

Abstract
Background/Aim: The relationship between renal function and severity of cardioembolic stroke (CES) stratified by sex remains poorly understood. Patients and Methods: A total of 640 consecutive CES patients within 48 h after stroke onset and with a modified Rankin Scale (mRS) score of 0 or 1 before onset were studied. The patients were divided into three groups based on their CCr values: low creatinine clearance (CCr) (L-CCr) (n=71, <30 ml/min), middle CCr (M-CCr) (n=227, 30 to <50 ml/min), and high CCr (H-CCr) (n=342, ≥50 ml/min). We compared the severity and functional outcomes of stroke among the three groups according to sex. Results: On admission, using the National Institutes of Health Stroke Scale, the L-CCr group had the most severe stroke, followed by the M-CCr and H-CCr groups (p<0.0001). Functional outcomes at discharge, assessed using the mRS, were the worst in the L-CCr group, followed by the M-CCr and H-CCr groups (p<0.0001). Multivariable analyses revealed that L-CCr was a significant determinant of severe stroke on admission and poor functional outcomes at discharge. According to sex, L-CCr was a significant determinant of severe stroke on admission and poor functional outcomes at discharge in female patients, but not in male patients. Conclusion: Low CCr is a risk factor for severe stroke on admission and unfavorable functional outcomes at discharge in Japanese CES patients, and particularly in female patients.
- Atrial fibrillation
- creatinine clearance
- cardioembolic stroke
- stroke severity
- functional outcome
The prevalence of both chronic kidney disease (CKD) and atrial fibrillation (AF) is increasing annually with the aging of the population (1). The Fushimi AF registry, which provides current clinical practice regarding real-world AF management in Japan, showed that 1.1% of the total population has AF and 26.4% of patients with AF have CKD (2). CKD is considered a risk factor for cardiovascular events; the presence of albuminuria and estimated glomerular filtration rate (eGFR) <60 ml/min/1.73 m2 increase the risk of cardiovascular events (3, 4). Creatinine clearance (CCr) and eGFR are calculated using an estimation formula based on serum creatinine levels (5, 6). As the value of creatinine differs based on sex and muscle mass, sex affects these formulas and some studies have investigated sex differences in CKD (7, 8).
Cardioembolic stroke (CES) associated with AF has been reported to be severe and has a poor functional prognosis; thus, anticoagulation is important for stroke prevention (9-11). Additionally, several studies investigating sex-related differences in the severity and functional outcomes of stroke in patients with ischemic stroke showed that the female sex is associated with severe stroke and unfavorable outcomes (12-15). However, few studies have reported the relationship between renal function and prognosis in patients with CES in relation to sex. In this study, we assessed the severity and functional outcomes of stroke in patients with CES with nonvalvular AF (NVAF) based on renal function in each sex.
Patients and Methods
Study patients. The Hirosaki Stroke and Rehabilitation Center (HSRC) provides an acute therapy in a stroke care unit and a rehabilitation therapy in a recovery rehabilitation ward. Over a 9-year period from April 2011 to March 2020, 1,659 consecutive patients with CES were admitted to the HSRC for acute therapy and chronic rehabilitation therapy within 60 days after the onset of CES. Of them, 640 patients with CES with NVAF within 48 h after the onset of the disease who had a modified Rankin Scale (mRS) score of 0 or 1 were studied (Figure 1).
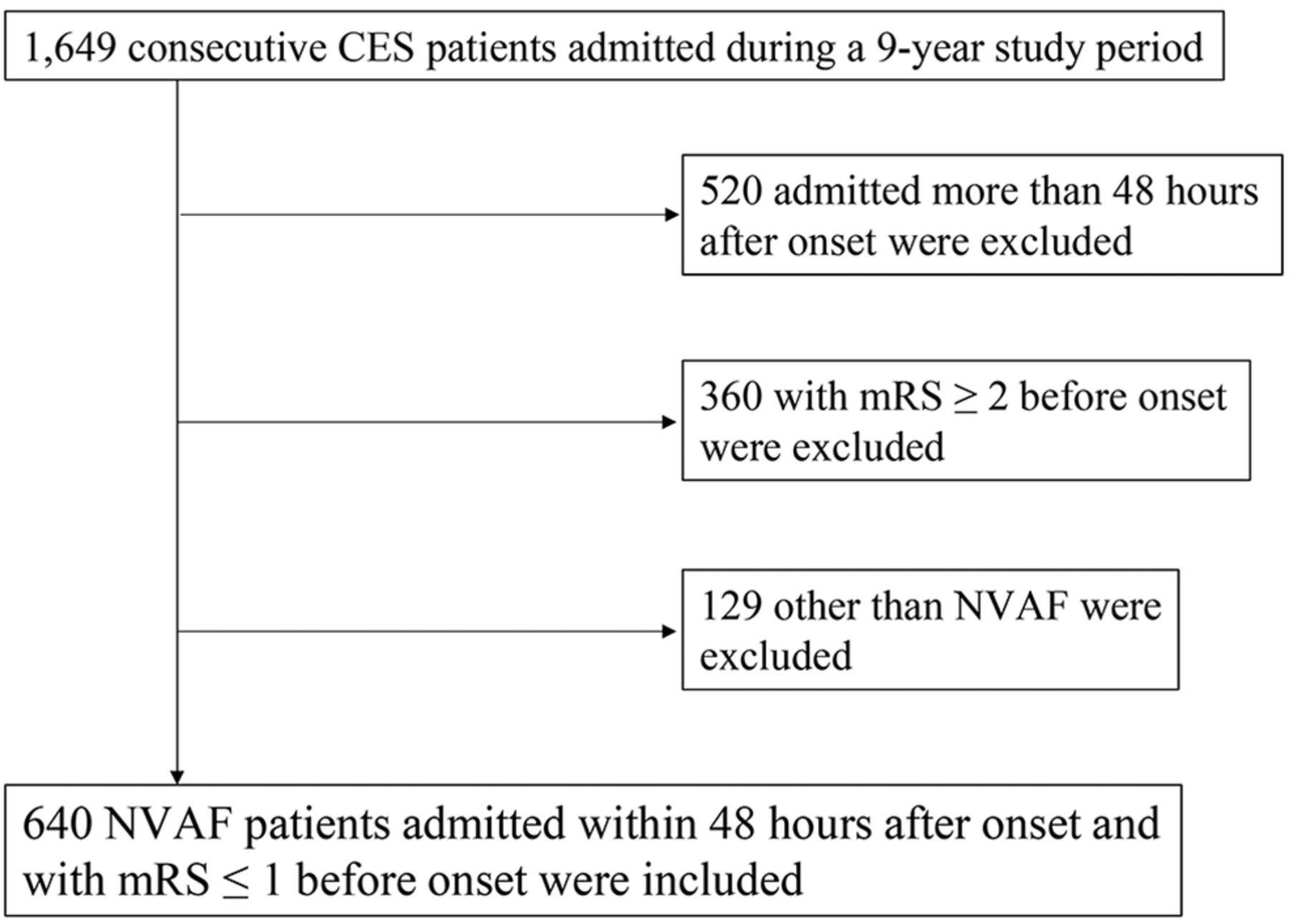
Flowchart of the study patients. CES: Cardioembolic stroke; mRS: modified Rankin Scale; NVAF: nonvalvular atrial fibrillation.
We used the Cockcroft–Gault equation to estimate the CCr (ml/min): [(140–age)×body weight/72×serum creatinine×(0.85 if sex=female)], which is an indicator of renal function required to administer direct oral anticoagulants (DOACs) in patients with NVAF. This equation is calculated by age, body weight, serum creatinine, and sex (5). The patients were divided into three groups based on their CCr values: the high CCr (H-CCr) group (≥50 ml/min; n=342; male/female=209/133), the middle CCr group (M-CCr) (30 to <50 ml/min; n=227; male/female=108/119), and low CCr (L-CCr) (<30 ml/min; n=71; male/female=23/48). Clinical characteristics, stroke severity on admission, and functional outcomes at discharge were analyzed and compared among these three groups and in each sex, separately. We further performed analyses using the eGFR (ml/min/1.73 m2), which is estimated based on the CKD-Epidemiology Collaboration Equation by Japanese formula [194×(serum creatinine)−1.094×(age)−0.287×(0.739 if sex=female)] (6).
This study was approved and an exemption of informed consent was granted by the ethics committee of the Hirosaki Stroke and Rehabilitation Center (Reference no.22B002) and the Hirosaki University Graduate School of Medicine (Reference no.2022-018). Subjects registered in the Hirosaki Stroke Registry (UMIN Clinical Trials Registry: UMIN000016880) were studied. All procedures were performed in accordance with the principles of the Declaration of Helsinki.
Diagnosis, stroke severity, and functional outcome. All patients underwent computed tomography of the brain on admission. Subsequently, magnetic resonance (MR) imaging including transversal diffusion-weighted imaging, T2-weighted imaging, fluid-attenuated inversion recovery, and MR angiography (Signa Excite HD 1.5T and Signa Explorer 1.5T; GE Medical System, Waukesha, WI, USA) were performed, when intracerebral hemorrhage was not detected. All patients underwent 12-lead electrocardiogram (ECG), chest X-ray, carotid ultrasonography, 24-h Holter ECG, and standard blood tests. CES was diagnosed based on the Trial of Org 10172 in Acute Stroke Treatment classification. Treatment with oral anticoagulants (OACs) before the onset of the disease was evaluated. Thrombolysis therapy with intravenous recombinant tissue plasminogen activator (rt-PA) was performed according to the Japanese guidelines. Stroke severity on admission was assessed using the National Institutes of Health Stroke Scale (NIHSS), and severe stroke was defined as an NIHSS score ≥8 (11, 15). Functional outcomes at discharge were assessed using the mRS. Thromboembolism risk before the onset of the disease was determined using the CHADS2 [congestive heart failure (CHF), hypertension, aged 75 years or older, diabetes, prior stroke or transient ischemic attack (TIA)] and CHA2DS2-VASc [CHF, hypertension, aged 75 years or older, diabetes, prior stroke or TIA, vascular disease, age 65-74 years, sex category (female)] scores in each patient.
Risk factors were as follows: CHF (New York Heart Association class II or higher, left ventricular ejection fraction <40%), hypertension (documented blood pressure ≥140/90 mmHg, antihypertensive treatment), diabetes (insulin or antidiabetic treatment or at least two determinations of diabetic type on separate days evaluated by fasting blood glucose ≥126 mg/dl, casual blood glucose ≥200 mg/dl, the oral glucose tolerance test, or HbA1c ≥6.5%), vascular disease (i.e., coronary artery disease, aortic plaque, or ankle brachial index ≤0.9), and dyslipidemia (lipid-lowering medications, triglyceride ≥150 mg/dl, low-density lipoprotein cholesterol ≥140 mg/dl, or high-density lipoprotein cholesterol <40 mg/dl).
Statistical analysis. Data were expressed as medians (25th-75th percentiles) or n (%). A statistical comparison of differences among the three groups was evaluated using the Kruskal-Wallis test or chi-square test. Multivariate logistic regression analyses for stroke severity on admission and functional outcomes at discharge were performed after adjusting for CHF, hypertension, diabetes, prior stroke or TIA, and OAC treatment. Statistical analyses were performed using JMP Pro 15 (SAS, Cary, NC, USA). p-Values of less than 0.05 indicated statistical significance.
Results
Patient profiles. The patient profiles in each group are summarized in Table I. The median age was 86 (82-89), 83 (79-87), and 76 (69-81) years in the L-CCr, M-CCr, and H-CCr groups, respectively (p<0.0001). The proportion of males and body weight were lower in the L-CCr group than those in the other groups (p<0.0001). The proportion of patients with CHF and vascular disease was higher in the L-CCr group than in the other groups. The proportions of patients with hypertension, diabetes mellitus, prior cerebral infarction or TIA, and dyslipidemia were not different among the three groups. The CHADS2 and CHA2DS2-VASc scores were higher in the L-CCr group than in the M-CCr and H-CCr groups (p<0.0001). The proportion of antiplatelet use was similar among the three groups. Moreover, no differences in OAC treatment before stroke onset and rt-PA thrombolysis were observed among the three groups.
Clinical characteristics of the study’s patients.
Comparisons of stroke severity on admission and functional outcomes at discharge. Stroke severity on admission was assessed using the NIHSS score. The patients in the L-CCr group had higher NIHSS scores than those in the M-CCr and H-CCr groups [14 (6-23) vs. 13 (5-20) and 8 (3-17), respectively; p<0.0001 by the Kruskal-Wallis test] (Table II). Multivariate logistic regression analysis of the NIHSS scores (≥8) on admission showed that the M-CCr and L-CCr groups differed significantly [odds ratio (OR)=1.68, 95% confidence interval (CI)=1.17-2.36; p=0.004, and OR=2.38; 95%CI=1.34-4.24; p=0.003, respectively], when the H-CCr group was used as a reference after adjusting for hypertension, diabetes mellitus, CHF, prior cerebral infarction or TIA, and OAC treatment before stroke onset (Table III). Regarding functional outcomes at discharge, assessed using the mRS, patients in the L-CCr group had the worst prognosis, followed by those in the M-CCr and H-CCr groups [4 (2-5), 4 (1-5), and 2 (1-4), respectively; p<0.0001] (Table II). Multivariate logistic regression analysis of the mRS scores (≥3) at discharge showed that the M-CCr and L-CCr groups differed significantly (OR=2.39; 95%CI=1.67-3.42; p<0.0001 and OR=3.27; 95%CI=1.84-5.79; p<0.0001, respectively), when the H-CCr group was used as a reference (Table III). Mortality was relatively higher in the L-CCr group than in the M-CCr and H-CCr groups, although there was no statistical significance (14%, 10%, and 7%, respectively; p=0.19) (Table II). The M-CCr group had the longest period of hospitalization, followed by the L-CCr and H-CCr groups [79 (20-121), 69 (24-114), and 53 (15-99), respectively; p=0.005] (Table II).
Comparisons of stroke severity on admission and outcomes at discharge among the three groups.
Multivariate logistic regression analysis for stroke severity on admission and outcomes at discharge.
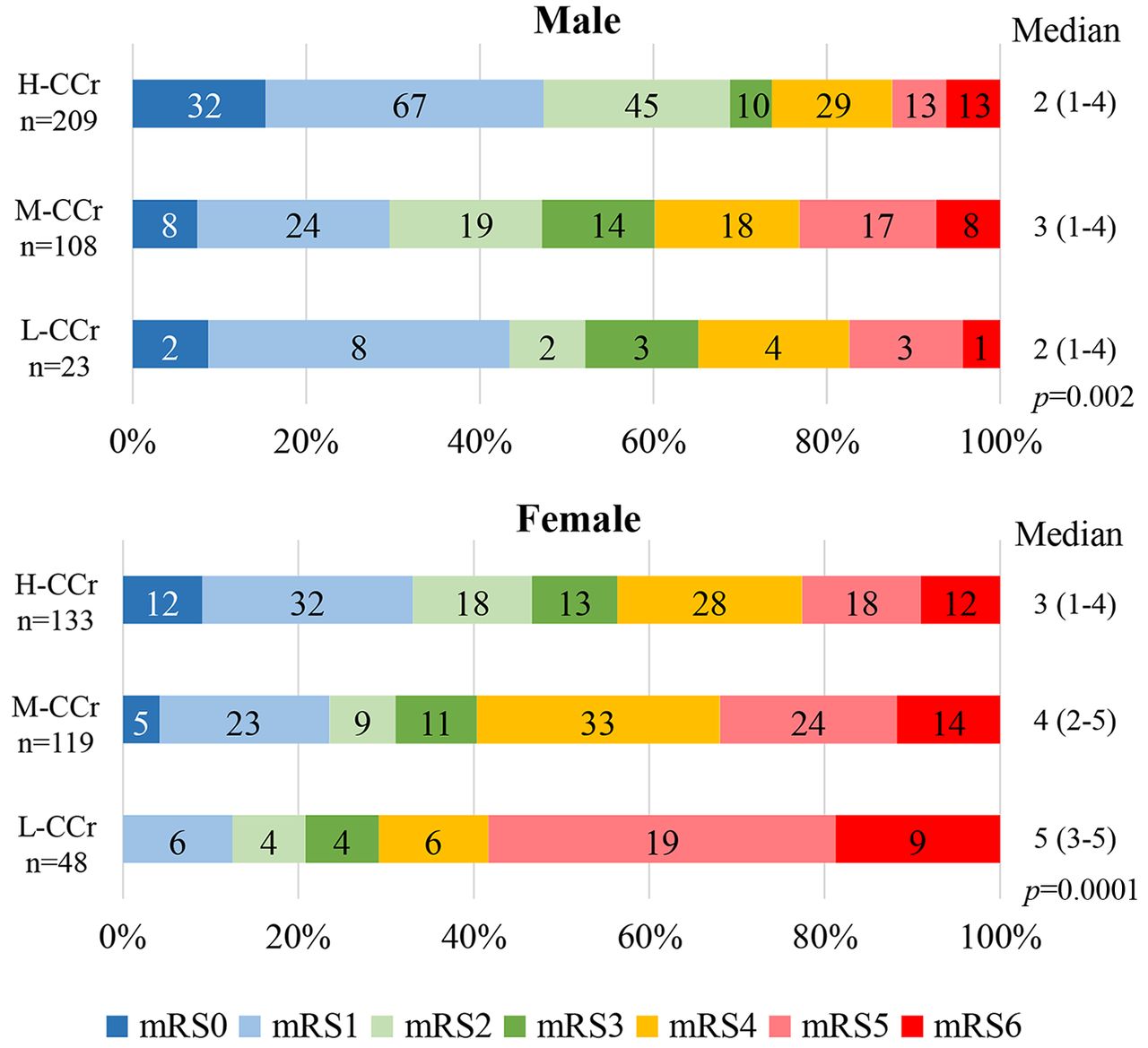
Analyses in each sex. We further analyzed stroke severity on admission and functional outcomes at discharge in each sex, separately. Multivariate logistic regression analysis of the NIHSS scores (≥8) on admission showed no difference among the three groups in male patients (Table IV). However, the M-CCr and L-CCr groups in female patients differed significantly (OR=1.93; 95%CI=1.11-3.37; p=0.02 and OR=3.33; 95%CI=1.41-7.89; p=0.006, respectively), when the H-CCr group was used as a reference (Table IV). The M-CCr group in male patients had the worst mRS score at discharge [3 (1-4)] compared with the L-CCr and H-CCr groups [2 (1-4) and 2 (1-4), respectively; p=0.002] (Figure 2). However, the L-CCr group in female patients had the worst mRS score [5 (3-5)], followed by the M-CCr and H-CCr groups [4 (2-5) and 3 (1-4), respectively; p=0.0001]. In the multivariate analysis of the mRS scores (≥3) at discharge, the M-CCr group in male patients differed significantly (OR=2.64; 95%CI=1.59-4.39; p=0.0002); however, the L-CCr did not differ (OR=1.95; 95%CI=0.79-4.83; p=0.15) (Table IV). In contrast, the M-CCr and L-CCr groups in female patients differed significantly (OR=1.84; 95%CI=1.06-3.17; p=0.03 and OR=3.04; 95%CI=1.34-6.86; p=0.008, respectively), when the H-CCr group was used as a reference.
Multivariate logistic regression analysis for stroke severity on admission and outcomes at discharge in each sex.

{kind=link}
{kind=link}
Comparison of the modified Rankin Scale (mRS) scores at discharge among the three groups in each sex. The median value and 25th-75th percentiles are shown in each group. The numbers in the graph indicate the number of patients. Creatinine clearance (CCr) was estimated using the Cockcroft–Gault equation. H-CCr ≥50 ml/min, 30≤M-CCr <50 ml/min, and L-CCr <30 ml/min.
Analyses using the eGFR. We performed analyses using the eGFR in the same way as CCr. The patients were divided into three groups based on the eGFR (ml/min/1.73 m2) values: eGFR <30 (L-eGFR) (n=32, male/female=8/24), eGFR 30 to <60 (M-eGFR) (n=291, male/female=151/140), and eGFR ≥60 (H-eGFR) (n=317, male/female=181/136). The patient characteristics in each group are summarized in Table V. The NIHSS scores on admission did not differ among the three groups (Table VI). Multivariate logistic regression analysis of the NIHSS scores (≥8) on admission also showed no significant difference among the three groups (Table VII). Regarding mRS scores at discharge, patients in the L-eGFR group had the worst prognosis, followed by those in the M-eGFR and H-eGFR groups [4 (2-5), 3 (1-5), and 2 (1-4), respectively; p=0.007] (Table VI). Multivariate logistic regression analysis of the mRS scores (≥3) at discharge showed that the L-eGFR group differed significantly (OR=2.96; 95%CI=1.29-6.81; p=0.01), when the H-eGFR group was used as a reference (Table VII). Mortality and period of hospitalization were not significantly different among the three groups (Table VI). According to sex, neither the NIHSS scores (≥8) on admission nor the mRS scores (≥3) at discharge differed significantly among the three groups in both sexes by multivariate analysis (Table VIII).
Clinical characteristics of the study’s patients.
Comparisons of stroke severity on admission and outcomes at discharge among the three groups.
Multivariate logistic regression analysis for stroke severity on admission and outcomes at discharge.
Multivariate logistic regression analysis for stroke severity on admission and outcomes at discharge in each sex.
Discussion
Major findings. In this study, we found that patients with CES with low CCr values, and particularly women, had higher NIHSS scores on admission and unfavorable functional outcomes at discharge. Furthermore, a sex difference was found in stratified analysis based on CCr, but not on eGFR. These findings indicate that low CCr in female patients with CES is a risk factor for severe stroke on admission and unfavorable functional outcomes at discharge.
Severe stroke and unfavorable functional outcomes in patients with CES with CKD. CKD is an independent risk factor for cardiovascular diseases and stroke. In a study of 1,120,295 adults who had not undergone dialysis or kidney transplantation, the adjusted hazard ratio (HR) for death, cardiovascular events, and hospitalization increased significantly with a reduced eGFR (16). A meta-analysis showed that eGFR <60 ml/min/1.73 m2 was independently associated with the incidence of stroke, particularly in Asian patients (3). A lower CCr is also reported to be an independent predictor of all-cause death and thromboembolism, including ischemic stroke, in 6,052 patients with NVAF registered in the J-RHYTHM Registry (17).
CKD is not only a risk factor for such events but also a predictor of poor prognosis in patients with stroke (18-20). Husseini et al. showed that decreased eGFR <60 ml/min/1.73 m2, particularly eGFR <15 without dialysis, is associated with in-hospital mortality or hospice in patients aged ≥65 years admitted with acute ischemic stroke (21). In analyses stratified by stroke subtypes, Yeh et al. showed that decreased eGFR, particularly eGFR <30 ml/min/1.73 m2, is associated with poor functional outcomes (mRS >3) and mortality 6 months after stroke onset in patients with large-artery atherosclerotic stroke using the data from the Taiwan Stroke Registry (22). Furthermore, a recent report from the Japan Stroke Data Bank showed that both eGFR <45 ml/min/1.73 m2 and proteinuria are associated with unfavorable functional outcomes (mRS scores of 3-6) at discharge in patients with CES or small vessel occlusion after adjusting for several factors, including sex (23). Consistent with this, this study also showed that decreased renal function in patients with CES is associated with unfavorable functional outcomes at discharge. Notably, we showed that decreased CCr values (M-CCr and L-CCr) are associated with both high NIHSS scores on admission and unfavorable functional outcomes at discharge, which is much clearer than decreased eGFR. By definition, the equation for calculating CCr includes sex, serum creatinine, and body weight, whereas that for calculating the eGFR includes sex and serum creatinine, but not body weight. We previously showed that low body mass index is a risk factor for severe stroke and unfavorable outcomes in patients with CES and NVAF (24). The inclusion of body weight in the equation for calculating CCr may have a significant impact on severe stroke and poor prognosis.
The kidney and brain have a similar vascular structure with small arterial vessels exposed to high-pressure fluctuations, resulting in microvascular damage. Traditional risk factors, such as diabetes and hypertension, further exacerbate these vascular damages. Consequently, these may lead to renal impairment and cerebral stroke or damage (25-27). Although the underlying mechanism remains to be determined, microvascular damage may be partly associated with severe stroke in patients with CKD. Further studies are clearly required.
Sex differences in stroke severity and functional outcomes in patients with CKD. Several studies investigating sex-related differences in stroke severity and functional outcomes in patients with ischemic stroke showed that the female sex is associated with severe stroke and unfavorable outcomes (12-14, 28). Additionally, we have previously shown that the female sex is an independent determinant of severe stroke and unfavorable functional outcomes, when only patients with CES were analyzed (15). Estrogen has a protective effect against ischemic stroke in middle-aged and autumnal women because it exerts anti-inflammatory effects, decreases cerebral vascular tone, and thereby increases cerebral blood flow (28, 29). Therefore, women after menopause may be exposed to an increasing risk of severe stroke compared with men (30, 31). Furthermore, microvascular damage due to renal impairment and the absence of the protective effect of estrogen after menopause may synergistically contribute to severe stroke and unfavorable outcomes in female patients with CKD. However, it cannot be completely excluded that stroke severity in male L-CCr patients is underestimated because only a few patients were included in this patient group (n=23).
Clinical implication. This study showed that patients with CES with low CCr values, particularly female ones, had a poor prognosis. Therefore, anticoagulation therapy should be ideally administered to L-CCr patients with NVAF to prevent the incidence of CES. However, as patients with CKD and NVAF are at a high risk of not only cerebral infarction but also cerebral hemorrhage, the use of OACs may often be hesitated in clinical settings. Four phase III randomized controlled trials comparing DOACs with warfarin in patients with NVAF excluded patients with severe renal insufficiency (CCr <30 or <25 ml/min) (32-35). Recently, the ELDERCARE-AF trial comparing edoxaban (15 mg) with placebo in Japanese patients with NVAF aged ≥80 years bridged this gap (36). A subgroup analysis stratified according to renal function showed that stroke/systemic embolism was significantly reduced in the edoxaban group compared with that in the placebo group in patients with CCr values of 15 to <30 ml/min (HR=0.33; 95%CI=0.16-0.71; p<0.01). However, major bleeding, mostly gastrointestinal bleeding, was relatively higher in the edoxaban group than that in the placebo group (HR=2.53; 95%CI=0.96-6.72; p=0.06) (37). The administration of edoxaban may be an alternative for patients with NVAF with low CCr values, although careful attention should be paid to gastrointestinal bleeding.
Study limitations. This study has several limitations. First, this was a single-center observational study, and therefore, the generalizability of our results may be limited. However, we studied consecutive patients during the study period and evaluated the severity and functional outcomes of these patients, thereby minimizing the biases caused by adopting an observational study design. Second, we used the Cockcroft–Gault equation to estimate the CCr as an indicator of renal function. As we mentioned earlier, CCr based on this equation is usually calculated to administer DOACs in patients with NVAF. We believe that the linkage of CCr based on this equation between stroke severity and DOAC administration provides some clinical implications. Third, the effect of rt-PA treatment on stroke severity and functional outcomes cannot be completely excluded, despite the not so many patients. Finally, the precise mechanisms by which female patients with CES, but not male ones, with low CCr values develop a poor prognosis, remain largely unknown. Further studies are clearly warranted.
Conclusion
Low CCr is a risk factor for severe stroke on admission and unfavorable functional outcomes at discharge in female Japanese patients with CES, but not in male patients.
Acknowledgements
The Authors are grateful to Mrs. Haruka Tonosaki for her excellent technical support.
Footnotes
Authors’ Contributions
Conception: Shuntaro Sakai, and Hirofumi Tomita. Study design: Shuntaro Sakai, Joji Hagii, and Hirofumi Tomita. Date collection and processing: Shuntaro Sakai, Joji Hagii, Shun Shikanai, Yuya Sorimachi, Shogo Hamaura, Ken Yamazaki, Natsumi Yamada, Hiroshi Shiroto, Shin Saito, Takaatsu Kamada, and Shingo Takanashi. Article writing: Shuntaro Sakai. Critical review: Joji Hagii, Ken Okumura, and Hirofumi Tomita.
Conflicts of Interest
Dr. Tomita received research funding from Boehringer Ingelheim, Bayer, Daiichi-Sankyo, and Speakers’ Bureau/Honorarium from Boehringer Ingelheim, Bayer, Daiichi-Sankyo, and Bristol-Myers Squibb. Dr. Okumura received Speakers’ Bureau/Honorarium from Boehringer Ingelheim, Bayer, Daiichi-Sankyo, Bristol-Myers Squibb, and Pfizer. The rest of the Authors have no relevant disclosures.
- Received October 18, 2022.
- Revision received October 30, 2022.
- Accepted November 1, 2022.
- Copyright © 2023, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).