
Abstract
Purpose
Postoperative pain is the commonest reason for delayed discharge and unanticipated hospital admission after ambulatory surgery. We investigated the severity of pain at 24 hr postoperatively and determined the most painful procedures. The need for further medical advice and clarity of postoperative analgesia instructions were also studied.
Methods
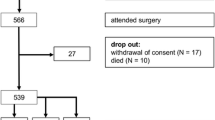
Five thousand seven hundred and three ambulatory surgical patients were telephoned 24 hr postoperatively. Patients graded their pain using the ten-point self-assessing verbal scale (0 = no pain, 10 = worst pain). Data were analyzed in two groups, those with moderate to severe pain (pain score 4–10) and those with no or mild pain (0–3).
Results
Thirty percent of patients (1,495/5,703) had moderate to severe pain. Microdiscectomy, laparoscopic cholecystectomy, shoulder surgery, elbow/hand surgery, ankle surgery, inguinal hernia repair, and knee surgery were identified as the procedures causing most pain at 24 hr. 13.2% of patients needed medical advice by telephone, 1.4% made an unplanned visit to a doctor while the rate of readmission to the hospital was 0.08%. Ninety-eight percent found postoperative instruction sheets and advice helpful. Eighty-eight percent of patients indicated that analgesic instructions were absolutely clear.
Conclusion
This study has identified the more painful common ambulatory surgical procedures which will allow take home analgesia to be tailored according to individual procedures. Further improvement in analgesic instructions may help in better pain management of ambulatory surgery patients.
Résumé
Objectif
La douleur postopératoire cause la plupart des départs retardés de l’hôpital ou des admissions non prévues après la chirurgie ambulatoire. Nous avons vérifié la sévérité de la douleur, 24 h après l’opération, et déterminé les interventions les plus douloureuses. La nécessité d’avis médical supplémentaire et la clarté des directives sur l’analgésie postopératoire ont aussi été notées.
Méthode
Nous avons téléphoné à 5 703 patients de chirurgie ambulatoire 24 h après l’opération. Les patients ont coté leur douleur selon une échelle verbale d’auto-évaluation en dix points (0 = aucune douleur, 10 = douleur très intense). Les données ont été classées en deux groupes : douleur modérée à sévère (score de 4–10) et douleur absente ou légère (0–3).
Résultats
Trente pour cent des patients (1 495/5 703) ont éprouvé des douleurs modérées à sévères. La microdiscectomie, la cholécystectomie laparoscopique, l’opération de l’épaule, du coude/de la main, de la cheville, la réparation d’une hernie inguinale et l’opération du genou causaient le plus de douleurs à 24 h. Nous avons noté que 13,2% des patients ont eu besoin d’avis médical au téléphone, 1,4% d’une visite médicale imprévue et 0,08 % d’une réadmission hospitalière. Les feuilles de directives postopératoires et les conseils ont été utiles pour 98 % des patients. Les directives sur l’analgésie ont été absolument claires pour 88 % des patients.
Conclusion
La présente étude a désigné les opérations chirurgicales ambulatoires courantes les plus douloureuses qui devront comporter une analgésie postopératoire à domicile adaptée aux besoins individuels. L’amélioration du traitement de la douleur postopératoire pourrait passer par des directives analgésiques plus claires.
Similar content being viewed by others


References
Twersky RS. Ambulatory surgery update. Can J Anaesth 1998; 45: R76–83.
Lakhani S, Leach Rd, Jarret PE. Effect of a surgical day unit on waiting lists. J R Soc Med 1987; 80: 628–9.
Meridy HW. Criteria for selection of ambulatory surgical patients and guidelines for anesthetic management: a retrospective study of 1553 cases. Anesth Analg 1982; 61: 921–6.
Chung F. Recovery pattern and home-readiness after ambulatory surgery. Anesth Analg 1995; 80: 896–902.
Ghosh S, Sallam S. Patient satisfaction and postoperative demands on hospital and community services after day surgery. Br J Surg 1994; 81: 1635–8.
Fortier J, Chung F, Su J. Unanticipated admission after ambulatory surgery—a prospective study. Can J Anaesth 1998; 45: 612–9.
Coley KC, Williams BA, DaPos SV, Chen C, Smith RB. Retrospective evaluation of unanticipated admissions and readmissions after same day surgery and associated costs. J Clin Anesth 2002; 14: 349–53.
Filos KS, Lehmann KA. Current concepts and practice in postoperative pain management: need for a change? Eur Surg Res 1999; 31: 91–107.
Rawal N. Postoperative pain management in day surgery. Anaesthesia 1998; 53(Suppl 2): 50–2.
Rosenberg J, Kehlet H. Does effective postoperative pain management influence surgical morbidity? Eur Surg Res 1999; 31: 133–7.
Chung F, Mezei G, Tong D. Adverse events in ambulatory surgery. A comparison between elderly and younger patients. Can J Anesth 1999; 46: 309–21.
Chung F, Ritchie E, Su J. Postoperative pain in ambulatory surgery. Anesth Analg 1997; 85: 808–16.
Callesen T, Bech K, Kehlet H. Prospective study of chronic pain after groin hernia repair. Br J Surg 1999; 86: 1528–31.
Rawal N, Hylander J, Nydahl PA, Olofsson I, Gupta A. Survey of postoperative analgesia following ambulatory surgery. Acta Anaesthesiol Scand 1997; 41: 1017–22.
Beauregard L, Pomp A, Choiniere M. Severity and impact of pain after day-surgery. Can J Anaesth 1998; 45: 304–11.
McHugh GA, Thoms GM. The management of pain following day-case surgery. Anaesthesia 2002; 57: 270–5.
Twersky R, Fishman D, Homel P. What happens after discharge? Return hospital visits after ambulatory surgery. Anesth Analg 1997; 84: 319–24.
Mezei G, Chung F. Return hospital visits and hospital readmissions after ambulatory surgery. Ann Surg 1999; 230: 721–7.
Hanchak NA, Patel MB, Berlin JA, Strom BL. Patient misunderstanding of dosing instructions. J Gen Intern Med 1996; 11: 325–8.
Hoddinott S. Report on a National Study of Access to Adult Basic Education Program and Services in Canada. Ottawa Board of Education, 1998; available from http://www.nald.ca/fulltext/stta/cover.htm.
Ad Hoc Committee on Health Literacy for the Council on Scientific Affairs. Health literacy: report of the Council on Scientific Affairs. JAMA 1999; 281: 552–7.
Le May S, Hardy JF, Taillefer MC, Dupuis G. Patient satisfaction with anesthesia services. Can J Anesth 2001; 48: 153–61.
Scott NB, Hodson M. Public perceptions of postoperative pain and its relief. Anaesthesia 1997; 52: 438–42.
Jenkins K, Grady D, Wong J, Correa S, Armanious S, Chung F. Post-operative recovery: day surgery patients’ preferences. Br J Anaesth 2001; 86: 272–4.
Macario A, Weinger M, Carney S, Kim A. Which clinical anesthesia outcomes are important to avoid? The perspective of patients. Anesth Analg 1999; 89: 652–8.
Martin Lopez MA, Fortuny GO, Riera FO, Grau LH, Maeso MP. Effectiveness of a clinical guide for the treatment of postoperative pain in a major ambulatory surgery unit. Ambul Surg 2001; 9: 33–5.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
McGrath, B., Elgendy, H., Chung, F. et al. Thirty percent of patients have moderate to severe pain 24 hr after ambulatory surgery: A survey of 5,703 patients. Can J Anesth 51, 886–891 (2004). https://doi.org/10.1007/BF03018885
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/BF03018885