

Abstract
Background/Aim: To clarify the clinical significance of measuring the mean corpuscular volume (MCV) of red blood cells before applying neoadjuvant chemotherapy (NAC) in patients with locally advanced esophageal squamous cell carcinoma (ESCC) who will receive NAC followed by curative resection. Patients and Methods: We retrospectively investigated 169 eligible patients at the Kanagawa Cancer Center between 2011-2018. The patients were divided into high and low-MCV groups. The cutoff value of the MCV was determined by the maximum χ2 statistic value on the log-rank test and was set at 92.8 fl. Clinicopathological features and outcomes were compared between the two groups. Results: There was no significant association between the MCV and clinicopathological features. Both five-year recurrence-free survival (RFS) and overall survival (OS) in the high-MCV group were significantly poorer than those in the low-MCV group (RFS, p=0.026; OS, p=0.006). On multivariate analysis, a high-MCV was an independent predictive survival factor for RFS [hazard ratio (HR)=1.728; 95% confidence interval (CI)=1.033-2.891; p=0.037] and OS (HR=1.836; 95%CI=1.002-3.365; p=0.049). Conclusion: Measurement of the MCV before NAC may be a useful prognostic biomarker in patients with locally advanced ESCC who will receive NAC followed by curative resection.
- Esophageal squamous carcinoma
- mean corpuscular volume
- neoadjuvant chemotherapy
Esophageal cancer is the seventh most common cancer and the sixth leading cause of cancer-related deaths worldwide (1). More than 600,000 new cases and an estimated 400,000 deaths are recorded annually worldwide (2). The current standard treatment for locally advanced esophageal squamous cell carcinoma (ESCC) is neoadjuvant chemotherapy (NAC) followed by complete resection (3). However, the prognosis of most patients with locally advanced ESCC remains poor. Therefore, personalized treatment using predictive biomarkers such as response to chemotherapy or survival can be helpful to improve outcomes in patients with locally advanced ESCC.
Mean corpuscular volume (MCV) is an index that describes the average volume of a red blood cell (RBC) and is one of the most commonly used clinical hematological parameters. MCV is associated with alcoholic polydipsia. It was reported that alcoholic polydipsia often decreases folic acid and vitamin B12 levels due to poor intake of folic acid and increased urinary excretion (4, 5). This mechanism inhibits the maturation of, and so weakens, blood cells. In addition, folic acid deficiency promotes hemolysis, lowering the RBC count, and so increasing the MCV. Thus, the MCV is commonly used to detect megaloblastic anemia due to vitamin B12 and folic acid deficiency (6, 7). The predictive role of the MCV in various solid tumors has received increasing attention in recent years. A high MCV is reportedly relevant to the incidence and prognosis of several malignancies, including esophageal cancer (8-11).
Since the MCV varies before and after chemotherapy (12, 13), it is unclear whether pre-treatment MCV can be useful as a biomarker for ESCC patients receiving NAC. Previous studies have reported that pre-treatment MCV is useful in predicting response to chemoradiotherapy (14).
In this study, we aimed to investigate whether measuring the MCV before NAC might be a prognostic biomarker in ESCC patients who will receive NAC followed by curative resection.
Patients and Methods
Ethical approval. Approval was obtained from the Institutional Review Board of the Kanagawa Cancer Center before the initiation of this study (approval number: 2021 epidemiological study-3). Written informed consent for using clinical data without identifying personal information was obtained from each patient before surgery.
Patients. We retrospectively investigated consecutive patients with esophageal cancer who had undergone esophagectomy at the Kanagawa Cancer Center between January 2011-December 2018. The inclusion criteria were as follows: 1) histologically proven primary ESCC located in the thoracic esophagus, 2) clinical stage II or III disease diagnosed according to the 8th edition of the Union for International Cancer Control TNM classification (15), and 3) history of NAC with cisplatin and 5-fluorouracil followed by complete resection (R0) with radical lymphadenectomy. The exclusion criteria were as follows: 1) history of NAC with agents other than cisplatin and 5-fluorouracil or history of chemoradiotherapy, 2) history of incomplete (R1 or R2) resection, and 3) history of esophagectomy as a salvage treatment.
Treatment procedure. As per the protocol of the Japan Clinical Oncology Group 9907 study, NAC was administered to patients with esophageal cancer stage II or III, prior to surgery (3, 16). Cisplatin and 5-fluorouracil were administered as neoadjuvant treatments twice every three weeks. Surgical resection was performed four to six weeks after completing chemotherapy, using standard procedure techniques. The first consists of an open subtotal esophagectomy via right thoracotomy, while the second is a thoracoscopic subtotal esophagectomy with reconstruction using a gastric tube put through the retrosternal route or posterior mediastinal route, with anastomosis through the cervical incision. Although a three-field lymphadenectomy is generally performed, a two-field lymphadenectomy is selected for ESCC located in the lower thoracic or abdominal esophagus. We routinely constructed a feeding tube into the stomach or duodenum, and enteral nutrition was initiated. Follow-up after surgery was performed every three months during the first year, and every six months for the subsequent two to five years. Physical examinations, blood chemistry, including tumor markers, and computed tomography scans from the neck to the abdomen were performed to evaluate the recurrence of esophageal cancer. When recurrence was suspected, additional imaging studies, such as positron emission tomography, were performed.
Data collection. All clinical, surgical, pathological, and survival data were retrospectively collected from the clinical databases and records. Data on body mass index (BMI) and physical status, as defined by the American Society of Anesthesiologists, were routinely collected before neoadjuvant chemoradiotherapy. Postoperative infectious complications that occurred during hospitalization or within 30 days of surgery were retrospectively identified from the patients’ medical records, and were defined as grade II or higher in severity using the Clavien-Dindo Classification (17), which identified specific factors including anastomotic leakage, pneumonia, abdominal abscess, surgical site infection, and pyothorax.
The pathological response to chemotherapy was assessed using the Japan Esophageal Society pathological criteria for the effects of chemotherapy (18). This pathological response was classified into six categories according to the proportion of viable cancer cells to the necrotic and degenerated cells in the tumor: in grade 3, no viable cancer cells are evident; in grade 2, viable cancer cells account for less than 1/3 of tumor tissue, while other cancer cells are severely degenerated or necrotic; in grade 1b, viable cancer cells account for 1/3 or more, but less than 2/3 of tumor tissue; in grade 1a, viable cancer cells account for 2/3 or more of tumor tissue; and in grade 0, there is no evidence of cytological or histological therapeutic effect. Patients were defined as responders when the histological grade was 2 or 3, and as non-responders when the grade was 0, 1a, or 1b.
Blood tests. MCV was calculated by dividing the hematocrit level by the RBC count. Laboratory factors, including pre-treatment serum MCV, were obtained within three days of initiating NAC. We determined the optimal cutoff value for the MCV for recurrence-free survival (RFS) using X-tile software (version 3.6.1; Yale School of Medicine, New Haven, CT, USA) (19). X-tile plots present a new tool for the assessment of biological relationships between a biomarker and outcome, and the discovery of population cutoffs based on marker expression. X-tile software can be used to divide patients into subgroups (e.g., tertiles and quartiles) by determining the optimal cutoff points of a continuous or categorical variable based on the maximum χ2 statistic value on the log-rank test. The optimal cutoff value for the MCV for recurrence was determined as 92.8 fl. Patients with an MCV of <92.8 and 392.8 fl were classified into the low-MCV and high-MCV groups, respectively.
Statistical analyses. We compared patient characteristics using Fisher’s exact test and the chi-square test. We defined overall survival (OS) as the time from starting the NAC to death from any cause, and RFS as the time from starting the NAC to the detection of recurrence or death, whichever came first. We discontinued data collection for patients who had not experienced an event until the date of their last follow-up visit. The survival rate was analyzed by plotting the Kaplan-Meier graph and differences in survival rates were assessed using the log-rank test. Univariate and multivariate analyses using a Cox proportional-hazards regression model were performed to explore prognostic factors for survival. All statistical analyses were performed using EZR ver. 1.37 (Jichi University, Tochigi, Japan) (20). All two-sided p-values of <0.05 were considered as statistically significant.
Results
Patient characteristics. A total of 193 patients were diagnosed with ESCC stage II or III between January 2011 and December 2018. Of these, 24 patients were excluded from the study: nine patients received chemoradiotherapy, nine received chemotherapy with triplet regimens during clinical trials, five underwent noncurative resection, and one had neuroendocrine carcinoma as the pathological diagnosis. Ultimately, 169 patients were included in this study, and among them, 112 and 57 patients were classified into the high-MCV and low-MCV groups, respectively. The median follow-up period was 46.40 [interquartile range (IQR)=4.70-121.27] months. The associations between the MCV and clinicopathological features are summarized in Table I. There were no differences between the two groups, except for sex (p=0.004).
Association between preoperative mean corpuscular volume and clinicopathological features.
Survival analysis. The 5-year RFS rate was significantly lower in the high-MCV group than in the low-MCV group (42.1% vs. 63.3%, p=0.026; Figure 1). The univariate analysis revealed clinical T factor, clinical N factor, clinical stage, pathological response, and the MCV as significant factors for RFS. The multivariate analysis revealed clinical T factor, clinical N factor, pathological response, and the MCV as independent predictive factors for RFS (Table II). The 5-year OS rate was significantly lower in the high-MCV group than in the low-MCV group (52.0% vs. 72.4%, p=0.006; Figure 2). In the univariate analysis, sex, clinical T factor, clinical N factor, clinical stage, pathological response, and the MCV were significant factors for OS. In the multivariate analysis, only the MCV was an independent predictive factor for OS (Table III).

Kaplan-Meier curves for recurrence-free survival and overall survival according to MCV level. (A) The 5-year RFS rate was significantly lower in the high-MCV group than in the low-MCV group (42.1% vs. 63.3%, p=0.026, log-rank test). (B) The 5-year OS rate was significantly lower in the high-MCV group than in the low-MCV group (52.0% vs. 72.4%, p=0.006, log-rank test).
Univariate and multivariate analyses for recurrence-free survival.

Kaplan-Meier curves for recurrence-free survival by pathological response. (A) In responders, the 5-year RFS rate was not significantly different between the high- and low-MCV groups (58.0% vs. 84.4%, p=0.148, using the log-rank test). (B) In non-responders, the 5-year RFS rate was significantly lower in the high-MCV group than in the low-MCV group (34.8% vs. 56.6%, p=0.036, log-rank test).
Univariate and multivariate analyses for overall survival.
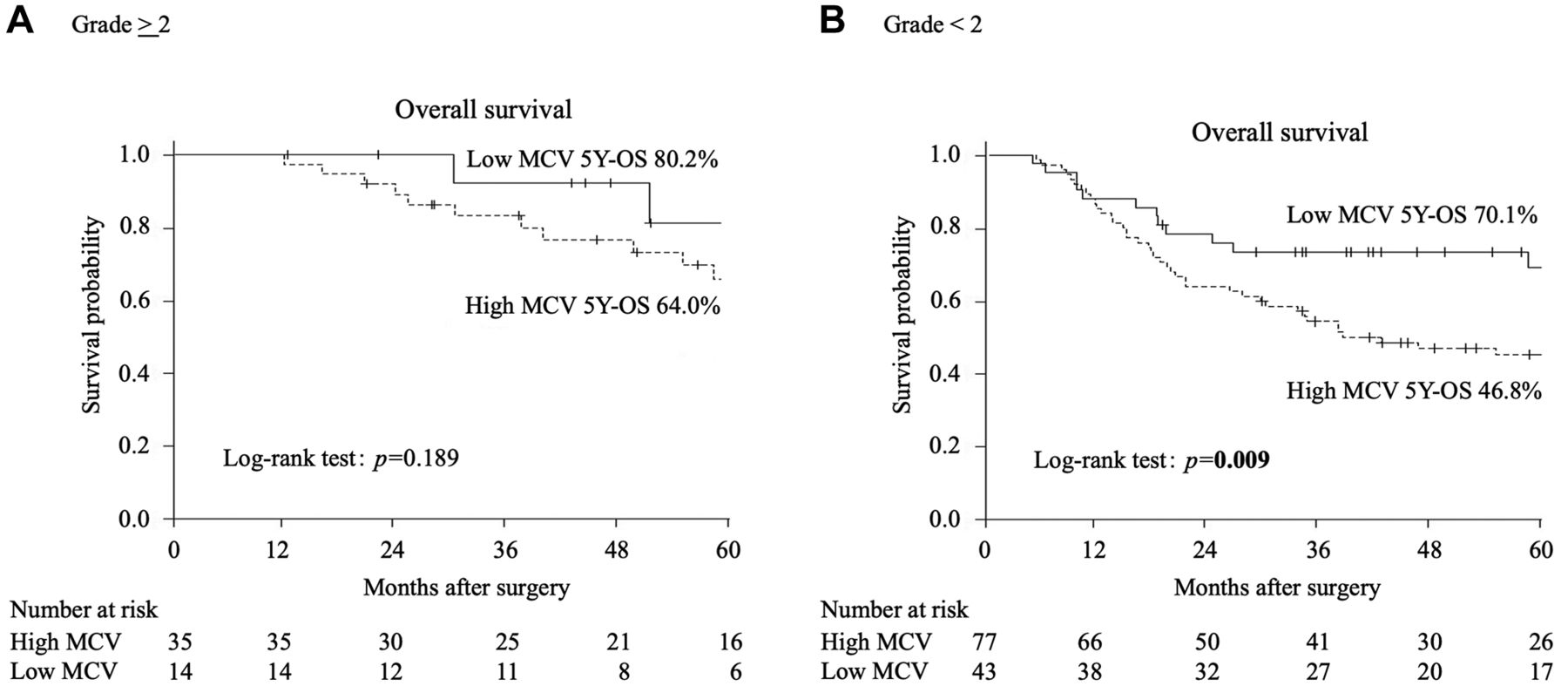
RFS and OS stratified by pathological response. The RFS and OS curves stratified by pathological response are shown in Figure 1B and C, respectively. In responders, the 5-year RFS rate was not significantly different between the high- and low-MCV groups (58.0% vs. 84.4%, p=0.148; Figure 2A). In non-responders, the 5-year RFS rate was significantly lower in the high-MCV group than in the low-MCV group (34.8% vs. 56.6%, p=0.036; Figure 2B). In responders, the 5-year OS rate was not significantly different between the high- and low-MCV groups (64.0% vs. 80.2%, p=0.189; Figure 3A). In non-responders, the 5-year OS rate was significantly lower in the high-MCV group than in the low-MCV group (46.8% vs. 70.1%, p=0.009; Figure 3B).
{kind=link}
{kind=link}
{kind=link}
Kaplan-Meier curves for overall survival by pathological response. (A) In responders, the 5-year OS rate was not significantly different between the high- and low-MCV groups (64.0% vs. 80.2%, p=0.189, using the log-rank test). (B) In non-responders, the 5-year OS rate was significantly lower in the high-MCV group than in the low-MCV group (46.8% vs. 70.1%, p=0.009, using the log-rank test).
Discussion
This study demonstrated that a high MCV prior to NAC is an independent factor for poorer survival, in terms of both RFS and OS, in patients with locally advanced ESCC. The significant finding of this study was that measuring the MCV before NAC may be an effective predictor of recurrence and survival in patients with advanced ESCC. Furthermore, stratification of the data based on the NAC response rate indicated that a high MCV is associated with poorer RFS and OS only in non-responders but not in responders. Our results suggest that the negative survival impact of the MCV may be negligible in patients with advanced ESCC who responded to NAC.
As for why the MCV is an important factor for survival in patients with advanced ESCC, it was reported that Folic acid deficiency, reflected by the MCV, is involved in inactivating tumor suppressor genes by causing abnormal DNA methylation (21, 22). However, these previous studies did not consider the effects of NAC with 5-fluorouracil. There are several reports on the relationship between chemotherapy with 5-fluorouracil and the MCV. Jung et al. (14) and Karvellas et al. (23) reported an increase in the MCV of RBCs after therapy with 5-fluorouracil. Furthermore, Wenzel et al. (24) reported that an increased MCV, without concomitant anemia, in patients receiving 5-fluorouracil might be due to 5-fluorouracil-induced thymidylate synthase (TS) inhibition in erythroid precursor cells. The cytotoxic activity of FdUMP, which was produced by the metabolism of 5-fluorouracil, depends on TS inhibition, leading to defective DNA synthesis. The increase in the MCV tended to be higher in patients with tumor remission or stable disease than in patients with tumor progression. Thus, we considered it rational to measure the MCV immediately before NAC and examined whether it was associated with outcomes in ESCC patients.
As a standard treatment for advanced ESCC, NAC, or preoperative adjuvant radiochemotherapy has been performed globally, and 5-fluorouracil is used in both regimens. Folic acid levels are related to the effects of 5-fluorouracil on ESCC, and are reflected in the MCV. Although Li et al. (16) reported that the therapeutic effect of concurrent chemoradiotherapy may differ depending on the pre-treatment MCV levels, the MCV was not related to the pathological response in this study. However, when we stratified the patients according to the pathological response to NAC and investigated the association between pathological response and survival, the MCV was associated with RFS and OS only in pathological non-responders to NAC and not in responders. This suggests that the cytotoxic effects of NAC on micrometastasis might exceed the negative survival effects of high MCV, which was reported in previous studies.
This study has several limitations. First, this was a retrospective study at a single institution, and the number of patients was relatively small. We cannot deny the possibility that our findings could have been observed by chance. Therefore, a prospective multicenter study is required. Second, this study was conducted over a relatively long period, from 2011-2018, which can be associated with historical biases in treatment strategies and perioperative management, dictating the short-term and prognostic outcomes after esophagectomy. Third, the most accurate optimal cutoff value of the MCV remains unknown. Although we determined the optimal cutoff value of the MCV for RFS using the X-tile software in this study, previous studies employed different cutoff values. Furthermore, changes in the MCV before and after chemotherapy, and difference in the degree of change in the MCV due to therapeutic effects, have been reported.
In conclusion, measuring the MCV before NAC may be a useful prognostic biomarker in patients with locally advanced ESCC who will receive NAC followed by curative resection.
Acknowledgements
The Authors thank all the patients, their families, and the site staff for their participation in this study.
Footnotes
Authors’ Contributions
Concept and study design were conducted by HY, KK, and TO. Data collection and literature search were performed by HY, KK, IH, HS, TA, TY, TO, YR, and TO. Data analysis and interpretation were performed by HY, KK, and TO. The manuscript and figures were drafted by HY, KK, and TO. Finally, the manuscript was revised and approved by all investigators. Thus, all the Authors actively participated in this study.
Conflicts of Interest
The Authors declare that there are no conflicts of interest regarding this study.
- Received June 6, 2022.
- Revision received June 30, 2022.
- Accepted July 1, 2022.
- Copyright © 2022, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).