
Abstract
Background
Nipple-sparing mastectomy (NSM) for both risk reduction and cancer is increasing. In the cancer setting, most studies suggest the use of both clinical and intraoperative biopsy criteria in patient selection. This study examines the use of both biopsy and clinical criteria in women undergoing total nipple-removing mastectomy.
Methods
The study consisted of 58 patients undergoing total mastectomy without nipple sparing. Biopsies of the subareola tissue (SA), proximal nipple (NC) contents and radial sections of the residual nipple (NR) were examined microscopically. Tumor size and distance from the nipple were also noted.
Results
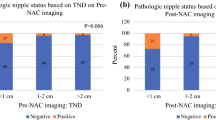
Using clinical criteria alone, the false negative rate was 53.8 % and a false positive rate of 44.4 %. When adding subareola and nipple core biopsies to clinical criteria the false negative rate fell to 7.7 % but the false positive rate remained at 44.4 %. When using only SA and NC biopsies to predict occult nipple involvement, the false negative rate was 11.8 %. In 4 cases the NC was positive while the SA was negative for cancer and in 6 cases the SA was positive and NC negative. In 2 cases both the NC and SA biopsies were negative while the NR was positive.
Conclusions
This study supports a more limited role in the use of clinical criteria for evaluating patients for NSM. This maximizes the number of patients who are candidates for NSM with minimal risk of nipple involvement. It was also noted that intraoperative biopsies are not totally reliable in predicting occult nipple involvement.

Similar content being viewed by others

References
Dao TN, Verheyden CN. TRAM flaps: a reconstructive option after bilateral nipple-sparing total mastectomy. Plast Reconstr Surg. 2005;116:986–92.
Mosahebi A, Ramakrishnan V, Gittos M, Collier J. Aesthetic outcome of different techniques of reconstruction following nipple-areola-preserving envelope mastectomy with immediate reconstruction. Plast Reconstr Surg. 2007;119:796–3.
Didier F, Radice D, Gandini S, et al. Does nipple preservation in mastectomy improve satisfaction with cosmetic results, psychological adjustment, body image and sexuality? Breast Cancer Res Treat. 2009;118:623–33.
Petit JY, Veronesi U, Orecchia R, et al. Nipple-sparing mastectomy in association with intraoperative radiotherapy (ELIOT): A new type of mastectomy for breast cancer treatment. Breast Cancer Res Treat. 2006;96:47–51.
de Alcantara Filho P, Capko D, Barry JM, Morrow M, Pusic A, Sacchini VS. Nipple-sparing mastectomy for breast cancer and risk-reducing surgery: the Memorial Sloan-Kettering Cancer Center experience. Ann Surg Oncol. 2011;18:3117–22.
Spear SL, Hannan CM, Willey SC, Cocilovo C. Nipple-sparing mastectomy. Plast Reconstr Surg. 2009;123:1665–73.
Petit JY, Veronesi U, Orecchia R, et al. Nipple-sparing mastectomy with nipple areola intraoperative radiotherapy: one thousand and one cases of a five years experience at the European institute of oncology of Milan (EIO). Breast Cancer Res Treat. 2009;117:333-8.
Crowe JP, Patrick RJ, Yetman RJ, Djohan R. Nipple-sparing mastectomy update: one hundred forty-nine procedures and clinical outcomes. Arch Surg. 2008;143:1106–10; discussion 1110.
Gerber B, Krause A, Dieterich M, Kundt G, Reimer T. The oncological safety of skin sparing mastectomy with conservation of the nipple-areola complex and autologous reconstruction: an extended follow-up study. Ann Surg. 2009;249:461–8.
Wijayanayagam A, Kumar AS, Foster RD, Esserman LJ. Optimizing the total skin-sparing mastectomy. Arch Surg. 2008;143:38–45; discussion 45.
Caruso F, Ferrara M, Castiglione G et al. Nipple sparing subcutaneous mastectomy: sixty-six months follow-up. Eur J Surg Oncol. 2006;32:937–40.
Sakamoto N, Fukuma E, Higa K, et al. Early results of an endoscopic nipple-sparing mastectomy for breast cancer. Ann Surg Oncol. 2009;16:3406–13.
Rivolin A, Kubatzki F, Marocco F, et al. Nipple-areola complex sparing mastectomy with periareolar pexy for breast cancer patients with moderately ptotic breasts. J Plast Reconstr Aesthet Surg. 2011;65:296–3.
Lambert PA, Kolm P, Perry RR. Parameters that predict nipple involvement in breast cancer. J Am Coll Surg. 2000;191:354–9.
Laronga C, Kemp B, Johnston D, Robb GL, Singletary SE. The incidence of occult nipple-areola complex involvement in breast cancer patients receiving a skin-sparing mastectomy. Ann Surg Oncol. 1999;6:609–13.
Pirozzi PR, Rossetti C, Carelli I, Ruiz CA, Pompei LM, Piato S. Clinical and morphological factors predictive of occult involvement of the nipple-areola complex in mastectomy specimens. Eur J Obstet Gynecol Reprod Biol. 2010;48:177–81.
Rusby JE, Brachtel EF, Othus M, Michaelson JS, Koerner FC, Smith BL. Development and validation of a model predictive of occult nipple involvement in women undergoing mastectomy. Br J Surg. 2008;95:1356–61.
Smith J, Payne WS, Carney JA. Involvement of the nipple and areola in carcinoma of the breast. Surg Gynecol Obstet. 1976;143:546–8.
Wang SY, Peng DF, Cai ZG, et al. [Clinicopathologic analysis of the nipple-areolar complex occult involvement in early stage breast carcinoma]. Zhonghua Zhong Liu Za Zhi. 2008;30:203–6.
Weidong L, Shuling W, Xiaojing G et al. Nipple involvement in breast cancer: retrospective analysis of 2323 consecutive mastectomy specimens. Int J Surg Pathol. 2011;19:328–34.
Kissen MW. Nipple preservation during mastectomy. Br J Surg. 1987;74:58–61.
Brachtel EF, Rusby JE, Michaelson JS et al. Occult nipple involvement in breast cancer: clinicopathologic findings in 316 consecutive mastectomy specimens. J Clin Oncol. 2009;27:4948–54.
Disclosure
The authors have no commercial interests to disclose.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Stolier, A., Stone, J.C., Moroz, K. et al. A Comparison of Clinical and Pathologic Assessments for the Prediction of Occult Nipple Involvement in Nipple-Sparing Mastectomies. Ann Surg Oncol 20, 128–132 (2013). https://doi.org/10.1245/s10434-012-2511-3
Received:
Published:
Issue Date:
DOI: https://doi.org/10.1245/s10434-012-2511-3