
Abstract
Background
Permanent paraffin subareolar biopsy during nipple-sparing mastectomy (NSM) tests for occult cancer at the nipple-areolar complex. Intraoperative subareolar frozen section can provide earlier detection intraoperatively. Cost analysis for intraoperative subareolar frozen section has never been performed.
Methods
NSM cases from 2006–2013 were reviewed. Patient records including financial charges were analyzed.
Results
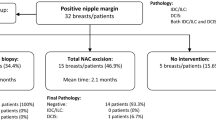
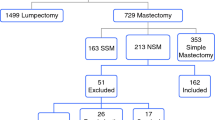
Of 480 subareolar biopsies for NSM from 2006–2013, 21 were abnormal (4.4 %). A total of 307 of the subareolar biopsies included intraoperative frozen section. Of the 307, 12 (3.9 %) were abnormal with 7 of 12 detected on intraoperative frozen section. The median baseline charge for an intraoperative subareolar frozen section was $309 for an estimated total cost of $94,863 in 307 breasts. The median baseline charge for interval operative resection of a nipple-areolar complex following an abnormal subareolar pathology result was $11,021. Intraoperative subareolar biopsy avoided an estimated six return trips to the operating room for savings of $66,126. At our institution, routine use of intraoperative frozen section resulted in an additional $28,737 in healthcare charges or $95 per breast.
Conclusions
We present the first cost analysis to evaluate intraoperative subareolar frozen section in NSM. This practice obviated an estimated six return trips to the operating room. With our institutional frequency of abnormal subareolar pathology, intraoperative frozen sections resulted in a marginal increased charge per mastectomy.
Similar content being viewed by others

References
Adam H, Bygdeson M, de Boniface J. The oncological safety of nipple-sparing mastectomy—a Swedish matched cohort study. Eur J Surg Oncol. 2014;40(10):1209–15.
Freeman BS. Technique of subcutaneous mastectomy with replacement; immediate and delayed. Br J Plast Surg. 1969;22(2):161–6.
Hartmann LC, Schaid DJ, Woods JE, et al. Efficacy of bilateral prophylactic mastectomy in women with a family history of breast cancer. N Engl J Med. 1999;340(2):77–84.
Hinton CP, Doyle PJ, Blamey RW, Davies CJ, Holliday HW, Elston CW. Subcutaneous mastectomy for primary operable breast cancer. Br J Surg. 1984;71(6):469–72.
Kissin MW, Kark AE. Nipple preservation during mastectomy. Br J Surg. 1987;74(1):58–61.
Luo D, Ha J, Latham B, et al. The accuracy of intraoperative subareolar frozen section in nipple-sparing mastectomies. Ochsner J. 2010;10(3):188–92.
Schecter AK, Freeman MB, Giri D, Sabo E, Weinzweig J. Applicability of the nipple-areola complex-sparing mastectomy: a prediction model using mammography to estimate risk of nipple-areola complex involvement in breast cancer patients. Ann Plast Surg. 2006;56(5):498–504.
Vyas JJ, Chinoy RF, Vaidya JS. Prediction of nipple and areola involvement in breast cancer. Eur J Surg Oncol. 1998;24(1):15–6.
Rusby JE, Brachtel EF, Othus M, Michaelson JS, Koerner FC, Smith BL. Development and validation of a model predictive of occult nipple involvement in women undergoing mastectomy. Br J Surg. 2008;95(11):1356–61.
Spear SL, Willey SC, Feldman ED, et al. Plast Reconstr Surg. 2011;128(5):1005–14.
de AlcantaraFilho P, Capko D, Barry JM, Morrow M, Pusic A, Sacchini VS. Nipple-sparing mastectomy for breast cancer and risk-reducing surgery: the Memorial Sloan-Kettering Cancer Center experience. Ann Surg Oncol. 2011;18(11):3117–22.
Crowe JP, Patrick RJ, Yetman RJ, Djohan R. Nipple-sparing mastectomy update: one hundred forty-nine procedure and clinical outcomes. Arch Surg. 2008;143(11):1106.
Petit JY, Veronesi U, Orecchia R, et al. Nipple sparing mastectomy with nipple areola intraoperative radiotherapy: one thousand and one cases of a five years experience at the European institute of oncology of Milan (EIO). Breast Cancer Res Treat. 2009;117(2):333-8.
Stolier A, Stone JC, Moroz K, et al. A comparison of clinical and pathologic assessments for the prediction of occult nipple involvement in nipple-sparing mastectomies. Ann Surg Oncol. 2013;20(1):128–32.
Chamberlain RS, Patil S, Minja EJ, Kordears K IV. Does residents’ involvement in mastectomy cases increase operative cost? If so, who should bear the cost? J Surg Res. 2012;178(1):18–27.
Coopey SB, Tang R, Lei L, et al. Increasing eligibility for nipple-sparing mastectomy. Ann Surg Oncol. 2013;20(10):3218–22.
Colwell AS, Tessler O, Lin AM, et al. Breast reconstruction following nipple-sparing mastectomy: predictors of complications, reconstruction outcomes, and 5-year trends. Plast Reconstr Surg. 2014;133(3):495–506.
Peled AW, Foster RD, Stover AC, et al. Outcomes after total skin-sparing mastectomy and immediate reconstruction in 657 breasts. Ann Surg Oncol. 2012;19(11):3402–9.
Spear SL, Rottman SJ, Seiboth LA, Hannan CM. Breast reconstruction using a staged nipple-sparing mastectomy following mastopexy or reduction. Plast Reconstr Surg. 2012;129(3):572–81.
Deshmukh AA, Cantor SB, Crosby MA, et al. Cost of contralateral prophylactic mastectomy. Ann Surg Oncol. 2014;21(9):2823-30.
Disclosure
None of the authors in this study have any financial interest in any of the products, devices, or drugs mentioned in this manuscript.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Alperovich, M., Reis, S.M., Choi, M. et al. Cost Analysis of Intraoperative Subareolar Frozen Section During Nipple-Sparing Mastectomy. Ann Surg Oncol 23, 490–493 (2016). https://doi.org/10.1245/s10434-015-4882-8
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-015-4882-8