore M, Garufi G, Bria E, Tortora G, et al. Treatment of Locally Advanced Gastric Cancer (LAGC): Back to Lauren’s Classification in Pan–Cancer Analysis Era? Cancers. 2020; 12(7):1749. https://doi.org/10.3390/cancers12071749
Chicago/Turabian StyleZurlo, Ina Valeria, Michele Basso, Antonia Strippoli, Maria Alessandra Calegari, Armando Orlandi, Alessandra Cassano, Mariantonietta Di Salvatore, Giovanna Garufi, Emilio Bria, Giampaolo Tortora, and et al. 2020. "Treatment of Locally Advanced Gastric Cancer (LAGC): Back to Lauren’s Classification in Pan–Cancer Analysis Era?" Cancers 12, no. 7: 1749. https://doi.org/10.3390/cancers12071749