

Abstract
Background/Aim: Little is known regarding seizures during radiotherapy for brain tumors. This prospective study investigated seizure activity in patients irradiated for high-grade gliomas. Patients and Methods: Using a seizure diary, progression of seizure activity was evaluated in 22 patients receiving chemoradiation for grade III (n=1) or IV (n=21) gliomas. Progression was defined as increased frequency of any and/or generalized seizures (>50%) or increased anti-epileptic medication (≥25%). Patients’ satisfaction with the diary was assessed using a questionnaire (six scales of 1-7 points). Uni- and multivariable analyses were performed including baseline seizure activity, age, sex, resection, tumor site, performance score, and history of epilepsy/seizures. Results: Ten patients (45%) experienced progression of seizure activity during their radiotherapy course, mainly due to increased seizure frequency (nine patients=41%). Mean values of patients’ satisfaction scores ranged between 3.92 and 4.92 points. Conclusion: Radiotherapy of high-grade gliomas can increase seizure activity. Patients require close monitoring to initiate or adjust anti-epileptic medication.
- Seizures
- high-grade gliomas
- radiotherapy
- chemoradiation
- patient reported outcomes
Gliomas represent the most common group of primary brain tumors in adults and can cause significant morbidity (1-3). This is especially true for grade IV gliomas (glioblastoma, GBM), which according to the national central brain tumor registry (CBTRUS) represented almost 50% of malignant central nervous system tumors in the United States diagnosed between 2014 and 2018 (3). Gliomas can be associated with seizures. In previous studies, the prevalence of pre-treatment seizures ranged between 9% and 45% in patients with GBM and between 29% and 67% in patients with grade III gliomas (4-10).
Very little is known regarding the course of seizures during a radiotherapy course. However, this information would be helpful, since patients with grade III or IV gliomas generally receive post-operative or definitive radiation treatment, either alone or combined with systemic chemotherapy. Radiotherapy is known to be associated with an acute inflammatory reaction that can lead to intracerebral edema and increased intracranial pressure (11, 12). Therefore, radiotherapy may cause or aggravate neurological symptoms including focal and generalized seizures, and the patients may require initiation or adjustment of anti-epileptic treatment (12).
This prospective interventional study (SURF-ROGG) investigated seizure activity in patients irradiated for high-grade gliomas, i.e., grade III or IV tumors, during their course of treatment. It focused on patient reported data from a seizure diary. It was hypothesized that the rate of patients with progression of seizure activity was at least 30%.
Patients and Methods
This prospective interventional study investigated the seizure activity during a course of radiotherapy in patients with high-grade gliomas. The study received approval by the ethics committee of the University of Lübeck, Germany (reference 20-311) and was registered at clinicaltrials.gov (identifier: NCT04552756). Eligibility criteria were previously reported and included histologically proven grade III or IV glioma, indication for normo-fractionated radiotherapy, Eastern Cooperative Oncology Group performance score of 0-2, age ≥18 years, written informed consent, and the patient’s capacity to cooperate and keep the seizure diary (13).
The study was terminated after enrollment of 23 patients, since the required number of 10 events was already reached (see results section). Twenty-two of these 23 patients met the eligibility criteria for evaluation of their data. One patient did not qualify for the analyses since the consent to participate was withdrawn after only three fractions of radiotherapy and no valid data could be obtained.
Of the 22 evaluable patients, 9 patients were female (41%) and 13 were male (59%). Median age was 59.5 years (range=30-80 years). Twenty-one patients (95%) had GBM and 1 patient a grade III lesion (5%). The patient with grade III glioma had a grade II lesion 27 years ago, and one of the other patients had another GBM 9 months ago. Since both patients were not irradiated for initial glioma, they were eligible for the SURF-ROGG trial. The most common site of glioma was frontal lobe in nine patients (41%). Ten patients (45%) received anti-epileptic medications prior to radiotherapy, which consisted of levetiracetam (n=8), levetiracetam plus lacosamide (n=1), or valproate (n=1). Six of these patients had a history of epilepsy or seizures. In the entire cohort, 16 patients (73%) received upfront resection, which was subtotal in eight patients and gross total in eight patients. Radiotherapy was performed as volumetric modulated arc therapy. Further details of radiation treatment were previously described (13). Planned regimens included 59.4 Gy in 33 fractions of 1.8 Gy in 17 patients (77%) and 60 Gy in 30 fractions of 2.0 Gy in 5 patients (23%). Overall treatment time was generally 6 to 7 weeks. In patients with GBM, radiotherapy was planned to be combined with concurrent temozolomide (TMZ), i.e., 75 mg/m2/day including weekends during the course of radiotherapy. Concurrent treatment should be followed by six courses of TMZ with 150-200 mg/m2/d1-5 (every 4 weeks) (14). The patient with a grade III glioma had an anaplastic oligodendroglioma that was treated with post-operative radiotherapy alone followed by chemotherapy with four courses of procarbazine, lomustine, and vincristine (15).
Endpoints and assessments. Primary endpoint was progression of seizure activity during the course of radiotherapy, which was defined as an increase in the number of seizures (any type) by >50%, increase in the number of generalized seizures by >50%, and/or initiation or increase in anti-epileptic medication by ≥25%. These parameters were assessed as outcomes reported by the patients using a seizure diary during and up to 6 weeks following radiotherapy. Moreover, patients were asked to complete a questionnaire (6 items) after completion of radiotherapy regarding their satisfaction with the seizure diary and undergo electroencephalography (EEG) at the beginning, at the end, and 6 weeks after radiotherapy.
Statistical considerations. According to sample size calculations, 35 patients should be enrolled, and 32 patients should be evaluable for the analyses. With this sample size, a one-sample exact binomial test with a one-sided significance level of 2.5% had a power of 80% to yield statistical significance if seizure activity (compared to baseline prior to radiotherapy) increased in 30% of patients (alternative hypothesis) assuming a ‘natural’ progression-rate of 10% without radiotherapy (null hypothesis). For appropriate description of the time profiles of seizure activity, normalized seizure frequencies over time were calculated for certain time periods, namely weeks 1-3 and 4-6/4-7 during radiotherapy, and weeks 1-3 and 4-6 following radiotherapy. The Wilcoxon-signed rank test was used to compare each period (mean seizure frequencies) to baseline. p-Values <0.05 were considered significant, and p-values <0.20 were considered indicating a trend. Seizure activity was calculated by summing the number of seizures during each time period, dividing the sum by the number of days with available data, and multiplying this result with 7 to normalize it to a weekly rate. The rate of progression of seizure activity was calculated and the 95% exact Clopper-Pearson confidence intervals were provided. To test whether the rate of progression of seizure activity was significantly increased beyond 10%, the one-sided binomial test at a one-sided 2.5% significance level was applied. In addition, each component of the primary composite endpoint of progression was subjected to statistical analysis.
A logistic regression model was applied including seizure activity at baseline (no vs. yes), age (≤59 vs. ≥60 years), sex (female vs. male), upfront resection (no/biopsy only vs. subtotal/gross total resection), tumor site (frontal/frontoparietal vs. other single sites vs. multifocal), ECOG performance score (0 vs. 1.2), and history of epilepsy or seizures (no vs. yes). Adjusted odds ratio estimates and Wald confidence intervals (95% confidence limits) were calculated. In addition, patients were planned to receive EEGs at the beginning, the end, and six weeks following radiotherapy. EEG activity typical for epilepsy was classified as absent or present. Mean change to baseline by 50% regarding the number of patients with such EEG activity was considered clinically relevant.
Patient satisfaction with the seizure diary was assessed after completion of radiotherapy using a questionnaire including six items (i. to vi.) modified according to Schrepp et al. (16). Patients were asked to rate on six scales ranging from 1 to 7 points (one scale for each item), whether they considered the seizure diary i. comprehensible, ii. supportive, iii. simple, iv. safe, v. as expected, and vi. clear. Higher scores represented higher degrees of satisfaction. Mean values plus standard deviations and median values plus ranges were calculated for each scale from the ratings of all patients participating in this survey. To obtain the rate of patients not satisfied with the seizure diary, the scoring points of the six scales were added for each patient and divided by 6 (mean value). Mean values <4.0 were considered as dissatisfaction. If the dissatisfaction rate was >40%, the seizure diary would be considered unsuitable for patients with high-grade gliomas.
Results
Nineteen of the 22 patients (86%) received the complete planned radiation dose within the study. In one patient, chemoradiation was postponed and finally stopped after 45 Gy due to decreased performance status and grade 4 thrombopenia, one patient terminated the treatment after 54 Gy for unknown reason (no acute toxicity observed), and the study was terminated in one patient due to incompliance. In 17 of the 21 patients (81%) scheduled for concurrent chemotherapy with TMZ, this treatment was given as planned. In 4 patients (19%), chemotherapy was not given during the entire period of radiotherapy due to thrombopenia, leucopenia, and/or elevation of liver enzymes. Moreover, 3 of the 17 patients (18%), who received the complete radiation dose and did not withdraw their consent to participate in this study during its course, did not receive TMZ following radiotherapy due to decreased performance status.
Of the 22 evaluable patients, ten patients (45%) experienced progression of seizure activity during the course of radiotherapy, which was significantly increased beyond 10% (p<0.0001; exact one-sided binomial test to test) (Table I). The progression rate was mainly caused by an increase in the frequency of any type of seizures (p=0.0001). On univariable analyses of the seven investigated baseline characteristics, no significant associations with progression of seizure activity were observed (Table II). The same applied to the multivariable analysis performed as full logistic regression model (Table III).
Confirmatory analysis of the primary study endpoint, i.e., increase in seizure activity during radiotherapy, and its components.
Univariable analysis of the primary composite study endpoint stratified by baseline characteristics.
Multivariable analysis of the primary composite study endpoint stratified by baseline characteristics (full logistic regression model): Odds ratio estimates and Wald confidence intervals.
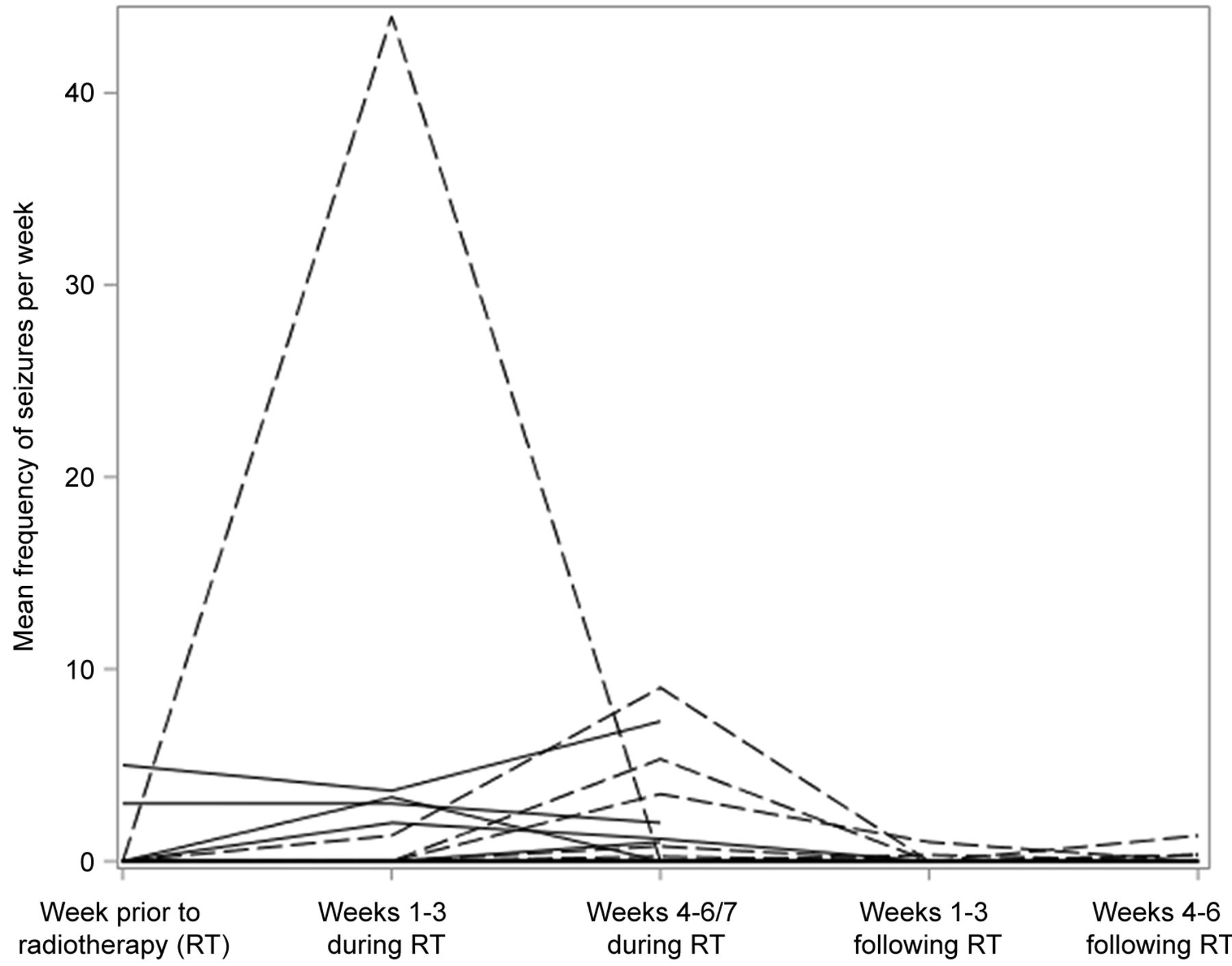
The mean seizure frequencies during the different periods of time are shown in Figure 1 and Table IV. When comparing the mean seizure frequencies during different time periods to pre-radiotherapy baseline, a significant difference was found for the period “weeks 4-6/7 during radiotherapy” (p=0.023), and a trend was observed for the period “weeks 1-3 during radiotherapy” (p=0.188). No significant increase in seizure frequency was found for periods “weeks 1-3 following radiotherapy” (p=0.50) and “weeks 4-6 following radiotherapy” (p=0.25). EEGs were available in 19/22 patients (86%) at the beginning of radiotherapy, 13/21 patients (62%) at the end of radiotherapy, and in 9/17 patients (53%) at about 6 weeks following radiotherapy. Otherwise, EEGs were refused by the patients. Of all 41 EEGs performed at different time points, only one EEG (2%) showed activity typical for epilepsy at 6 weeks following radiotherapy.

{kind=link}
Spaghetti-plot showing mean seizures per week during the different periods of time, namely during the week prior to radiotherapy (baseline), weeks 1-3 and 4-6/7 during radiotherapy, and weeks 1-3 and 4-6 following radiotherapy (see also Table IV).
Descriptive statistics of mean seizure frequencies (mean number of seizures per week) across periods of time (see also Figure 1).
Questionnaires regarding patient satisfaction with the seizure diary were completed by 13 patients (59%). Mean values of the scores given by the patients ranged between 3.92 and 4.92 points, and median values ranged between 4 and 5 points (Table V). The mean values of the points from the six scales ranged between 3.17 and 6.33 points. In five patients, the mean values were <4.0 points, representing a dissatisfaction rate of 38%.
Results of the questionnaires regarding patient satisfaction with the seizure diary. Patients rated on scales (1-7 points), whether they considered the diary comprehensible, supportive, simple, safe, as expected, and clear. Higher scores represented higher degrees of satisfaction.
Discussion
Primary brain tumors often cause neurologic symptoms including focal and generalized seizures. In the literature, the prevalence of pre-treatment seizures was reported to range from 29 to 67% in patients with grade III gliomas and from 9 to 45% in patients with GBM (4-10). In our prior study of patients irradiated for malignant gliomas, the prevalence of pre-radiotherapy seizures was 48.8% and 21.5% in patients with grade III or grade IV gliomas, respectively (4). Although a considerable number of patients assigned to radiotherapy or chemoradiation of gliomas experience seizures, very little is known about the development of seizures during a radiotherapy course. Since radiotherapy of gliomas leads to an acute inflammatory reaction in the brain resulting in edema and increased intracranial pressure, it is likely that it triggers the occurrence of seizures or aggravates pre-existing symptoms (11, 12). In a series of 11 patients who received post-operative radiotherapy for residual pituitary tumors and developed radiation-induced brain disorders, generalized seizures were found in four of these patients (11). Moreover, in a review article, seizures were identified as presenting symptoms of acute radiation-induced encephalopathy (12).
When designing the present SURF-ROGG trial, it was hypothesized that at least 30% of the patients receiving radiotherapy or concurrent chemoradiation for high-grade gliomas would experience progression of seizure activity during the 6 to 7 weeks course of this treatment. Since according to sample size calculations, 32 evaluable patients were required, a progression rate of at least 30% would mean that 10 patients would experience increased seizure activity during their course of radiotherapy. However, according to the results of the SURF-ROGG trial, the progression rate was 45% and, therefore, higher than expected. When comparing the mean seizure frequencies during and following radiotherapy to baseline, a significant difference was found for “weeks 4-6/7 during radiotherapy” and a trend was observed for “weeks 1-3 during radiotherapy”. These results suggest that an increase in seizure activity can occur at any time during radiotherapy but appeared to become more likely during the second half of the course.
Eight patients had an increase in focal seizures that was identified only by the seizure diary, which, therefore, can be considered very helpful for this purpose. In contrast, only 2% of all EEGs performed at various time points showed activity considered typical for epilepsy. Therefore, the diagnostic benefit of EEGs during radiotherapy for gliomas appeared limited. However, the value of the seizure diary had limitations when used in this group of patients. This applied particularly to the patients’ satisfaction with its use. Almost 40% of the patients gave a mean satisfaction score of <4.0 points on a scale of 1-7 points. The lowest mean scores were given for feeling safe with the seizure diary followed by clarity and supportive value. These findings suggest that, although a seizure diary kept by the patients can be helpful for identifying increased seizure activity, the patients may still require additional support by medical staff members for its optimal use.
In summary, radiotherapy of high-grade gliomas can increase seizure activity during the course of treatment. The rate of progression of seizure activity was higher than expected. Thus, patients need close monitoring to initiate or adjust anti-epileptic medication. A seizure diary can be helpful for identifying increased seizure activity in this patient group. However, patients may require support by medical staff members for optimal use of the diary.
Acknowledgements
As part of the project NorDigHealth, this study was funded by the European Regional Development Fund through the Interreg Deutschland-Danmark program (Interreg Secretariat, Kruså, Denmark).
Footnotes
Authors’ Contributions
D.R., J.W., P.T., D.O., S.E.S., S.T. and T.W.K. participated in the design of the study. Data were collected by D.R., J.W. and P.T., and analyzed by a professional statistician. D.R. and S.E.S. drafted the article, which was read and approved by all Authors.
Conflicts of Interest
On behalf of all Authors, the corresponding Author states that there are no conflicts of interest related to this study.
- Received May 21, 2022.
- Revision received June 8, 2022.
- Accepted June 9, 2022.
- Copyright © 2022, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).