

Abstract
Background/Aim: Sinonasal rhabdomyosarcoma (RMS) is a rare soft tissue malignancy. Due to the limited cases, the clinicopathological features and prognostic factors are still not well understood. Patients and Methods: This retrospective review included eight patients with sinonasal RMS at our institution between 2004 and 2020. Patient demographics, tumor features, Intergroup Rhabdomyosarcoma Study Group (IRSG) stage and clinical group, treatment strategy, and survival rates were evaluated. Kaplan-Meier analysis and log-rank tests were performed to analyze the possible prognostic factors. Results: We observed a predominance of male sex and alveolar-type tumor in sinonasal RMS. Nasal obstructions and neck masses were the most common symptoms. Patients with pretreatment lactate dehydrogenase (LDH) levels >400 U/l and negative immunohistochemical staining for desmin or MyoD1 had lower survival rates. Conclusion: In patients with sinonasal RMS, pretreatment LDH levels >400 U/l and negative immunohistochemical staining for desmin or MyoD1 may suggest a poor prognosis. These factors can not only contribute to the prediction of prognosis in patients with sinonasal RMS but also facilitate the design of more appropriate treatment strategies.
- Rhabdomyosarcoma
- sinonasal
- lactate dehydrogenase
- desmin
- MyoD1
Rhabdomyosarcoma (RMS) is a malignant tumor with a propensity for skeletal muscle differentiation. It is the most common soft tissue sarcoma in children, accounting for approximately 50% of all pediatric soft tissue sarcomas (1-3). However, it is rare in adults, accounting for <1% of all adult malignancies. RMS can be classified into four histological subtypes: embryonal (ERMS), alveolar (ARMS), pleomorphic (PRMS), and spindle cell/sclerotic. ERMS is the most common type, followed by ARMS (4, 5). ARMS is more aggressive than the other subtypes and is often associated with a worse prognosis. ARMS can be further classified according to the presence or absence of the paired box (Pax) proteins 3 and 7/forkhead box O1 (PAX3/7-FOXO1) fusion gene. The outcome in patients with fusion-negative ARMS is indistinguishable from that in ERMS and differs significantly from that in ARMS with fusion genes (6).
Approximately 35% of RMS cases arise in the head and neck region, including the orbital, parameningeal, and non-parameningeal areas (3). Tumors in the parameningeal areas have the worst outcome among those in the head and neck region, especially the paranasal sinuses, owing to the structural complexity and tendency for central nervous system (CNS) and skull base invasion (3, 7, 8). As the tumor location affects the disease prognosis, it appears alongside the usual TNM in the Intergroup Rhabdomyosarcoma Staging Group (IRSG) staging of RMS (9). In addition, the IRSG clinical group for RMS is based on the extent of residual disease after resection and evidence of regional lymph node (LN) or distal metastasis, which is one of the most important prognostic factors in RMS. The treatment strategy for RMS, which includes surgery, chemotherapy, and radiotherapy, is risk-based. The main treatment strategy for sinonasal RMS is a combination of chemotherapy and radiotherapy, with surgery applied to resectable tumors or as salvage therapy (10).
The current study retrospectively analyzed the clinicopathological features, outcomes, and prognostic factors of sinonasal RMS at the Taipei Veterans General Hospital over a 17-year period.
Patients and Methods
Patient population. This retrospective review included eight patients with sinonasal RMS who were treated at Taipei Veterans General Hospital, between 2004 and 2020. This study was approved by the hospital Institutional Review Board.
Sinonasal RMS was defined as RMS with lesions originating in the nasal cavity or paranasal sinus. Patient demographics (age and sex), presenting symptoms, tumor characteristics (location, histological type, regional lymph node status, distal metastasis status, skull base, orbit, and CNS invasion), treatment strategy, and overall survival were recorded. Histological confirmation was obtained for every case and all tumor characteristics were evaluated using computed tomography (CT) or magnetic resonance imaging (MRI). The IRSG-TNM staging system and IRSG clinical group classification were also applied for all patients.
Statistical analysis. The follow-up time was defined as the interval between the start date of treatment and events or the last follow-up date. The Kaplan-Meier method was used to establish survival curves, and log-rank tests were used to compare the overall survival of patients with different characteristics. Categorical data including tumor characteristics and patient demographics were compared using Fisher’s exact tests. All statistical analyses were carried out using SPSS version 24.0 (SPSS Inc., Chicago, IL, USA). The results were considered significant at p<0.05.
Results
Patient demographics. The demographic features of the eight patients (five men and three women) with sinonasal RMS included in this study are listed in Table I. The mean age at diagnosis was 30.25 years (range=7-57 years) and two patients were diagnosed at <18 years of age. The most common symptoms were nasal obstruction and painless neck mass, followed by epistaxis and rhinorrhea. None of the patients had a history of cancer or radiotherapy exposure; however, one patient had a family history of nasopharyngeal carcinoma.
Characteristics of sinonasal rhabdomyosarcoma in study’s patients (N=8).
Tumor characteristics. Most of the tumors were ARMS (n=6, 75%), with five tumors showing gene translocation. ERMS was identified in one patient. However, the tumor subtype in one patient could not be identified. The tumors were identified in the nasal cavity, maxillary sinuses, and ethmoid sinuses in all patients, followed by the frontal and sphenoid sinuses in 50.0% and 12.5% of patients, respectively. Five and three patients had tumors on the left and right sides, respectively. Skull base, orbit, and CNS invasions were discovered in three, four, and three patients, respectively. Most patients presented with regional disease (n=6, 75%). Distant metastasis and localized disease were observed in three (37.5%) and one cases (12.5%), respectively.
According to the IRSG-TNM staging system, stage III disease was the most common (n=5, 62.5%), followed by stage IV disease (n=3, 37.5%). One patient (12.5%) had IRSG clinical group II disease, whereas four (50%) and three (37.5%) patients had group III and group IV disease, respectively. Radiotherapy and chemotherapy using various regimens were administered to all patients (Table II). Four patients (50%) underwent surgery, with two patients undergoing surgery before and after chemotherapy. The mean follow-up time was 24.73 months. Most cases developed local recurrence (n=5, 62.5%). Regional recurrence and distal metastasis after treatment were observed in one and four cases, respectively.
Initial chemotherapy regimen of sinonasal rhabdomyosarcoma in study’s patients.
Immunohistochemical features. The immunohistochemical features are summarized in Table III. Six, five, and six cases were positive for desmin, MyoD1, and myogenin, respectively. Desmin, MyoD1, and myogenin positivity was observed in half of the cases (cases 1, 4, 5, 6). Case 1 was positive for CD99. Case 2 was positive for staining for desmin, MyoD1, vimentin, and HHF-35. Case 3 was positive for desmin and myogenin, and focally positive for synaptophysin. Case 7 was positive for myogenin and CD99.
The results of immunohistochemical staining in study’s patients.
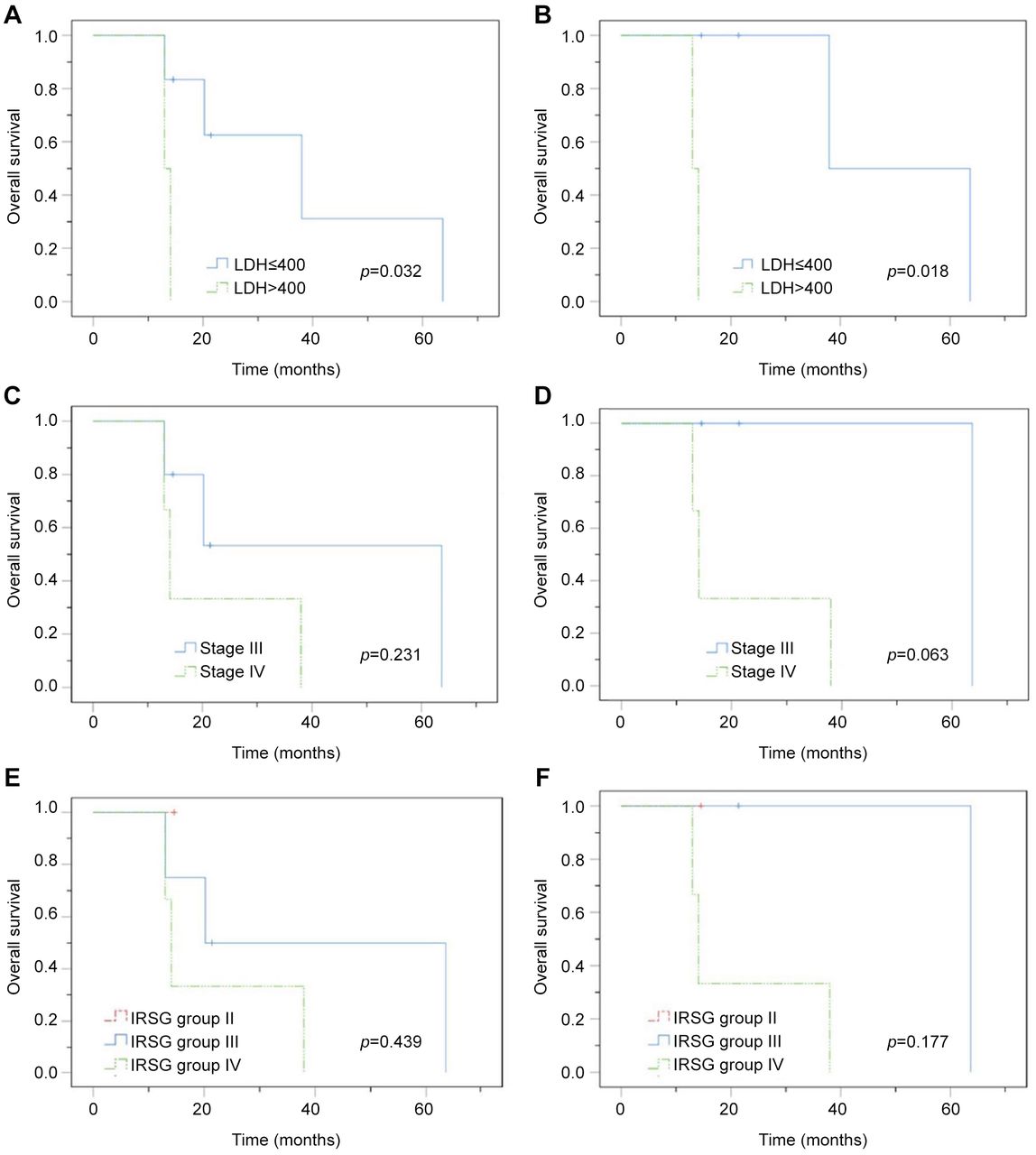
Prognosis analysis. Patients with pretreatment lactate dehydrogenase (LDH) levels >400 U/l had a significantly worse survival rate than those with LDH levels <400 U/l (p=0.032, Figure 1A). A similar result was observed after excluding patients <18 years of age (p=0.018, Figure 1B).

Kaplan-Meier survival curves according to pretreatment serum LDH levels in (A) all patients and (B) adult patients, stage in (C) all patients and (D) adult patients, IRSG clinical group in (E) all patients and (F) adult patients.
Patients with stage IV disease at the time of diagnosis had worse survival rates than those with stage III disease in both groups (including or excluding patients <18 years); however, these differences were not statistically significant (p=0.231, p=0.063, respectively; Figure 1C and D).
A survival analysis based on the IRSG clinical group was also performed. Group II included only one case, and the follow-up time was too short for analysis. In both groups, after including and excluding patients aged <18 years, those with IRSG clinical group IV disease had lower survival rates than those with clinical group III disease. However, these differences were not statistically significant (p=0.439, p=0.177, respectively; Figure 1E and F).
Immunohistochemical staining was analyzed in the survival analysis. Only seven cases were included in the analysis, owing to a missing immunohistochemistry staining report in one case. Patients who tested negative for desmin had significantly worse survival rates than those who tested positive (p=0.014, Figure 2A). Similar results were observed after excluding patients aged <18 years (p=0.025, Figure 2B).

{kind=link}
{kind=link}
Kaplan-Meier survival curves according to the results of desmin in immunohistochemical staining in (A) all patients and (B) adult patients, and the results of MyoD1 in (C) all patients and (D) adult patients.
In both groups, including and excluding patients <18 years, those negative for MyoD1 had significantly lower survival rates than those positive for MyoD1 (p=0.025, p=0.046, respectively; Figure 2C and D). In our study, there were no significant differences in overall survival based on age, sex, histological type, and the presence of gene translocation (all p>0.05) (Table IV).
Overall survival of sinonasal rhabdomyosarcoma patients with various characteristics.
Discussion
RMS is the most common soft-tissue sarcoma in children (11). However, some studies have reported that it is rare in the adult population, with a less favorable outcome (1, 12-14). One reason for this finding is that adult patients are more likely to have ARMS, which is more aggressive than ERMS (4). Another potential reason is that children with RMS have a better sensitivity to chemotherapy than adults with the disease (12). Some studies have shown a higher proportion of regional or distant metastases at the time of diagnosis in adults with RMS (1, 15). Although adult RMS is inherently different from pediatric RMS, Ferrari et al. suggested that both children and adults with RMS should receive similar treatment (1).
However, in the current study, pediatric patients did not have a significant superior survival rate than adults (Table IV). Only two cases were children (25%), with the histological type in one case being ARMS (50%). The disproportionate distributions of the histological subtypes among the children in our study compared to the usual distribution may have contributed to the statistical differences between our study and others.
For sinonasal RMS, Li et al. found an overall male predominance, with a male-to-female ratio of 1.7:1, which was consistent with the current study (16). In contrast, Sanghvi et al. reported a higher incidence in women than in men (11). However, some studies have reported equal distributions of men and women (7, 17). No significant differences in survival based on sex were noted in most studies, compatible with our current study (Table IV) (11, 16-19). However, Turner et al. reported a significantly longer survival in women compared to men (7). Variations in sex-specific hormones may play a role in improving the survival of women.
The prognosis of patients with sinonasal RMS is related to the tumor size and extension. Therefore, early diagnosis and treatment are critical. However, the initial symptoms of RMS are usually subtle and vary depending on the primary site. Nasal obstruction, rhinorrhea, and recurrent otitis media are the most common symptoms in patients with sinonasal RMS (12, 20). The present study demonstrated similar results. The most common symptoms at presentation were nasal obstruction (50%) and neck mass (50%), followed by rhinorrhea (37.5%) and epistaxis (37.5%). Thus, RMS should be included in the differential diagnosis of nasal obstruction, rhinorrhea, or other nonspecific symptoms in adults or children. Recently, Jaly et al. reported that head and neck sarcomas may present as large, solitary, superficial masses without lymph node enlargement, and the imaging feature may raise suspicion of the diagnosis of sarcoma (21).
ERMS type is the most common type in patients with RMS, followed by the ARMS and PRMS type (1, 4, 7, 15, 16). The ARMS form, which is more aggressive than the ERMS form, is more common in adult patients (4). Some studies reported an ERMS predominance and better prognosis in younger children, whereas adolescents were more likely to have ARMS and worse outcomes (12). Sanghvi et al. found that the survival rates in patients with embryonal sinonasal RMS were higher than those with alveolar sinonasal RMS (11) In contrast, Wurm et al. reported that there was no significant difference in survival between embryonal and alveolar sinonasal RMS, which is consistent with the findings in our current study (Table IV) (22).
According to gene status, ARMS can be further divided into fusion gene-positive and fusion gene-negative subtypes. The two translocations, t(2;13) (q35;q14) and t(1;13)(p36;q14), result in the expression of paired box (Pax) proteins 3 and 7/forkhead box O1 (PAX3/FOXO1) and PAX7/FOXO1, which are expressed in approximately 80% of patients with ARMS (23, 24). Fusion proteins influence proliferation, apoptosis, differentiation, and motility, all of which contribute to tumorigenesis. The PAX/FOXO1 fusion gene status influences the prognosis in patients with fusion-gene-negative ARMS, the prognosis of which is comparable to that of patients with ERMS. However, the genetic abnormalities of ERMS differ from those of ARMS. ERMS is caused by the loss of heterozygosity on the short arm of chromosome 11, which results in the inactivation of a tumor-suppressor gene and promotes tumor growth (25). Five cases (83.3%) in the present study had fusion-positive ARMS. In our study, there was no significant difference in overall survival between patients with fusion-negative ARMS and patients with fusion-positive ARMS (Table IV).
Pathologists can diagnose RMS based on tumor morphology with better differentiation, such as the presence of cross striations or rhabdomyoblasts. However, RMS displays a wide morphological spectrum and can be poorly differentiated, resembling other small blue round-cell tumors that require immunohistochemistry (IHC) for conclusive diagnosis (26). IHC staining of desmin, muscle-specific actin, myogenin, MyoD1, and myoglobin was used to diagnose RMS. Desmin is a frequently used marker with high sensitivity but low specificity for the diagnosis of RMS (27). Morotti et al. reported similarly high sensitivities and specificities for MyoD1 and myogenin, making them the most useful tools for confirming the diagnosis of RMS (27). In the present study, six, five, and six cases were positive for desmin, MyoD1, and myogenin, respectively. Surprisingly, patients who tested negative for desmin had a significantly worse survival rate than those who tested positive, contrary to the report by Dias et al., who hypothesized that desmin positivity was more commonly observed in well-differentiated RMS patients who did not respond well to chemotherapy (28). One explanation for our discordant finding may be the limited sample size, with only one desmin-negative case. Moreover, the patient was stage IV at the time of diagnosis, which could have affected the prognosis. In the present study, we found that patients with negative MyoD1 expression had a much worse survival rate than those with positive MyoD1 expression. The same was reported by Ahmed et al. (29). This may be because MyoD1 plays a role in cancer development, including regulation of proliferation and apoptosis (30).
Elevated LDH levels are a negative prognostic factor for lymphoma and several solid cancers, including renal cell carcinoma, nasopharyngeal carcinoma, sarcoma, and lung cancer (31). Glycolysis is the main energy source for malignant cells. The reversible conversion of pyruvate to lactate is catalyzed by LDH, and the LDHA isoenzyme, which is typically expressed by malignant cells, has a greater affinity for pyruvate and converts pyruvate to lactate. Lactate promotes tumorigenesis and angiogenesis and assists cancer cells in immune escape. Ustuner et al. reported worse survival in adult patients with RMS with high LDH levels upon presentation compared to patients with levels within the normal range (32). Our results demonstrated a similar finding, in which patients with pretreatment LDH levels >400 U/l showed a worse outcome than those with LDH levels <400U/l. Thus, LDH level may be a predictor of sinonasal RMS outcomes in children and adults.
The IRSG clinical group for RMS is another prognostic factor based on postoperative residual disease and evidence of regional and distal metastasis. Siddiqui et al. analyzed 157 cases of pediatric sinonasal RMS from the National Cancer Database and reported worse survival in more advanced IRSG clinical group (I, 85.7%; II, 80.0%; III, 40.0%; IV, 24.4%) (19). Li et al. analyzed 40 adult patients with sinonasal RMS from a single center and showed that the IRSG clinical group was an independent prognostic factor for overall survival (16). The results of the present study did not demonstrate a significant correlation between IRS clinical group and survival. The reason may be the limited sample size, with only one, four, and three cases in IRSG clinical groups II, III, and IV, respectively.
Based on the tumor location and size, as well as the presence of regional or distant metastasis, RMS can be divided into stages I to IV. Owing to its anatomical complexity and proximity to critical structures, the sinonasal region is considered an unfavorable site. Therefore, sinonasal RMS is classified as stage II or higher. Li et al. reported a better prognosis in patients with stage II sinonasal RMS (16). In the multivariate regression, however, stage was not a significant prognostic predictor, consistent with the findings reported by Siddiqui et al. (19). We also observed better survival in patients with stage III disease at the time of diagnosis compared to that in patients with stage IV disease in both groups, including or excluding patients <18 years of age; however, these differences were not statistically significant (p=0.231, p=0.063). The IRSG staging system may play a limited role in predicting the prognosis of sinonasal RMS; however, more research with larger sample sizes and thorough staging is needed to confirm this finding.
The current treatment for RMS is a risk-based strategy comprising chemotherapy, surgery, and radiotherapy. According to the IRSG-TNM stage, IRSG clinical group, and histological type, the risk was classified as low, intermediate, or high. The most commonly used chemotherapy regimens are vincristine, actinomycin D, and cyclophosphamide (VAC); vincristine, dactinomycin, and ifosfamide (VAI); vincristine, ifosfamide, and etoposide (VIE). The results of the Intergroup Rhabdomyosarcoma Study-IV showed that these treatments were equally effective for patients with non-metastatic RMS (33). Due to the anatomical complexity of the sinonasal region, complete tumor excision is difficult. However, some studies have shown that surgical excision is an alternative for some early-stage sinonasal RMS (13, 34). The recent reports of the genomic and molecular landscapes suggest the potential for immunotherapy and targeted therapy as viable treatment strategies (35).
Due to the rarity of the disease, the major limitation of this study was the small number of patients with sinonasal RMS. Therefore, additional studies with larger sample sizes are needed to verify the prognostic factors. Multi-centered studies may be arranged to resolve this issue.
In conclusion, we observed a predominance of male sex and alveolar type in sinonasal RMS. Patients with pretreatment LDH levels >400 U/l and desmin or MyoD1 negativity had significantly poorer survival rates. These factors help predicting patient outcomes in sinonasal RMS.
Acknowledgements
This work was supported by the Taipei Veterans General Hospital, Taipei, Taiwan, R.O.C. (Grant numbers V111B-006).
Footnotes
Authors’ Contributions
Lo WL and Yeh CF conceived of the presented idea and design of study. Lo WL, Huang WH and Yeh CF acquired the data. Lo WL and Yeh CF analyzed and/or interpreted the data. Lo WL and Yeh CF drafted the manuscript. Yeh CF revised the manuscript critically for important intellectual content. Lo WL, Huang WH and Yeh CF approved the version of the manuscript to be published.
Conflicts of Interest
The Authors declare that they have no competing interests in regard to this study.
- Received August 12, 2022.
- Revision received September 14, 2022.
- Accepted September 19, 2022.
- Copyright © 2022, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).