Phase I Study of Carbon Ion Radiotherapy and Image-Guided Brachytherapy for Locally Advanced Cervical Cancer

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility
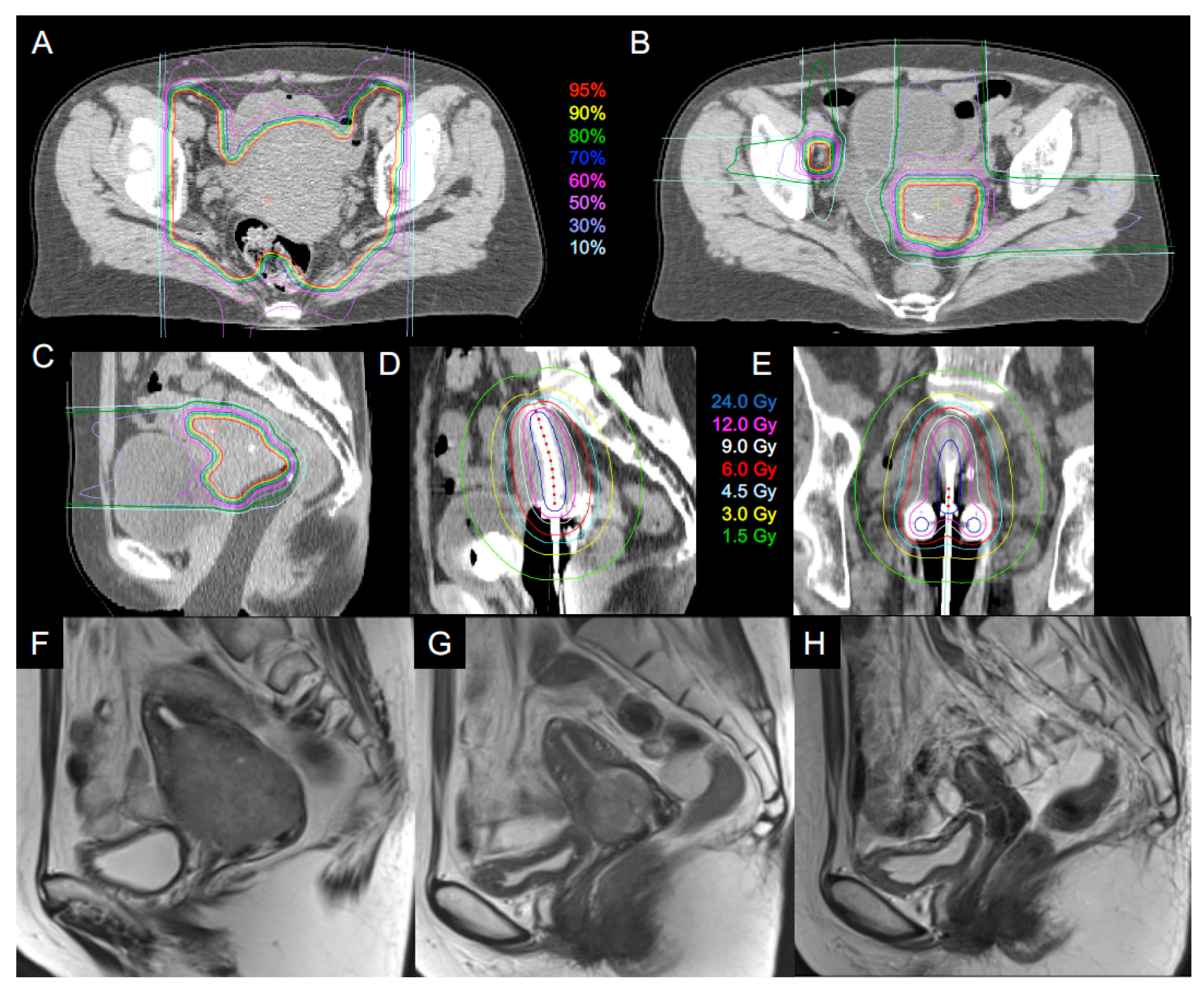
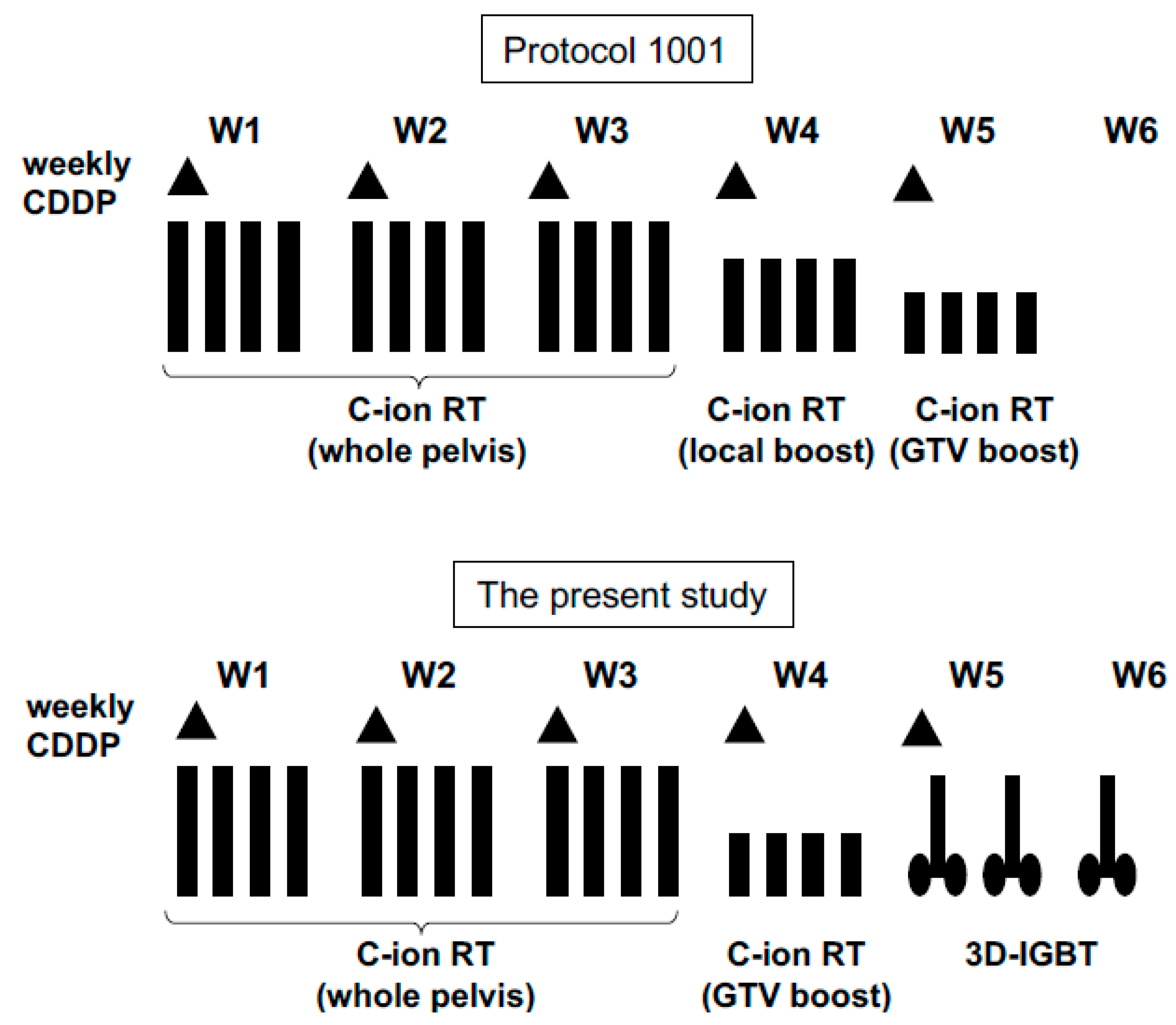
2.2. Carbon Ion Radiotherapy
2.3. Image-Guided Brachytherapy
2.4. Cumulative Dose Calculation
2.5. Chemotherapy
2.6. Study Design
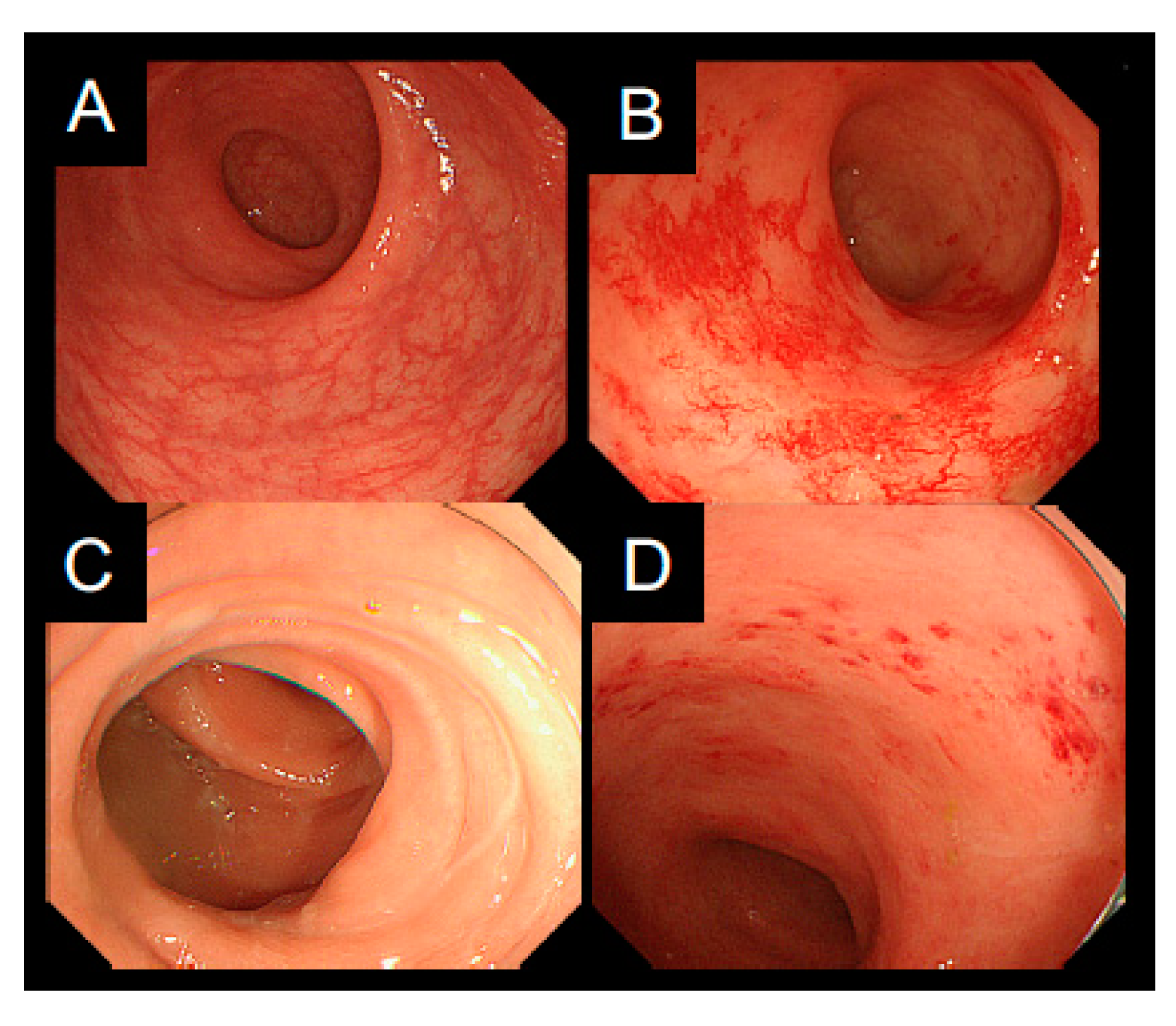
2.7. Evaluation of Safety and Efficacy
3. Results
3.1. Patient Characteristics
3.2. Safety
3.3. Efficacy
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| C-ion RT | carbon ion radiotherapy |
| 3D-IGBT | 3D image-guided brachytherapy |
| DLT | dose-limiting toxicities |
| RBE | relative biological effectiveness |
| EQD2 | equivalent dose of 2 Gy per fraction |
| CCRT | concurrent chemoradiotherapy |
| EBRT | external beam radiotherapy |
| DVH | dose-volume histogram |
| CTVHR | high-risk clinical target volume |
| LET | linear energy transfer |
| RD | recommended dose |
| FIGO | International Federation of Gynecology and Obstetrics |
| CT | computed tomography |
| MRI | magnetic resonance imaging |
| GTV | gross tumor volume |
| CTV | clinical target volume |
| iCTVWP | internal clinical target volume with whole pelvis |
| PTVWP | planning target volume with whole pelvis |
| CTVCX | CTV with cervix |
| CTVLN | CTV with positive lymph node |
| OARs | organs at risk |
| VRS | Vienna Rectoscopy Score |
References
- Haie-Meder, C.; Pötter, R.; Van Limbergen, E.; Barillot, I.; De Brabandere, M.; Dimopoulos, J.; Dumas, I.; Erickson, B.; Lang, S.; Nulens, A.; et al. Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group (I): Concepts and terms in 3D image-based 3D treatment planning in cervix cancer brachytherapy with emphasis on MRI assessment of GTV and CTV. Radiother. Oncol. 2005, 74, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Pötter, R.; Haie-Meder, C.; Van Limbergen, E.; Barillot, I.; De Brabandere, M.; Dimopoulos, J.; Dumas, I.; Erickson, B.; Lang, S.; Nulens, A.; et al. Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group (II): Concepts and terms in 3D image-based treatment planning in cervix cancer brachytherapy–3D dose volume parameters and aspects of 3D image-based anatomy, radiation physics, and radiobiology. Radiother. Oncol. 2006, 78, 67–77. [Google Scholar] [PubMed]
- Pötter, R.; Georg, P.; Dimopoulos, J.C.; Grimm, M.; Berger, D.; Nesvacil, N.; Georg, D.; Schmid, M.P.; Reinthaller, A.; Sturdza, A.; et al. Clinical outcome of protocol based image (MRI) guided adaptive brachytherapy combined with 3D conformal radiotherapy with or without chemotherapy in patients with locally advanced cervical cancer. Radiother. Oncol. 2011, 100, 116–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rijkmans, E.C.; Nout, R.A.; Rutten, I.H.; Ketelaars, M.; Neelis, K.J.; Laman, M.S.; Coen, V.L.; Gaarenstroom, K.N.; Kroep, J.R.; Creutzberg, C.L. Improved survival of patients with cervical cancer treated with image-guided brachytherapy compared with conventional brachytherapy. Gynecol. Oncol. 2014, 135, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Ohno, T.; Noda, S.E.; Okonogi, N.; Murata, K.; Shibuya, K.; Kiyohara, H.; Tamaki, T.; Ando, K.; Oike, T.; Ohkubo, Y.; et al. In-room computed tomography-based brachytherapy for uterine cervical cancer: Results of a 5-year retrospective study. J. Radiat. Res. 2017, 58, 543–551. [Google Scholar] [CrossRef] [PubMed]
- Minkoff, D.; Gill, B.S.; Kang, J.; Beriwal, S. Cervical cancer outcome prediction to high-dose rate brachytherapy using quantitative magnetic resonance imaging analysis of tumor response to external beam radiotherapy. Radiother. Oncol. 2015, 115, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Mazeron, R.; Castelnau-Marchand, P.; Dumas, I.; del Campo, E.R.; Kom, L.K.; Martinetti, F.; Farha, G.; Tailleur, A.; Morice, P.; Chargari, C.; et al. Impact of treatment time and dose escalation on local control in locally advanced cervical cancer treated by chemoradiation and image-guided pulsed-dose rate adaptive brachytherapy. Radiother. Oncol. 2015, 114, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Kusada, T.; Toita, T.; Ariga, T.; Maemoto, H.; Hashimoto, S.; Shiina, H.; Kakinohana, Y.; Heianna, J.; Nagai, Y.; Kudaka, W.; et al. Computed tomography-based image-guided brachytherapy for cervical cancer: Correlations between dose-volume parameters and clinical outcomes. J. Radiat. Res. 2018, 59, 67–76. [Google Scholar] [CrossRef] [PubMed]
- Kamada, T.; Tsujii, H.; Blakely, E.A.; Debus, J.; De Neve, W.; Durante, M.; Jäkel, O.; Mayer, R.; Orecchia, R.; Pötter, R.; et al. Carbon ion radiotherapy in Japan: An assessment of 20 years of clinical experience. Lancet Oncol. 2015, 16, e93–e100. [Google Scholar] [CrossRef]
- Durante, M.; Orecchia, R.; Loeffler, J.S. Charged-particle therapy in cancer: Clinical uses and future perspectives. Nat. Rev. Clin. Oncol. 2017, 14, 483–495. [Google Scholar] [CrossRef] [PubMed]
- Nakano, T.; Suzuki, M.; Abe, A.; Suzuki, Y.; Morita, S.; Mizoe, J.; Sato, S.; Miyamoto, T.; Kamada, T.; Kato, H.; et al. The phase I/II clinical study of carbon ion therapy for cancer of the uterine cervix. Cancer J. Sci. Am. 1999, 5, 362–369. [Google Scholar] [PubMed]
- Kato, S.; Ohno, T.; Tsujii, H.; Nakano, T.; Mizoe, J.E.; Kamada, T.; Miyamoto, T.; Tsuji, H.; Kato, H.; Yamada, S.; et al. Dose escalation study of carbon ion radiotherapy for locally advanced carcinoma of the uterine cervix. Int. J. Radiat. Oncol. Biol. Phys. 2006, 65, 388–397. [Google Scholar] [CrossRef] [PubMed]
- Wakatsuki, M.; Kato, S.; Ohno, T.; Karasawa, K.; Ando, K.; Kiyohara, H.; Tsujii, H.; Nakano, T.; Kamada, T.; Shozu, M.; et al. Dose-escalation study of carbon ion radiotherapy for locally advanced squamous cell carcinoma of the uterine cervix (9902). Gynecol. Oncol. 2014, 132, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Wakatsuki, M.; Kato, S.; Kiyohara, H.; Ohno, T.; Karasawa, K.; Tamaki, T.; Ando, K.; Tsujii, H.; Nakano, T.; Kamada, T.; et al. Clinical trial of prophylactic extended-field carbon-ion radiotherapy for locally advanced uterine cervical cancer (protocol 0508). PLoS ONE 2015, 10, e0127587. [Google Scholar] [CrossRef]
- Wakatsuki, M.; Kato, S.; Ohno, T.; Karasawa, K.; Kiyohara, H.; Tamaki, T.; Ando, K.; Tsujii, H.; Nakano, T.; Kamada, T.; et al. Clinical outcomes of carbon ion radiotherapy for locally advanced adenocarcinoma of the uterine cervix in phase 1/2 clinical trial (protocol 9704). Cancer 2014, 120, 1663–1669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Okonogi, N.; Wakatsuki, M.; Kato, S.; Karasawa, K.; Kiyohara, H.; Shiba, S.; Kobayashi, D.; Nakano, T.; Kamada, T.; Shozu, M.; et al. Clinical outcomes of carbon ion radiotherapy with concurrent chemotherapy for locally advanced uterine cervical adenocarcinoma in a phase 1/2 clinical trial (Protocol 1001). Cancer Med. 2018, 7, 351–359. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ohno, T.; Kanai, T.; Yamada, S.; Yusa, K.; Tashiro, M.; Shimada, H.; Torikai, K.; Yoshida, Y.; Kitada, Y.; Katoh, H.; et al. Carbon ion radiotherapy at the Gunma University Heavy Ion Medical Center: New facility set-up. Cancers 2011, 3, 4046–4060. [Google Scholar] [CrossRef] [PubMed]
- Kanai, T.; Endo, M.; Minohara, S.; Miyahara, N.; Koyama-ito, H.; Tomura, H.; Matsufuji, N.; Futami, Y.; Fukumura, A.; Hiraoka, T.; et al. Biophysical characteristics of HIMAC clinical irradiation system for heavy-ion radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 1999, 44, 201–210. [Google Scholar] [CrossRef]
- Ohno, T.; Wakatsuki, M.; Toita, T.; Kaneyasu, Y.; Yoshida, K.; Kato, S.; Ii, N.; Tokumaru, S.; Ikushima, H.; Uno, T.; et al. Recommendations for high-risk clinical target volume definition with computed tomography for three-dimensional image-guided brachytherapy in cervical cancer patients. J. Radiat. Res. 2017, 58, 341–350. [Google Scholar] [CrossRef] [PubMed]
- Wachter, S.; Gerstner, N.; Goldner, G.; Pötzi, R.; Wambersie, A.; Pötter, R. Endoscopic scoring of late rectal mucosal damage after conformal radiotherapy for prostatic carcinoma. Radiother. Oncol. 2000, 54, 11–19. [Google Scholar] [CrossRef]
- Mundt, A.J.; Lujan, A.E.; Rotmensch, J.; Waggoner, S.E.; Yamada, S.D.; Fleming, G.; Roeske, J.C. Intensity-modulated whole pelvic radiotherapy in women with gynecologic malignancies. Int. J. Radiat. Oncol. Biol. Phys. 2002, 52, 1330–1337. [Google Scholar] [CrossRef]
- Gandhi, A.K.; Sharma, D.N.; Rath, G.K.; Julka, P.K.; Subramani, V.; Sharma, S.; Manigandan, D.; Laviraj, M.A.; Kumar, S.; Thulkar, S. Early clinical outcomes and toxicity of intensity modulated versus conventional pelvic radiation therapy for locally advanced cervix carcinoma: A prospective randomized study. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Koom, W.S.; Sohn, D.K.; Kim, J.Y.; Kim, J.W.; Shin, K.H.; Yoon, S.M.; Kim, D.Y.; Yoon, M.; Shin, D.; Park, S.Y.; et al. Computed tomography-based high-dose-rate intracavitary brachytherapy for uterine cervical cancer: Preliminary demonstration of correlation between dose-volume parameters and rectal mucosal changes observed by flexible sigmoidoscopy. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 1446–1454. [Google Scholar] [CrossRef] [PubMed]
- Ippolito, E.; Massaccesi, M.; Digesù, C.; Deodato, F.; Macchia, G.; Pirozzi, G.A.; Cilla, S.; Cuscunà, D.; Di Lallo, A.; Mattiucci, G.C.; et al. Early proctoscopy is a surrogate endpoint of late rectal toxicity in prostate cancer treated with radiotherapy. Int. J. Radiat. Oncol. Biol. Phys. 2012, 83, e191–e195. [Google Scholar] [CrossRef] [PubMed]
- Wakatsuki, M.; Ohno, T.; Yoshida, D.; Noda, S.E.; Saitoh, J.; Shibuya, K.; Katoh, H.; Suzuki, Y.; Takahashi, T.; Nakano, T. Intracavitary combined with CT-guided interstitial brachytherapy for locally advanced uterine cervical cancer: Introduction of the technique and a case presentation. J. Radiat. Res. 2011, 52, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Oike, T.; Niimi, A.; Okonogi, N.; Murata, K.; Matsumura, A.; Noda, S.E.; Kobayashi, D.; Iwanaga, M.; Tsuchida, K.; Kanai, T.; et al. Visualization of complex DNA double-strand breaks in a tumor treated with carbon ion radiotherapy. Sci. Rep. 2016, 6, 22275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nakano, T.; Suzuki, Y.; Ohno, T.; Kato, S.; Suzuki, M.; Morita, S.; Sato, S.; Oka, K.; Tsujii, H. Carbon beam therapy overcomes the radiation resistance of uterine cervical cancer originating from hypoxia. Clin. Cancer Res. 2006, 12, 2185–2190. [Google Scholar] [CrossRef] [PubMed]
- Jadon, R.; Pembroke, C.A.; Hanna, C.L.; Palaniappan, N.; Evans, M.; Cleves, A.E.; Staffurth, J. A systematic review of organ motion and image-guided strategies in external beam radiotherapy for cervical cancer. Clin. Oncol. (R. Coll. Radiol.) 2014, 26, 185–196. [Google Scholar] [CrossRef] [PubMed]
- Jensen, A.D.; Nikoghosyan, A.V.; Lossner, K.; Haberer, T.; Jäkel, O.; Münter, M.W.; Debus, J. COSMIC: A regimen of intensity modulated radiation therapy plus dose-escalated, raster-scanned carbon ion boost for malignant salivary gland tumors: Results of the prospective phase 2 trial. Int. J. Radiat. Oncol. Biol. Phys. 2015, 93, 37–46. [Google Scholar] [CrossRef] [PubMed]
- Jensen, A.D.; Krauss, J.; Potthoff, K.; Desta, A.; Habl, G.; Mavtratzas, A.; Windemuth-Kiesselbach, C.; Debus, J.; Münter, M.W. Phase II study of induction chemotherapy with TPF followed by radioimmunotherapy with Cetuximab and intensity-modulated radiotherapy (IMRT) in combination with a carbon ion boost for locally advanced tumours of the oro-, hypopharynx and larynx-TPF-C-HIT. BMC Cancer 2011, 11, 182. [Google Scholar] [CrossRef] [PubMed]
- Brahme, A. Recent advances in light ion radiation therapy. Int. J. Radiat. Oncol. Biol. Phys. 2004, 58, 603–616. [Google Scholar] [CrossRef] [PubMed]
- Brahme, A. Potential developments of light ion therapy: The ultimate conformal treatment modality. Radiol. Sci. 2009, 52, 8–31. [Google Scholar]




{kind=link}
{kind=link}
{kind=link}
| Patient Number | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| Age | 45 | 44 | 47 | 56 | 57 | 64 |
| Histology | SCC | SCC | Ad | Ad | Ad | Ad |
| FIGO stage | IIB | IIIB | IIB | IIB | IIB | IIB |
| Cervical tumor size (cm) | 5.7 | 6 | 5.7 | 4.2 | 6.4 | 4.8 |
| Pelvic lymph node | Positive | Negative | Negative | Negative | Positive | Positive |
| Cisplatin (course) | 5 | 5 | 5 | 5 | 5 | 5 |
| C-ion RT (Gy (RBE)/fr) | 55.2/16 | 55.2/16 | 55.2/16 | 55.2/16 | 55.2/16 | 55.2/16 |
| Brachytherapy (session) | 3 | 3 | 3 | 3 | 3 | 3 |
| Overall treatment | 34 | 37 | 34 | 35 | 34 | 37 |
| time (days) |
| Patient Number | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| Carbon ion radiotherapy EQD2 (Gy (RBE)) | ||||||
| Rectosigmoid D2cc | 47.8 | 44.2 | 43.2 | 44.7 | 45.9 | 45.6 |
| Bladder D2cc | 50.4 | 73.2 | 70.9 | 70.9 | 71.9 | 72.0 |
| CTVHR D90 | 49.7 | 61.3 | 61.5 | 62.7 | 53.6 | 45.6 |
| Brachytherapy EQD2 (Gy) | ||||||
| Rectosigmoid D2cc | 22.9 | 25.7 | 25.0 | 23.4 | 23.7 | 24.6 |
| Bladder D2cc | 29.8 | 40.1 | 26.6 | 40.9 | 26.3 | 19.1 |
| CTVHR D90 | 30.7 | 28.9 | 28.6 | 36.4 | 30.1 | 22.3 |
| Total EQD2 (Gy, Gy (RBE)) | ||||||
| Rectosigmoid D2cc | 70.7 | 69.9 | 68.2 | 68.1 | 69.6 | 70.2 |
| Bladder D2cc | 80.2 | 113.3 | 97.5 | 111.8 | 98.2 | 91.1 |
| CTVHR D90 | 80.4 | 90.2 | 90.1 | 99.1 | 83.7 | 67.9 |
| Toxicity | Grade | ||||
|---|---|---|---|---|---|
| 0 | 1 | 2 | 3 | 4 | |
| Acute hematological toxicities | |||||
| White blood cell | 0 | 1 | 4 | 1 | 0 |
| Neutrophil | 0 | 5 | 0 | 1 | 0 |
| Hemoglobin | 0 | 6 | 0 | 0 | 0 |
| Platelet | 0 | 1 | 1 | 0 | 0 |
| Acute non-hematological toxicities | |||||
| Upper GI tract | 3 | 3 | 0 | 0 | 0 |
| Lower GI tract | 3 | 1 | 0 | 0 | 0 |
| Genitourinary tract | 5 | 1 | 0 | 0 | 0 |
| Skin | 4 | 2 | 0 | 0 | 0 |
| Late toxicities | |||||
| Lower GI tract | 2 | 3 | 0 | 1 | 0 |
| Genitourinary tract | 5 | 0 | 1 | 0 | 0 |
| Patient Number | DLT | Disease Status at the Time of Last Follow-Up | OS (months) | PFS (months) | First Failure Site |
|---|---|---|---|---|---|
| 1 | None | DOD | 24 | 3 | Paraaortic lymph node |
| 2 | None | NED | 52 | 52 | |
| 3 | None | AWD | 50 | 21 | Lung |
| 4 | None | AWD | 50 | 7 | Lung |
| 5 | None | NED | 45 | 45 | |
| 6 | None | NED | 45 | 15 | Left iliac lymph node |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ohno, T.; Noda, S.-e.; Murata, K.; Yoshimoto, Y.; Okonogi, N.; Ando, K.; Tamaki, T.; Kato, S.; Hirakawa, T.; Kanuma, T.; et al. Phase I Study of Carbon Ion Radiotherapy and Image-Guided Brachytherapy for Locally Advanced Cervical Cancer. Cancers 2018, 10, 338. https://doi.org/10.3390/cancers10090338
Ohno T, Noda S-e, Murata K, Yoshimoto Y, Okonogi N, Ando K, Tamaki T, Kato S, Hirakawa T, Kanuma T, et al. Phase I Study of Carbon Ion Radiotherapy and Image-Guided Brachytherapy for Locally Advanced Cervical Cancer. Cancers. 2018; 10(9):338. https://doi.org/10.3390/cancers10090338
Chicago/Turabian StyleOhno, Tatsuya, Shin-ei Noda, Kazutoshi Murata, Yuya Yoshimoto, Noriyuki Okonogi, Ken Ando, Tomoaki Tamaki, Shingo Kato, Takashi Hirakawa, Tatsuya Kanuma, and et al. 2018. "Phase I Study of Carbon Ion Radiotherapy and Image-Guided Brachytherapy for Locally Advanced Cervical Cancer" Cancers 10, no. 9: 338. https://doi.org/10.3390/cancers10090338