

Abstract
Background/Aim: Silicone implants are widely used biomaterials in surgeries owing to their physiological inertness and low toxicity. However, capsular contracture is a severe complication caused by the insertion of breast implants, which can endanger the health of patients. In this study, twelve different silicone breast implants were tested to determine which could lead to a lower incidence of capsular contracture. Materials and Methods: For in vivo experiments, these silicone implants were implanted into 60 rats (i.e., five implants per rat). The implants were explanted eight weeks after the operation. Samples were analyzed and measured by using hematoxylin and eosin staining, Masson’s trichrome staining, and immunofluorescence staining methods. We compared twelve samples for their differences in the thickness of capsular formation, number of inflammatory cells, collagen expression, fibroblast intensity (i.e., Vimentin and α-SMA), and inflammatory cytokines (i.e., IL-8, CD68, MCP-1, and F4/80). Results: Different surface textures of breast implants gave different effects on capsular thickness, collagen formation, fibroblast formation, and potential inflammation. Samples that had smooth textures such as SEBBIN, HANS, and Mentor showed higher collagen formation than other samples. SEBBIN Texture, Motiva Micro, HANS Smooth I, and HANS Micro exhibited higher fibroblast formation (i.e., α-SMA, Vimentin). SEBBIN Smooth and samples in HANS group displayed lower expression of inflammation cytokines (IL-8, CD68, MCP-1, and F4/80). Conclusion: These findings provide preliminary reports on the surface texture effect and support a selection of breast silicone implants in breast reconstruction to avoid the formation of capsular contracture after implantation.
- Silicone implants
- capsular contracture
- anaplastic large cell lymphoma
- bacterial biofilms
- surface texture
Silicone breast implants are frequently used in cosmetic augmentation and post-mastectomy breast reconstruction. Since their first therapeutic application in 1960, implant manufacture, materials and surgical techniques have progressed. The safety of breast silicone implants has been thoroughly researched. Spontaneous breakage and silicone gel leak have been considerably reduced following an increase in device standards (1, 2). In 2020, the Plastic Surgery Statistics Report indicated that 193,073 breast reconstruction surgeries had been accomplished – ranking fifth in all cosmetic surgical procedures. Unfortunately, with an occurrence of over 10%, this operation is frequently followed by the formation of capsular contracture (CC), which has been found to be one of the most important reasons for revision breast surgery.
Medically, capsular contracture (CC) occurs mostly in the context of complications from breast implants. The host tissue recognizes the breast implant as a foreign body and triggers an immune reaction, which can lead to the creation of new collagen fibers in the capsule around the implant (3, 4). Although the chronic inflammatory reaction of the body to the foreign object results in the creation of capsular tissue around the implant, this response can sometimes be excessive and cause the collagen-fiber capsule to shrink, tighten, and compress the breast implant, leading to a rigid and malformed breast (5, 6). In addition, long-term capsular contracture and T-cell response may lead to breast implant-associated anaplastic large cell lymphoma (BIA-ALCL) (7, 8).
The etiology of capsular contracture is not completely understood. The position of the wound area, hypertrophic scars, excessive inflammatory reaction, formation of biofilm, allergy to surgical glove powders or silicone gel leak have all been cited as possible causes of the formation of capsular contracture (9). Among all the risk factors, the most common etiology for the development of capsular contracture is still the establishment of a biofilm deposit on the surface of implants (10, 11). Biofilm production together with implant surface morphology and genetic susceptibility, are thought to trigger the development of BIA-ALCL. Although several studies have demonstrated the influence of the biofilm layer and implant surface characteristics on capsular contraction and BIA-ALCL, the relationship between implant surface architecture and biofilm production has yet to be defined (5, 12, 13).
The literature demonstrates that the smooth and textured implants exhibit different rates of capsular contracture. The surface mechanism of the breast implant can significantly affect the formation of the capsule; specifically, the amount and arrangement of the collagen fibers in the capsule as well as the implant adhesion (14-16). Smooth silicone implants lead to the formation of dense capsules with highly aligned and organized collagen fibers (17, 18), whereas implants with textured surfaces cause tissue ingrowth and disorder the alignment of the surrounding capsule. The stability of collagen fibers is the reason why textured implants have lower rates of capsular contracture and malposition compared with smooth surface implants (17, 19-21). Adherence of the tissue to the implants can prevent the movement of implants in the breasts, which may decrease the risk of implant rotation and movement (22, 23). However, it is worth noting that textured implants are more likely to cause ALCL. The US Food and Drug Administration (FDA) reported in January 2011 that there might be a link between breast implants and the formation of ALCL. Following that, in July 2019, the FDA ordered a recall of textured-surface implants due to findings that BIA-ALCL and textured-surface breast implants have an association (24). In order to relieve the fibrosis and decrease the occurrence of capsular contracture, micro/nano textured implants have been developed, having the characteristics of both smooth and textured surfaces. Besides, surface modification combined with drug delivery is also receiving great attention.
Therefore, we conducted an in vivo and in vitro study to obtain information about capsules caused by breast implants. Considering the wide usage of breast implants and the occurrence of capsular contracture, it is necessary to perform more research in this field to solve this problem. Herein, we used twelve different kinds of silicone breast implants with different surface area and from different companies and evaluated how the surface of silicone implants affects the capsule formation and tissue adherence in the rat model.
Materials and Methods
Materials. PBS buffer was ordered from iNtRON Bio company (Seongnam, Gyeonggi, Korea), xylene was purchased from Duksan (Seoul, Republic of Korea), 10X sodium citrate buffer was ordered from Biosesang (Seongnam, Gyeonggi, Republic of Korea), fetal bovine serum (FBS) was purchased from GIBCO (Grand Island, NY, USA). Vimentin, F4/80 and alpha Smooth Muscle Actin antibodies were purchased from Santa Cruz Biotechnology (Dallas, TX, USA). Rat CXC2/IL-8 antibody was ordered from R&D System (Minneapolis, MN, USA). Anti-CD68 antibody was ordered from Abcam (Cambridge, UK). Alex Fluor 488 rabbit anti-mouse IgG (H+L) was purchased from Invitrogen (Carlsbad, CA, USA). The names and annotation of 12 silicone samples are shown in Table I.
Names and annotations of silicone samples.
Animal model. All in vivo animal experiments were approved by the Bundang Seoul National University and Institutional Animal Care Committee (approval BA-1802-241-014-08). Nine weeks old adult male Sprague Dawley rats weighing 200-350 g were ordered from BioOrient (Seongnam, Gyeonggi, Republic of Korea) and housed in two rats per cage. The rats were kept in a controlled environment with a temperature of 24°C, relative humidity of 55%, and a 12-h light cycle. Sixty rats were randomly divided into 12 groups. Isoflurane was used to anesthetize the rats, and the dorsal hair was shaved with a shaving machine. Betadine was used to sterilize the surgical region. The dorsal side of the Sprague Dawley rats was opened by using a #15 scalpel blade, and silicone was inserted into the sub-panniculus pocket; the incision (3.0-3.5 cm long) was stitched using nylon 4/0 Ethicon (New Brunswick, NJ, USA). After disinfecting the surgical site with 70% alcohol and betadine, a light dressing was provided. The implanted rats were observed for up to 2 months.
All parts of surgical sites, including the dermis, epidermis, posterior, and anterior capsules in the dorsal area, were chosen for biopsy analysis 2 months after implantation, and the implants were retrieved. The collected tissues were fixed in 10% paraformaldehyde for 24 h at 4°C and then embedded in paraffin. The tissue samples were cut into 5 μm thick slides and histologically analyzed.
H&E staining. The tissue samples were deparaffinized twice in xylene for 3 min before being rehydrated in decreasing concentrations of ethanol; twice in 100% ethanol for 3 min followed by 95%, 90%, 80%, and 70% ethanol for 3 min each and then rinsed twice with distilled water for 3 min. The tissue samples were stained with Hematoxylin for 5 min, and then rinsed twice with distilled water to remove the excess stain before being incubated in Buling reagent for 10-15 s. The tissue samples were then washed twice in distilled water for 3 min each time, incubated for 3 min in Eosin Y solution, and rinsed with 100% ethanol. After being dehydrated thrice in 100% ethanol for 3 min, the tissue samples were mounted with synthetic glue. The results of the H&E staining were analyzed using a microscope and photographs were captured. The capsular thickness was recorded in images from three different areas such as the left, middle, and right parts of the slide, and measured using the ImageJ software (Wayne Rasband, Bethesda, MD, USA).
MT staining. The tissue samples were deparaffinized, rehydrated, and stained by using a Masson’s trichrome staining kit (Sigma-Aldrich, St. Louis, MO, USA) according to the manufacturer’s guidance. Briefly, tissue samples were incubated with Bouinsat at room temperature overnight and then rinsed with distilled water until the slices were entirely clear. Tissue samples were stained for 10 min with Weigerts Hematoxylin, then washed with distilled water, and submerged for 10 min in Biebrich scarlet acid solution. The tissue samples were rinsed in distilled water first, and then incubated for 10 min in phosphomolybdic-phosphotungstic acid solution and aniline blue solution. The slides were then rinsed with distilled water and incubated in acetic acid for 3 min. Finally, dehydration with 100% ethanol for 3 min, 95% ethanol for 2 min, and 10 min in xylene was performed. One drop of mounting media was used to mount the tissue slides. The collagen fibers were analyzed by using a microscope (Zeiss Axio Scope.A1, Carl Zeiss, Göttingen, Germany).
Immunofluorescence staining. The tissue samples after deparaffinization and rehydration were boiled in 1X Antigen Retrieval Buffer diluted using 10% FBS/PBS in the microwave four times, for 5 min each. The slides were washed with 1×PBS buffer (pH 7.4) three times for 3 min each, followed by blocking of the proteins for 1 h in blocking solution containing 4% BSA in 1×PBS. Then, they were incubated at 4°C overnight with diluted primary antibodies. After that, the plates were washed with 1×PBS buffer twice, and the secondary antibodies diluted to 1:1,000 were added and incubated for 1 h at room temperature. Then, the plates were washed thoroughly with 1×PBS three times for 3 min each and cell nuclei were stained with DAPI (VECTASHIELD, Vector Laboratories, Newark, CA, USA). At last, images were obtained using a confocal microscope (Zeiss LSM 710 or LSM 800, Carl Zeiss, Göttingen, Germany).
Statistical analysis. The data are displayed as mean±standard error from three to five independent experiments and analyzed using GraphPad Prism software (GraphPad Software Inc., San Diego, CA, USA). Statistical analysis was performed by using a Student’s t-test. A p-value less than 0.05 indicated statistical significance.
Results
Measurement of capsular thickness after implantation. Capsular formation in accordance with the surface of 12 different silicone implants was examined quantitatively after eight weeks of subcutaneous implantation. The macroscopic morphology of the tissue implant interface is shown in representative cross-section images after H&E staining (Figure 1A).

Evaluation of capsule thickness. (A) The capsular thickness was measured for 12 silicone implants after eight weeks of implantation in rats by H&E staining. The dotted lines indicate the boundaries of capsules in each kind of silicone implant. (B) Quantitative analysis of capsular thickness for 12 silicone implants. Scale bar: 100 μm. (A: Allergan Smooth; B: Euro Smooth; C: Euro Texture; D: HANS Smooth I; E: HANS Smooth II; F: HANS Micro; G: Mentor Smooth; H: Mentor Texture; I: Motiva Micro; J: SEBBIN Smooth; K: SEBBIN Micro; L: SEBBIN Texture).
The different surfaces of the silicone implants present the different capsular morphologies among the different groups. Allergan Smooth, Euro Smooth, Hans Smooth I & II, Mentor Smooth, and SEBBIN Smooth were nearly identical, appearing smooth and flat with no textural depth. This morphology is caused by the collagen fibers on the capsule, which are arranged parallel to the surface. On the other hand, Euro Texture, Mentor Texture, and SEBBIN Texture contained pores and displayed complexity. HANS Micro, Motiva Micro, and SEBBIN Micro have rough, uneven texture surfaces.
The thickness of capsules was strongly associated with implantation time and the quality of implanted materials that contribute to the formation of contracted capsules. The average capsular thickness of the distinct groups was different, ranging from 132 to 374 μm. The SEBBIN Micro displayed the best capsule thickness of 132 μm among 12 different kinds of breast implants. The capsular thicknesses of Allergan Smooth, Euro Smooth, HANS Micro, SEBBIN Smooth, and SEBBIN Texture were similar and slightly higher than that of Euro Texture, HANS Smooth I & II, and Motiva Micro. However, the capsular thickness in Mentor Texture and Mentor Smooth was large, close to 400 μm (Figure 1B).
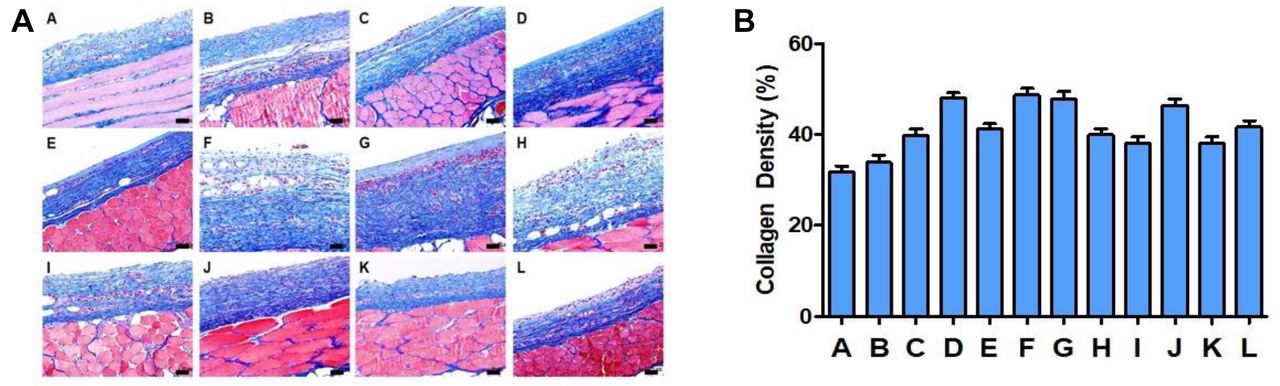
Analysis of formation of collagen fibers in capsule. The formation of capsular contracture is related to the intensity of collagen formation in capsules. The collagen fibers in capsules were visualized by MT staining (Figure 2A), and collagen intensity was measured and compared among the 12 breast implanted silicones (Figure 2B). The collagen intensity did not differ much between the 12 groups. The intensities of collagen in Allergan Smooth and Euro Smooth were the lowest, at 31% and 33%, respectively. Euro Texture, HANS Smooth II, Mentor Texture, Motiva Micro, SEBBIN Micro and SEBBIN Texture showed a similar intensity of collagen about 38-41%. The intensity of collagen was highest, at 46-48%, in SEBBIN Smooth, HANS Micro, HANS Smooth I and Mentor Smooth.

Evaluation of collagen deposition in capsules. (A) MT staining images of 12 silicone implants. Collagen fibers are presented in blue color. (B) Quantitative analysis of collagen density for 12 silicone implants. Scale bar: 50 μm. (A: Allergan Smooth; B: Euro Smooth; C: Euro Texture; D: HANS Smooth I; E: HANS Smooth II; F: HANS Micro; G: Mentor Smooth; H: Mentor Texture; I: Motiva Micro; J: SEBBIN Smooth; K: SEBBIN Micro; L: SEBBIN Texture).
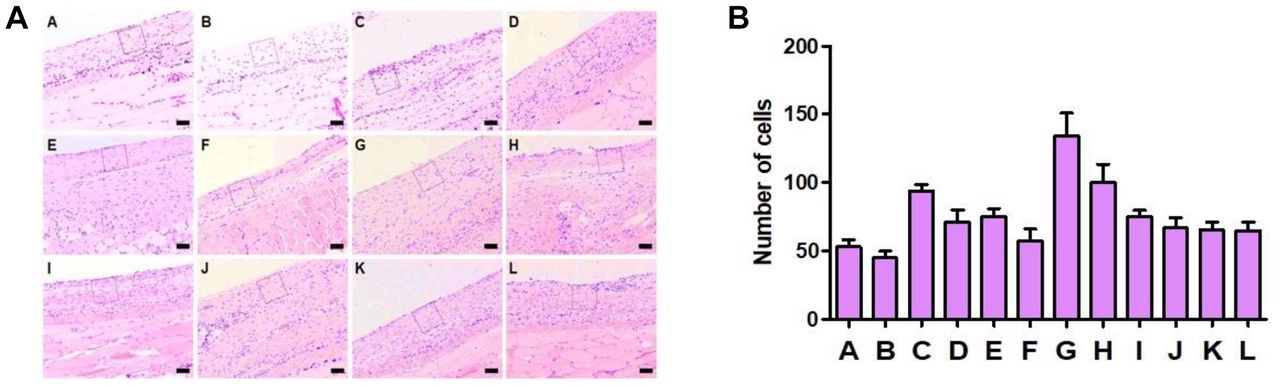
Quantification of inflammatory cells in the capsule. The proclivity of foreign materials to cause inflammation and fibrosis is a major issue linked to their implantation. A prolonged inflammatory process around a breast implant causes capsular contracture, which is a pathologic consequence. The inflammatory state is created by various reactions of many inflammatory cells. In this study, we chose a square with an area of 0.01 mm2 in the capsule close to the implant capsule interface for each group and count the number of inflammatory cells in the square (Figure 3A). The number of inflammatory cells ranged from 45 to 152 cells in all groups. Euro Smooth presented the lowest number of inflammatory cells among the 12 implanted silicones. The number of inflammatory cells in Allergan Smooth, HANS Mirco, Mentor Texture, SEBBIN Micro, SEBBIN Smooth, and SEBBIN Texture was the same while slightly higher than that in Euro Texture, HANS Smooth I & II, and Motiva Micro. However, the highest number of inflammatory cells was observed in Mentor Smooth with 152 cells compared to the other groups (Figure 3B).

Inflammatory cell counting in capsules. (A) H&E staining images of 12 silicone implants for counting cells. (B) Quantitative analysis of cell counting for 12 silicone implants. Scale bar: 50 μm. (A: Allergan Smooth; B: Euro Smooth; C: Euro Texture; D: HANS Smooth I; E: HANS Smooth II; F: HANS Micro; G: Mentor Smooth; H: Mentor Texture; I: Motiva Micro; J: SEBBIN Smooth; K: SEBBIN Micro; L: SEBBIN Texture).
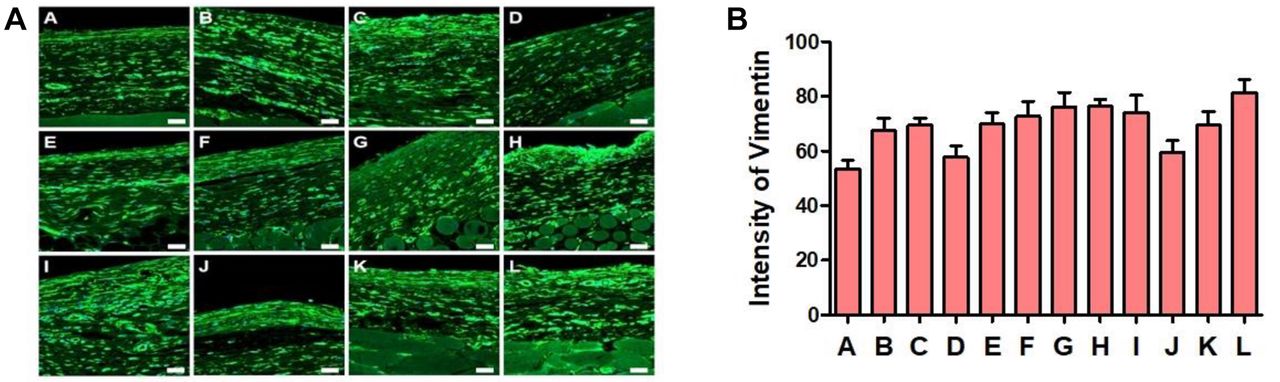
Analysis of fibroblast formation in the capsule. After silicone breast implant surgery, capsular contracture is a common consequence. Fibroblasts and macrophages are important factors in the development of capsular contracture. Vimentin and alpha SMA are known as fibroblast intermediate filament and fibroblast activation markers. In the research, Vimentin and α-SMA were quantified using the immunofluorescence (IF) staining method (Figure 4 and Figure 5). Allergan Smooth, HANS Smooth I, and SEBBIN Smooth exhibited lower intensity of Vimentin with 53 compared to other groups, while other silicone groups have a similar range from 70 to 76 (Figure 4B). And the highest intensity of Vimentin was observed at 81 in the SEBBIN Texture (Figure 4B).

Evaluation of Vimentin expression in capsules. (A) Representative fluorescence images of the intensity of Vimentin in the capsule from 12 different silicone implants were quantified by immunofluorescence staining. (B) Quantitative analysis of Vimentin intensity for 12 silicone implants. Scale bar: 50 μm. (A: Allergan Smooth; B: Euro Smooth; C: Euro Texture; D: HANS Smooth I; E: HANS Smooth II; F: HANS Micro; G: Mentor Smooth; H: Mentor Texture; I: Motiva Micro; J: SEBBIN Smooth; K: SEBBIN Micro; L: SEBBIN Texture).

Evaluation of α-SMA expression in capsules. (A) Representative fluorescence images showing the intensity of α-SMA in the capsule from 12 different silicone implants were quantified by immunofluorescence staining. (B) Quantitative analysis of α-SMA intensity for 12 silicone implants. Scale bar: 50 μm. (A: Allergan Smooth; B: Euro Smooth; C: Euro Texture; D: HANS Smooth I; E: HANS Smooth II; F: HANS Micro; G: Mentor Smooth; H: Mentor Texture; I: Motiva Micro; J: SEBBIN Smooth; K: SEBBIN Micro; L: SEBBIN Texture).
Moreover, the presence of α-SMA positive myofibroblast, which plays a key role in matrix contraction, is another maker of capsular contracture. The different intensities of α-SMA among 12 silicone implants are shown in Figure 5B. Euro Texture shows the lowest intensity of α-SMA among 12 silicone groups. And then following Allergan Smooth, HANS Smooth I & II, and SEBBIN Smooth had similar and lower intensity than the other groups. The intensity of α-SMA in Motiva Micro exhibited the highest intensity of 53 (Figure 5B).
Inflammatory cytokines. Inflammation plays an important role in capsular contracture. We also analyzed the inflammation level in capsules following implantation of 12 silicones by IF staining for four cytokine markers: IL-8, CD-68, MCP-1, and F4/80 (Figure 6, Figure 7, Figure 8, Figure 9).
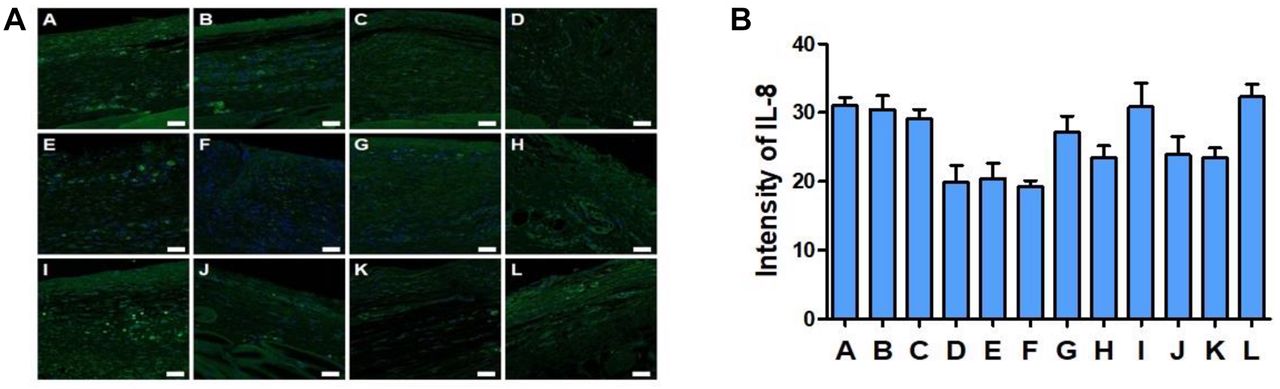
Evaluation of IL-8 expression in capsules. (A) Representative immunofluorescence images of IL-8 in capsules from 12 different silicone implants. (B) Quantitative analysis of IL-8 intensity for 12 silicone implants. Scale bar: 50 μm. (A: Allergan Smooth; B: Euro Smooth; C: Euro Texture; D: HANS Smooth I; E: HANS Smooth II; F: HANS Micro; G: Mentor Smooth; H: Mentor Texture; I: Motiva Micro; J: SEBBIN Smooth; K: SEBBIN Micro; L: SEBBIN Texture).
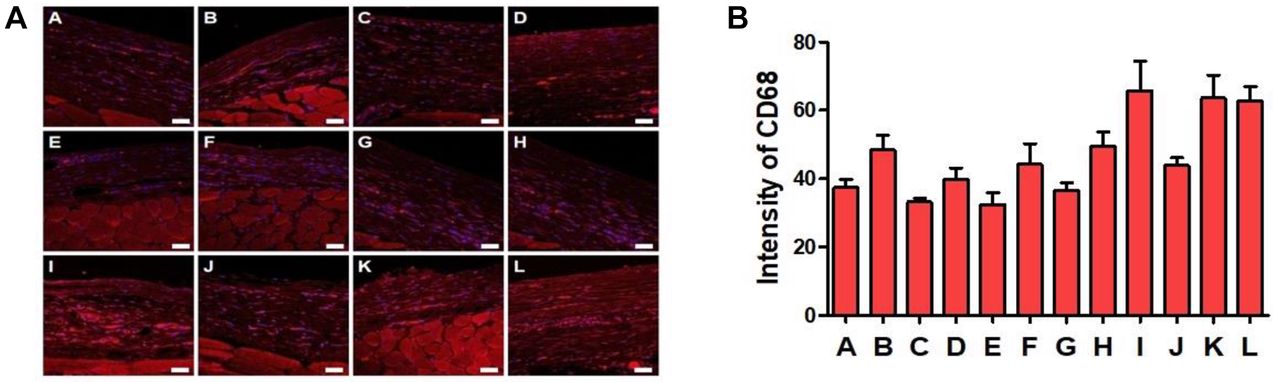
Evaluation of CD68 expression in capsules. (A) Representative immunofluorescence images of CD 68 in capsules from 12 different silicone implants. (B) Quantitative analysis of CD68 intensity for 12 silicone implants. Scale bar: 50 μm. (A: Allergan Smooth; B: Euro Smooth; C: Euro Texture; D: HANS Smooth I; E: HANS Smooth II; F: HANS Micro; G: Mentor Smooth; H: Mentor Texture; I: Motiva Micro; J: SEBBIN Smooth; K: SEBBIN Micro; L: SEBBIN Texture).
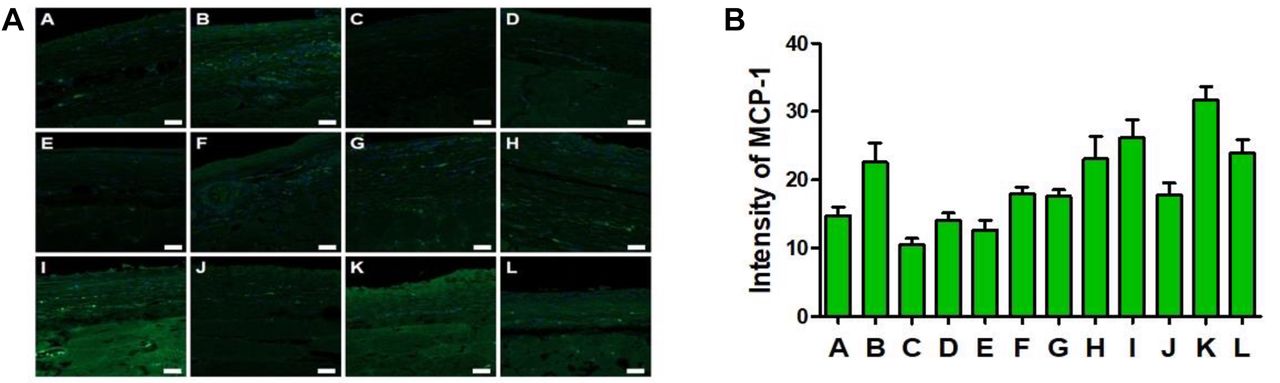
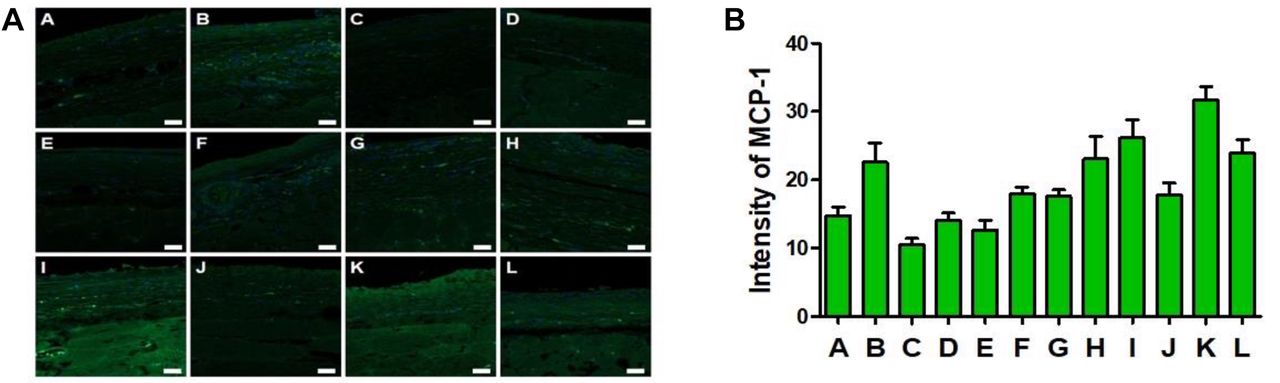
Evaluation of MCP-1 expression in capsules. (A) Representative immunofluorescence images of MCP-1 in capsule from 12 different silicone implants. (B) Quantitative analysis of MCP-1 intensity for 12 silicone implants. Scale bar: 50 μm. (A: Allergan Smooth; B: Euro Smooth; C: Euro Texture; D: HANS Smooth I; E: HANS Smooth II; F: HANS Micro; G: Mentor Smooth; H: Mentor Texture; I: Motiva Micro; J: SEBBIN Smooth; K: SEBBIN Micro; L: SEBBIN Texture).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Evaluation of F4/80 expression in capsules. (A) Representative immunofluorescence images of F4/80 in capsules from 12 different silicone implants. (B) Quantitative analysis of F4/80 intensity for 12 silicone implants. Scale bar: 50 μm. (A: Allergan Smooth; B: Euro Smooth; C: Euro Texture; D: HANS Smooth I; E: HANS Smooth II; F: HANS Micro; G: Mentor Smooth; H: Mentor Texture; I: Motiva Micro; J: SEBBIN Smooth; K: SEBBIN Micro; L: SEBBIN Texture).
IL-8 staining intensity was different among 12 silicone implanted groups ranging from 18 to 32 (Figure 6A and B). All silicones belonging to HANS group displayed lower expression of IL-8 than that in other groups. IL-8 expression was similar in Mentor Texture, SEBBIN Micro, and SEBBIN Smooth. However, Allergan Smooth, Euro Smooth, Euro Texture, Mentor Smooth, Motiva Micro, and SEBBIN Texture had higher expression of IL-8 compared to other groups (Figure 6B).
CD68 is a biomarker of macrophages. CD68 varied between implanted groups (Figure 7A and B). As shown in Figure 7B, HANS Smooth II and Euro Texture had the lowest levels of CD68 at 32, compared to other groups. The levels of CD68 expression in Allergan Smooth, HANS Smooth I, HANS Micro, and Mentor Smooth were slightly higher. In contrast, Motiva Micro, SEBBIN Micro, and SEBBIN Texture significantly exhibited a CD68 intensity higher than 60 (Figure 7B).
Expression of MCP-1 was also examined in all implanted silicones using IF staining (Figure 8A and B). MCP-1 is a crucial chemokine that attracts and induces monocyte migration from the bloodstream to become tissue macrophages. MCP-1 expression was the lowest in Euro Texture at 10, among the 12 implanted silicones (Figure 8B). Sequent, HANS Smooth I & II, Allergan Smooth, Mentor Smooth, HANS Micro and SEBBIN Smooth expressed similar levels of MCP-1 ranging from 12 to 19, which were slightly higher levels compared to Euro texture. SEBBIN Micro showed the highest expression of MCP-1, which was measured at 32 (Figure 8B).
F4/80 is a mature mouse cell surface glycoprotein expressed at high levels on various macrophages (Figure 9A and B). It is regarded as a unique marker of murine macrophages. The results of IF staining and the bar chart show that the intensity of F4/80 in the SEBBIN Smooth group was the lowest (at 20), followed by that in the Euro Texture group. F4/80 intensities in HANS Smooth II, HANS Smooth I, and HANS Micro were slightly higher than Euro Texture, ranging from 30 to 32. Allergan Smooth group, which is regarded as the control group in the experiment, ranked seventh in the intensity among all the groups, at 36. The highest intensity appeared in the Motiva Micro group, which was over two times the lowest one (Figure 9B).
In short, the results obtained for the different cytokines among the 12 different types of silicone implants indicated that each silicone implant exhibited different expression levels of inflammatory cytokines.
Discussion
The most common issue following breast augmentation and reconstruction with breast implants is capsular contracture. Despite the fact that the cause of capsular contracture is uncertain, several researchers have focused on risk factors such as immunological variables, bacterial contamination, and surgical technique. Although none of the ideas are conclusive, there is agreement that the breast reconstruction technique and the surface of the implants are additional contributing elements.
The goal of our research is to elucidate how the surface of implants affects the development of capsular contracture. Understanding the physical features of implant surfaces by analyzing the surface of implants can help us to understand how a surface may affect tissue response. Such histological findings can prepare the ground for a deeper understanding of implant surface texture aspects. It is worth mentioning that surface texture variances can occur in the same type of breast implant, which could indicate differences in the manufacturing process. Moreover, the materials of silicone implants manufactured by different companies may be incompatible. It is critical to understand the changes in surface texture, which play a key role in capsular development. Further, detailed assessments of the implant surface, like texturing surface area and roughness, will be carried out in the future, allowing for a more thorough comparison.
Fibroblasts are one of the major cell types involved in breast capsular contracture due to the deposition of the extracellular matrix and the synthesis of collagen (25, 26). The breast capsular thickness becomes thicker with time of implantation, indicating that fibroblasts continue depositing collagen fibers in the capsule (27, 28). A chronic inflammatory reaction may explain this. When the implant is inserted into the body, the white blood cells, including neutrophils, basophils, mast cells and eosinophils known as polymorphonuclear leukocytes (PMNs) will travel to the site of implantation and release cysteinyl leukotrienes, which are strong lipid inflammatory mediators. Fibroblasts are stimulated to migrate and multiply when they are exposed to leukotrienes. Fibroblasts secrete TGF-β, produce collagen and develop into myofibroblasts. And capsular contracture occurs as a result of these changes (29-31). In our research, we evaluated the intensity of Vimentin, which is known as a fibroblast marker and plays a critical role in determining tissue compatibility, fibrosis, and wound healing, in all types of silicone implants. The results indicated that all silicone implants did not differ significantly regarding Vimentin intensity and ten of twelve silicone implants exhibited similar levels of expression of Vimentin. In contrast, Allergan Smooth, HANS Smooth and SEBBIN Smooth showed slightly decreased intensity compared to other groups.
Moreover, myofibroblasts are elastic fibroblasts that are typically found in capsular architecture and actively participate in wound closure during healing (32). Myofibroblasts have been studied for their function in the formation of capsular contracture. Myofibroblasts create a contractile force that reduces the area of the capsular surface as the collagen network remodels and stabilizes the contracture (21). Properly activated fibroblasts evolve into protomyofibroblasts with limited contractility, then converted into myofibroblasts with the ability to generate significant contractile forces (27). The number of myofibroblasts observed in the capsule is commonly used as an appraisal marker to determine the degree of fibrosis because a higher number of myofibroblasts in the capsule generates greater contraction and thus stronger pressure on the implant. This will lead to implant deformation and discomfort of patients (33). However, previous research demonstrated the expression of Vimentin and α-SMA, which indicate the level of collagen deposition, is used to assess the compatibility of implant materials. High levels of Vimentin and alpha-SMA expression indicate that more collagen was generated during this period. The capsule can be thick, more likely to shrink, and finally cause capsular contracture (32, 34). α-SMA is a differentiated myofibroblast maker whose expression in the capsule is measured using IF staining. Our results indicate that the degree of expression of α-SMA was lowest in Allergan and Euro Texture at 28 and 27, respectively. And other silicone groups had similar α-SMA expression levels but slightly increased. These findings indicate that the degrees of expression of fibroblast and myofibroblast among 12 silicone implants were at different levels because they differ in implant materials, structure, and manufacturing.
The production of collagen around a silicone implant that has progressed beyond the typical thick barrier to become a powerful and thick covering that thickens and contracts across the full surface of the breast implant is known as capsular contracture. Fibroblasts have been connected to the initial development of the capsule because they produce collagen. The majority of the tissue in capsule is composed of consistently dispersed collagen fibers, according to histological analysis (25, 28). This indicates that the degree of collagen expression in the capsule after silicone implants depends on capsular thickness as well as the expression of fibroblasts and myoblasts in the capsule. Our research showed that the capsular thickness differed significantly among 12 silicone implants. However, the levels of collagen expression showed the same trend as the degree of Vimentin and α-SMA expression. Collagen intensity in Allergan Smooth was the smallest among the 12 breast silicone implants. Minami and colleagues found that smooth implants often lead to thicker capsules with a higher proportion of thick collagen fibers (35). This is consistent with our results showing that HANS Smooth I &II, SEBBIN Smooth, and Mentor Smooth had the highest degree of collage expression compared to other silicone implants.
Interestingly, Allergan Smooth and Euro Smooth displayed the lowest level of collagen intensity. This result may indicate differences in the materials of silicone implants and production technology. Besides, texture silicone implants have surface with pores and the collagen fibers can develop multidirectionally. Collagen expression in textured implants was lower than that in smooth implants. This finding as agrees with the previous study (26). The implant is more stable because of the interaction between the textured-surface implant and surrounding tissue, which may be linked to a lower risk of capsular contracture. By controlling the roughness of the existing textured surface on the microscale, micro-textured implants acquire both smooth and textured surfaces. The occurrence of capsular contracture will eventually decrease owing to the reduction of inflammation and fibrosis.
The capsular contracture in breast silicone implants could be associated with an increase in overall capsular thickness related to the non-collagen layer and a high amount of collagen matrixes in the capsules. In addition, another factor that also contributes to forming the capsular contracture is inflammation. A fibrotic process is triggered when insertion of silicone implants into the body causes the development of inflammation, and the foreign body reaction happens during the chronic inflammatory phase (36). During the inflammatory stage, various cytokines such as IL-8, CD68, IL-6, IL-1β, MCP-1, and F4/80 are secreted. In our research, we counted the number of inflammatory cells (Figure 3) and also analyzed the expression of several inflammatory cytokines in the capsule using IF staining. IL-8 is a chemokine generated mainly by macrophages and has an important function in the inflammatory process, owing to its powerful chemokine actions on neutrophils. Neutrophils were found in higher numbers in constricted breast capsules, which is associated with an enhanced expression of IL-8 (37). The intensity of IL-8, in our study, was different between the 12 silicone implants and all implants belonging to HANS implants showed similar levels but comparatively the lowest expression. In contrast, Allergan Smooth, Euro Smooth, Euro Texture, Mentor Texture and SEBBIN Texture exhibited the highest expression. These findings may imply that enhanced IL-8 released by macrophages and fibroblasts at the breast capsule could increase angiogenesis in contracted breast capsules, leading to greater fibrosis and the development of capsular contracture. Moreover, CD68, MCP-1, and F4/80 are the markers for inflammatory infiltration. The levels of these cytokine were significantly different in the capsules between the 12 silicone implants showing the same trend. The lower levels of expression of CD68, MCP-1 and F4/80 were observed in the HANS silicones among all silicone implants. The little presence of these cytokine markers in the capsular formation demonstrates that the inflammatory process is inhibited owing to the lack of macrophages.
Conclusion
Our research aimed to investigate the formation of capsular contracture in 12 silicone implants with differences in surface texture, materials, and technology. We examined the capsular thickness, the level of collagen expression, and the presence of Vimentin positive fibroblasts, α-SMA positive myofibroblasts, inflammatory cells and the levels of inflammatory cytokines such as IL-8, CD68, MCP-1, and F4/80. Our findings provide a better view regarding the effects of breast implants’ surface texture features, allowing us to categorize the implants into different categories based on their surface morphology. Moreover, this study facilitates the selection of breast silicone implants that lead to a lower incidence of capsular contracture, which is important in breast augmentation.
Acknowledgements
This research was funded by grant No. 14-2017-0019 from SNUB Research Fund and supported by a grant of the Korea Health Technology R&D Project through the Korea Health Industry Development Institute (KHIDI), funded by the Ministry of Health & Welfare, Republic of Korea (Grant number : HR22C1363).
Footnotes
Authors’ Contributions
Conceptualization: C. Y. Heo and S. Y. Nam; methodology: S. Y. Nam, P. N. Chien; validation: S. Y. Nam, P. N. Chien; formal analysis: S. Y. Nam, P. N. Chien, X.R. Zhang; data curation: X.R. Zhang; writing: X.R. Zhang, P. N. Chien, X.T. Trinh, and S. Y. Nam; supervision: C. Y. Heo. All Authors have approved the final version of the manuscript submitted for publication and agree to be accountable for all aspects of the work.
Conflicts of Interest
The Authors declare no conflicts of interest regarding this study.
- Received July 29, 2022.
- Revision received August 26, 2022.
- Accepted August 29, 2022.
- Copyright © 2022, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).