
Abstract
Objective
This study aimed to evaluate and compare sizes, shapes and bridging of the sella turcica (ST) in Yemeni individuals with different skeletal patterns, genders, and ages, and to assess the association between the linear dimension of ST and gender, age, or skeletal patterns. The standard anatomical structure of ST among Yemeni subjects is still unknown and this study can be considered as the first reference regarding ST of Yemeni individuals.
Materials and methods
Cephalogram images for 234 subjects (167 females and 67 males) were traced and classified for groups by gender, age, and dentofacial skeletal patterns. Size, shape, and bridging of ST were assessed. Multivariate ANOVA (MANOVA) analysis was used to detect the interaction between gender, age, and skeletal patterns on ST dimensions.
Results
The mean values for length, anteroposterior diameter, and depth of ST were 8.02 ± 1.67, 11.37 ± 1.60, and 8.56 ± 1.26 mm, respectively. A significant difference in length of ST between gender and age stages (p < 0.05) was detected while older subjects revealed a greater anteroposterior diameter than younger subjects (p < 0.05). The morphological variations of ST were observed in 55.6% of samples. No significant association between the shape of ST and skeletal patterns (p > 0.05) was found.
Conclusions
ST bridging was highly prevalent in Yemeni subjects (35.9%). Samples showed a higher rate of complete ST bridging in the three skeletal patterns, Class I (17.1%), Class II (18.9%), and Class III (20%). ST dimensions and shape findings in this study can be used as reference standards for further investigation, including the ST area in the Yemeni population.
Similar content being viewed by others

Introduction
‘‘Turkish saddle’’ which is commonly known as “Sella Turcica” (ST), is a superior depression of the sphenoid bone that hosts and protects the pituitary gland. The ST is composed of the anterior wall (tuberculum sellae), the posterior wall (dorsum sellae), and the pituitary fossa in between. The pituitary fossa is ringed with two anterior and two posterior clinoid processes, which may differ in shape and size [1].
The ST is considered as one of the critical anatomical references in orthodontics because the S-point, located in the center part of sella, is a fixed landmark in cephalometric analysis. Furthermore, the anterior wall of ST is utilized to assess craniofacial growth and interrelationship between jaws [2]. Such assessments are beneficial to predict orthodontic treatment outcomes, prescribe convenient orthodontic plans, and describe craniofacial patterns. On the other hand, any pathological or anatomical abnormalities in the pituitary gland could well reveal changes in the shape of ST.
Quite a several studies have been provided that certain pathological conditions, such as William syndrome [3], primary hypopituitarism [4], growth hormone deficiency [5], congenital lumbosacral abnormality, and seckel pear syndrome [6], could alter the shape and size of ST. One of the most popular forms of ST alteration is the fusion of the anterior and posterior clinoid processes, that known as ST bridging [1]. This form can also be highly related to severe craniofacial deviation, tooth agenesis [7], canine impaction [8], and individuals with cleft palate [9].
To detect anatomical disorder of the sella area, the normal morphology of the ST has to be demonstrated. However, the normal pattern varies from individuals to individuals. Hence, the evaluation must be conducted in races individually. That has been embodied in the published literature [10,11,12,13]. To date, average measurements and morphology of ST in Yemeni subjects remain unclear.
Accordingly, the current study aimed to assess and compare the shape, size, and bridging of ST in Yemeni subjects with different skeletal classifications, genders, and age stages. The null hypothesis was that no association between the linear dimension of ST and gender, age, or skeletal patterns.
Materials and methods
This was a cross-sectional study. The subjects were collected from “3D radiology center” in IBB city, Yemen. Digital cephalogram, and orthopantomogram, with a full record of the dental and medical history of 272 patients, were obtained via email. Radiographs are currently used, and referrals are being conveyed electronically in conjunction with photographs [12, 14]. Vatech, Pax-i3D Smart™ machine was used for all lateral cephalometric radiographs with 50–90 KVp and 4–16 mA for 12.9 sec. The individuals with distinct craniofacial syndromes, cleft lip, cleft palate, dental anomalies, severe skeletal deflections, and systemic conditions that have been proven to cause a transformation in form and size of ST were excluded. Only radiographs with high quality and clearance in ST area were involved. Therefore, the number of samples used in our study was 234 subjects (167 females and 67 males). Radiographs were distributed according to age into pre and post-pubertal stages, 8–14 years and 15–28 years, respectively, and according to skeletal patterns into three groups depending on the ANB angle; Class I: ANB angle 0–4 degree, Class II: ANB angle > 4, and Class III: ANB angle < 0 [10, 13, 15, 16]. The distribution is summarized in detail in Table 1.
Cephalometric analysis and the size of ST
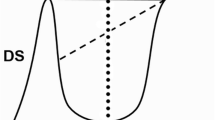
Each cephalometric radiograph was traced with Steiner analysis by using digital software (Uceph version 4.2.1, Chengdu ya xun Technology Co., Ltd). The ST dimensions were measured with the same software by (R.A) author, consistent with the approach defined by Silverman [17] as cited by Axelsson et al. [18] as shown in (Fig. 1). The length of ST was evaluated by drawing a line between the tips of tuberculum sellae and dorsum sellae. The depth of ST was detected as a constructed, perpendicular line from the former line to the deepest point on the floor surface. The anteroposterior diameter (A.P diameter) of ST was calculated as a distance between the tuberculum sellae and the farthest point on the fossa's posterior internal wall.

Normal ST morphology and reference lines used for measuring sellae size: TS, tuberculum sellae; DS, dorsum sellae; BPF, base of the pituitary fossa; black line, length of sellae; dashed line, Antero-posterior diameter of sellae; dotted line, depth of sellae
The shape of ST
ST morphology was classified according to the definitions of Axelsson et al. [18], as normal shape, irregular notching in the posterior wall of dorsum sellae, ST bridging, oblique anterior wall, pyramidal shape of dorsum sellae, and the double contour of the floor.
ST bridging
ST bridging was evaluated depending on the relationship between the length and A.P diameter of ST in line with Leonardi standard [19]:
-
Type 1 (no calcification): length of ST > 75% of A.P diameter of ST.
-
Type 2 (partial calcification): length of ST ≤ 75% of A.P diameter of ST, in the radiograph, was observed as an extension without fusion of the anterior and posterior clinoid process.
-
Type 3 (complete calcification): fusing between the anterior and posterior processes, radiographically detectable diaphragma sellae.
Reliability of measurements
Three months later, 30 lateral cephalometric images were chosen randomly and distributed equally between genders, age groups, and skeletal classifications. The images were re-evaluated by (X.L) author. The intraclass correlation coefficient (ICC) was conducted to estimate the ST dimension readings’ reproducibility and Kappa value was used to test reliability for the skeletal pattern, bridging, and shape of ST [20, 21].
Statistical analysis
Measurement data were inserted into the statistical package of social sciences version 26.0 (SPSS, IBM, New York, US) for statistical analysis. After proving the normality and homogeneity distribution of data. Multivariate ANOVA analysis (MANOVA) employed to examine the interaction of genders, two age stages and skeletal types on the linear measurements of ST, pairwise comparison and post hoc tests were performed when the differences statistically significant. Chi-square test was used to evaluate the association of ST morphology between genders, skeletal patterns, and age stages. The same test was also carried out to investigate the relation between ST calcification and skeletal patterns. Significance was set at p > 0.05. Statistically, the probability of rejecting the null hypothesis was 32% regarding gender and age interaction on ST length, 40% between skeletal patterns and ST depth, and 6% between age stages and ST A.P diameter, otherwise, the null hypothesis was accepted.
Results
The reliability measurements were 97, 95, and 94% for A.P diameter, depth, and length of the ST, respectively; and 100% for ST morphology and skeletal pattern, 91% for ST bridging.
The size of ST
The linear dimensions of ST were 8.02 ± 1.67, 11.37 ± 1.60, and 8.56 ± 1.26 mm for length, A.P diameter, and depth (Table 2). Summarizes the means and standard deviations of ST measurements according to age, gender and skeletal patterns. MANOVA interactions were showed that there was a significant difference between age and gender related to ST length (Table 3), pairwise comparison clarified that length of ST was greater in pre-pubertal male than in pre-pubertal female individuals. A significant association was observed between skeletal classes and the depth of ST (Table 3) whereas class II cases were with larger ST depth than class III as was explained by Scheffe’s multiple comparison. The A.P diameter was significantly correlated with age stages, the older group revealed greater diameter than the younger group (Table 3). The interaction among age, gender, and skeletal patterns all together on length, depth, and A.P diameter of ST was not statistically significant (Table 3).
The shape of ST
All six patterns of the ST inclusive of the normal pattern as summed up by Axelsson et al.[18] were found in the current study (Fig. 2). The normal morphology existed in 44.4% of subjects, followed by ST bridging (35.9%), pyramidal shape (6%), and double contour of the floor (5.1%). The oblique anterior wall (4.7%) and the irregular dorsum sellae (3.8%) were the least seen shapes. No significant association in the shape of ST between genders, age groups, or skeletal patterns was detected. Figure 3 typifies rates of ST morphology among the three skeletal classifications. The association between the shape of ST and the linear dimension of ST was determined (Table 4) and the result was not statistically significant.

a Normal morphology, b ST bridging, c double contour of the floor, d irregularity (notching) in the posterior wall of dorsum sellae, e pyramidal shape of dorsum sellae, f oblique anterior wall

Shape of ST in different skeletal patterns
ST bridging
Type 1 of ST bridging was noticed in 62.8% (n = 147), type 2 was found in 18.8% (n = 44), and type 3 was observed in 18.4% (n = 43) of samples in this study (Fig. 4). No significant association between ST calcification and skeletal patterns was detected (Table 5).

a Type 1 (no calcification), b Type 2 (partial calcification), c Type 3 (complete calcification)
Discussion
This retrospective study detected and compared the size, shape, and bridging of ST in Yemeni samples with different skeletal patterns, genders, and age stages.
Size of ST
The mean size of ST obtained from this study was larger than that in studies done by Magat et al. [22] among Turkish samples, Shrestha et al. and Muhammed et al. [13, 14] among Nepalese patients, Ghaida et al. [23] among Jordanian et al. [24] among Iraqi. In contrast, it was smaller by 0.5–2.83 mm than those reported by Alkofide [10] in Saudi samples. These discrepancies result from ethnic, genetic, and environmental differences between populations and the approaches of measurements, which may affect by the magnification degree in cephalogram and the location of measuring landmarks.
When determining if gender played differences in the size of ST, the previous literature [10, 13, 25,26,27,28] provided no significant difference in terms of all three ST dimensions. In contrast to those studies, Axelsson et al. [18] and Sathyanarayana et al. [11] observed that a significant difference in length of ST between females and males existed, Ghaida et al. [23] conducted a study on 509 samples, found that only height of ST showed a significant difference between females and males while Magat et al. [22] found that the A.P diameter was different between genders. While the current study result revealed that the significant difference was in the interaction between age and gender related to the length of ST, pre-pubertal female subjects were with shorter ST length than pre-pubertal males. May we need future studies to enhance and justify this result especially since this study is the first investigation conducted on Yemeni individuals.
Increasing the size of ST with age was associated with increasing the pituitary gland’s size [29, 30]. In the current study, significant differences in A.P diameter of ST among age groups were noticed. Post-pubertal patients had greater A.P diameter than pre-pubertal patients. This result is consistent with a study by Valizadeh et al. [31]. Muhammed et al. [12] carried a study on 360 samples from three races. Found that older patients presented higher length and diameter of ST than younger patients. Alkofide [10], and Yasa et al. [25] recorded that all three dimensions of ST increased with age. Hence, ST is growing with age, this growth happened at an early age in females, as stated by Preston [32]. Choi et al. [33] registered that growth is continuing up to 25 years of age. Therefore, no significant rise was recorded after 26 years of age.
In all related literature, whether or not the skeletal pattern correlates with the size of ST is still unclear. Alkofide [10] stated that the individuals with skeletal Class III patterns revealed a larger ST diameter compared to the individuals with Class II patterns. Shrestha et al. [13] found that length and A.P diameter was larger in Class III patients than those with Class II. In this study, individuals with skeletal Class III revealed a smaller depth of ST compared to individuals with skeletal class II pattern. Contrarily, Magat et al. [22], Meyer-Marcotty et al. [34] and Shah et al. [28] stated that there was no significant difference between the linear dimension of ST and skeletal patterns. These discrepancies among the results might be due to the difference in the degree of magnification or sample compositions (ethnicity, gender, age, etc.).
The shape of ST
Fifty-six percent of the patients indicated different variations in the shape of ST, and only 44% revealed normal sellae morphology in the present study. Shrestha et al. [13], Alkofide [10], and Sathyanarayana et al. [11] found the opposite result to the current research that patients with normal morphology of ST more than those with other variations in Nepalese, Saudi, and South Indian. However, Magat et al. [22] stated that only 39% of Turkish patients indicated normal ST morphology and 61% with other variations. The irregular shape of dorsum sellae was the least seen in this study (3.8%). In contrast, it was the most common finding in the population of Nepalese 15% [13], Saudi 11.1% [10], and South Indian 15% [11].
No significant differences in morphology of ST between genders, age groups, or skeletal patterns were detected.
Bridging of ST
ST bridging morphology was the most common variation of ST in this study, 35.9%. This result was higher than all the previous literature. Type 1 bridging was noticed in 62.8%, type 2 was seen in 18.8%, and type 3 was observed in 18.4% of the patients. According to the study conducted by Shrestha et al. [13], 65% of the patients indicated type 1 bridging, 23.33% type 2, and 11.67% type 3. Leonardi et al. [19], who used the length of ST rather than the interclinoid distance to detect the bridging type reported that 56.4, 33.7, and 9.9% of the patients revealed type 1, 2, and 3 of ST bridging, respectively, in the control group. In this study, the percentage of type 3 ST bridging was higher than all previous studies. Kogali S et al. [35] executed a cadaveric study of 112 adult skull bones to appraise the existence of type 3 ST bridging, which was 8.04%. Relatively higher percentage (18.4%) may have been detected in the present study as this was a radiographic study. The discrepancies between the radiographic studies and direct anatomical studies may be caused by overlapping’s superimposition of the clinoid processes in the cephalograms [36].
This study showed that 17.1% of Class I, 18.9% of Class II, and 20% of Class III were with type 3 ST bridging. Whereas Shrestha et al. [13] found that 5% of Class I and 17.5% of Class III indicated type 3 ST bridging. Meyer-Marcotty et al. [34] reported that 9.4% of Class I and 16.8% of Class III with type 3 ST bridging. An increase in the percentage of type 3 ST bridging in this study could be racial or maybe because of radiological reasons.
In the current study, there was no significant association between bridging types and skeletal patterns, while research has been done by Dasgupta et al. [37] who considered ST bridging as a predictor of Class II malocclusion. On the other hand, Meyer-Marcotty et al. [34] and Shrestha et al. [13] have found that the frequency of type 3 ST bridging in Class III is more than that in Class II. Abdel-Kader [38] registered that 6.9% of ST bridge was noticed in the orthognathic group, and 4.83 percent of ST bridging noticed in the orthodontic group in Saudi samples. Pattern of malocclusion affects the prevalence of ST bridging [1, 38]. A recent study has been performed on 156 Japanese patients with tooth agenesis, cited that ST bridging increased in patients with tooth agenesis. Another study was published by Sinha et al. [9] on 300 patients and reported that ST bridging resembled 38% in the cleft individuals group but only 10% in the non-cleft group. In our investigation, patients with tooth agenesis or cleft palate both were excluded. Calcification of diaphragma sellae, or ‘bridging’ of the ST, with no symptoms or clinical abnormalities, is regarded as one of ST normal variants [39]. However, some pathological conditions may relate to this calcification [7, 19, 40]. The study has been conducted on lateral cephalogram radiographs, which are two-dimensional images. Thus the obtained values were not as accurate as those obtained from the studies that use three-dimensional images (CBCT) or from cadaveric studies. Another drawback is the data was collected via email. Therefore, there were no model casts, and some tooth anomalies could not be detected.
Conclusion
ST bridging rates were obviously higher in Yemeni individuals (35.9%) in comparison with other populations. Length of ST was affected by the gender and age of subjects; however, A.P diameter of ST was influenced by only the age. No striking effects of skeletal patterns on calcification types or shape, length, and A.P diameter of ST were found. No association between the shape of ST and gender, age, and skeletal patterns of samples or between shape and size of ST were noticed. The findings of the current study can be utilized as reference standards for Yemeni subjects when studying ST by orthodontists, radiologists, or maxillofacial surgeons.
References
Jones R, Faqir A, Millett D, Moos K, McHugh S. Bridging and dimensions of sella turcica in subjects treated by surgical-orthodontic means or orthodontics only. Angle Orthod. 2005;75(5):714–8.
Kjær I. Sella turcica morphology and the pituitary gland—a new contribution to craniofacial diagnostics based on histology and neuroradiology. Eur J Orthod. 2015;37(1):28–36.
Axelsson S, Storhaug K, Kjær I. Post-natal size and morphology of the sella turcica in Williams syndrome. Eur J Orthod. 2004;26(6):613–21.
Ammar A, Al-Sultan A, Al Mulhim F, Al Hassan AY. Empty sella syndrome: does it exist in children? J Neurosurg. 1999;91(6):960–3.
Dostálová S, Šonka K, Šmahel Z, Weiss V, Marek J. Cephalometric assessment of cranial abnormalities in patients with acromegaly. J Craniomaxillofac Surg. 2003;31(2):80–7.
Venieratos D, Anagnostopoulou S, Garidou A. A new morphometric method for the sella turcica and the hypophyseal fossa and its clinical relevance. Folia Morphol. 2005;64(4):240–7.
Sato D, Endo T. Size and bridging of the sella turcica in Japanese orthodontic patients with tooth agenesis. Odontology. 2020;108(4):730–7.
Baidas LF, Al-Kawari HM, Al-Obaidan Z, Al-Marhoon A, Al-Shahrani S. Association of sella turcica bridging with palatal canine impaction in skeletal class I and class II. Clin Cosmet Investig Dent. 2018;10:179.
Sinha SP, Shetty A, Nayak UK. The morphology of sella turcica in cleft and non-cleft individuals. Saudi Dent J. 2020;32(2):86–92.
Alkofide EA. The shape and size of the sella turcica in skeletal class I, class II, and class III Saudi subjects. Eur J Orthod. 2007;29(5):457–63.
Sathyanarayana HP, Kailasam V, Chitharanjan AB. The size and morphology of sella turcica in different skeletal patterns among South Indian population: a lateral cephalometric study. J Indian Orthod Society. 2013. https://doi.org/10.1177/0974909820130507S.
Muhammed FK, Abdullah AO, Liu Y. Morphology, incidence of bridging, dimensions of sella turcica, and cephalometric standards in three different racial groups. J Craniofac Surg. 2019;30(7):2076–81.
Shrestha GK, Pokharel PR, Gyawali R, Bhattarai B, Giri J. The morphology and bridging of the sella turcica in adult orthodontic patients. BMC Oral Health. 2018;18(1):1–8.
Muhammed FK, Abdullah A, Liu Y. A morphometric study of the sella turcica: race, age, and gender effect. Folia Morphol. 2020;79(2):318–26.
Lauc T, Nakaš E, Latić-Dautović M, Džemidžić V, Tiro A, Rupić I, Kostić M, Galić I. Dental age in orthodontic patients with different skeletal patterns. Biomed Res Int. 2017. https://doi.org/10.1155/2017/8976284.
Daer AA, Abuaffan AH. Cephalometric norms among a sample of Yamani adults. Orthod Waves. 2016;75(2):35–40.
Silverman FN. Roentgen standards fo-size of the pituitary fossa from infancy through adolescence. Am J Roentgenol Radium Ther Nucl Med. 1957;78(3):451.
Axelsson S, Storhaug K, Kjær I. Post-natal size and morphology of the sella turcica. Longitudinal cephalometric standards for Norwegians between 6 and 21 years of age. Eur J Orthod. 2004;26(6):597–604.
Leonardi R, Barbato E, Vichi M, Caltabiano M. A sella turcica bridge in subjects with dental anomalies. Eur J Orthod. 2006;28(6):580–5.
Damstra J, Slater JJH, Fourie Z, Ren Y. Reliability and the smallest detectable differences of lateral cephalometric measurements. Am J Orthod Dentofacial Orthop. 2010. https://doi.org/10.1016/j.ajodo.2010.05.013.
Koo TK, Li MY. A guideline of selecting and reporting intraclass correlation coefficients for reliability research. J Chiropr Med. 2016;15(2):155–63.
Magat G, Sener SO. Morphometric analysis of the sella turcica in Turkish individuals with different dentofacial skeletal patterns. Folia Morphol. 2018;77(3):543–50.
Ghaida JA, Mistareehi AJ, Mustafa AG, Mistarihi S, Ghozlan HH. The normal dimensions of the sella turcica in Jordanians: a study on lateral cephalograms. Folia Morphol. 2017;76(1):1–9.
Yousif HA, Nahidh M, Yassir YA. Size and morphology of sella turcica in Iraqi adults. MDJ. 2010;7(1):23–30.
Yasa Y, Ocak A, Bayrakdar IS, Duman SB, Gumussoy I. Morphometric analysis of sella turcica using cone beam computed tomography. J Craniofac Surg. 2017;28(1):e70–4.
Konwar SK, Singhla A, Bayan R. Morphological (length, depth, and diameter) study of sella turcica in different mandibular growth patterns in Indians. IJDMS. 2016;3(3):4–9.
Otuyemi O, Fadeju A, Adesina B, Otuyemi D. A Cephalometric analysis of the morphology and size of sella turcica in Nigerians with normal and bimaxillary incisor protrusion. J West Afr Coll Surg. 2017;7(2):93.
Shah A, Bashir U, Ilyas T. The shape and size of the sella turcica in skeletal class I, II and III in patients presenting at Islamic International Dental Hospital, Islamabad. Pak Oral Dent J. 2011;31(1):102–8.
Sari S, Sari E, Akgun V, Ozcan E, Ince S, Saldir M, Babacan O, Acikel C, Basbozkurt G, Ozenc S. Measures of pituitary gland and stalk: from neonate to adolescence. J Pediatr Endocrinol Metab. 2014;27(11–12):1071–6.
Chauhan P, Kalra S, Mongia SM, Ali S, Anurag A. Morphometric analysis of sella turcica in North Indian population: a radiological study. Int J Res Med Sci. 2014;2(2):521–6.
Valizadeh S, Shahbeig S, Mohseni S, Azimi F, Bakhshandeh H. Correlation of shape and size of sella turcica with the type of facial skeletal class in an Iranian group. Iran J Radiol. 2015. https://doi.org/10.5812/iranjradiol.12(2)2015.16059.
Preston CB. Pituitary fossa size and facial type. Am J Orthod. 1979;75(3):259–63.
Choi W-J, Hwang E-H, Lee S-R. The study of shape and size of normal sella turcica in cephalometric radiographs. Imag Sci Dent. 2001;31(1):43–9.
Meyer-Marcotty P, Reuther T, Stellzig-Eisenhauer A. Bridging of the sella turcica in skeletal class III subjects. Eur J Orthod. 2010;32(2):148–53.
Kolagi S, Herur A, Patil G, Rairam G. Complete sella turcica bridges prevalence and dimensions. J Anat Soc India. 2011;60(1):22–5.
Becktor JP, Einersen S, Kjær I. A sella turcica bridge in subjects with severe craniofacial deviations. Eur J Orthod. 2000;22(1):69–74.
Dasgupta P, Sen S, Srikanth H, Kamath G. Sella turcica bridging as a predictor of class II malocclusion—an investigative study. J Stomatol Oral Maxillofac Surg. 2018;119(6):482–5.
Abdel-Kader HM. Sella turcica bridges in orthodontic and orthognathic surgery patients. A retrospective cephalometric study. Aust Orthod J. 2007;23(1):30–5.
Tetradis S, Kantor ML. Prevalence of skeletal and dental anomalies and normal variants seen in cephalometric and other radiographs of orthodontic patients. Am J Orthod Dentofacial Orthop. 1999;116(5):572–7.
Leonardi R, Farella M, Cobourne MT. An association between sella turcica bridging and dental transposition. Eur J Orthod. 2011;33(4):461–5.
Acknowledgements
The authors wish to acknowledge the contribution made by the 3D Scan center for providing the entire data in this study. This work was supported by the Chinese Scholarship Council (CSC) under Grant number CSC 2017BSZ011024. The authors also dedicate this work to the spirit of Dr. Fenik, the second corresponding author of this article, who left this life after being infected with COVID-19.
Funding
No funding was received to conduct this research.
Author information
Authors and Affiliations
Corresponding authors
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
AL-Mohana, R.A.A.M., Muhammed, F.K., Li, X. et al. The bridging and normal dimensions of sella turcica in Yemeni individuals. Oral Radiol 38, 162–170 (2022). https://doi.org/10.1007/s11282-021-00541-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11282-021-00541-7