

Abstract
Background: Cancer of the Meckel’s diverticulum (MD) is extremely rare. It is often advanced at the time of operation and the prognosis is poor. An effective treatment for this cancer has not yet been developed and there is no MD-carcinoma mouse model. Materials and Methods: MD carcinoma was established as a patient-derived xenograft (PDX) in 5-week-old male nude mice by subcutaneous transplantation of surgical specimens together with surrounding normal tissue. Hematoxylin and eosin (H&E) staining was performed on paraffin-embedded tissue sections of the original tumor resected from patients and transplanted tumors grown in nude mice. Results: Three of five mice implanted with MD tumor fragments grew. MD-carcinoma histopathology, observed with H&E-stained tissue sections of the tumors grown in the mice and tumor from the original patient, was concordant. Both showed the luminal structures characteristic of MD carcinoma, and the lumens were filled with serous fluid. Conclusion: The first PDX mouse model of MD carcinoma has been established. The PDX model maintained MD-carcinoma histology of the tumor in the patient. The MD carcinoma mouse model will enable basic research on MD carcinoma, as well as the testing of novel therapeutic agents.
- Meckel’s diverticulum carcinoma
- mouse model
- PDX
- patient-derived xenograft
- nude mouse
Meckel’s diverticulum (MD) is a remnant of the yolk sac in the embryo. It is located 0.5 to 1 cm from the ileum to the oral side and is found as a protrusion on the lateral side of the intestinal membrane (1-3). The incidence of MD cancer is very low, i.e., 0.5%-3.2% of patients with Meckel’s diverticulitis (4). According to Weinstein, of the 106 MD tumor lesions analyzed, 26 were benign and 80 were malignant, the latter consisting of 35 sarcomas, 29 carcinoids, and 16 carcinomas (4). Early diagnosis of MD carcinoma is difficult because of its anatomical location, and therefore the tumor is often found in an advanced stage (5). The only treatment is surgery, but in many cases, it is not curative. Chemotherapy is considered to be necessary, but due to limited data, the clinical features are often unclear, and first-line treatment has not yet been defined (6).
Since cancers originating from MD occur very infrequently and are poorly documented, a patient-derived xenograft (PDX) mouse model of MD carcinoma has not yet been established. In a recent study, we established an improved tumor-establishment method in nude mice: PDX mouse models were established using Hozumi’s tumor-transplantation method (7), in which the tumor and surrounding normal non-cancerous tissue from surgical specimens are co-transplanted subcutaneously. We used Hozumi’s method to establish the first PDX model of MD-carcinoma.
Materials and Methods
Mice. To establish an MD-carcinoma PDX mouse model, athymic (nu/nu) nude mice (AntiCancer, Inc., San Diego, CA, USA) were used under an AntiCancer, Inc. Institutional Animal Care and Use Committee (IACUC) protocol that was specifically approved for the present study, which followed the principles and procedures outlined in the National Institutes of Health Guide for the Care and Use of Animals, Assurance No. A3873-1.
Patient-derived tumor. A surgical specimen of MD carcinoma was collected at Ikeda Hospital, Shizuoka, Japan with written informed patient consent.
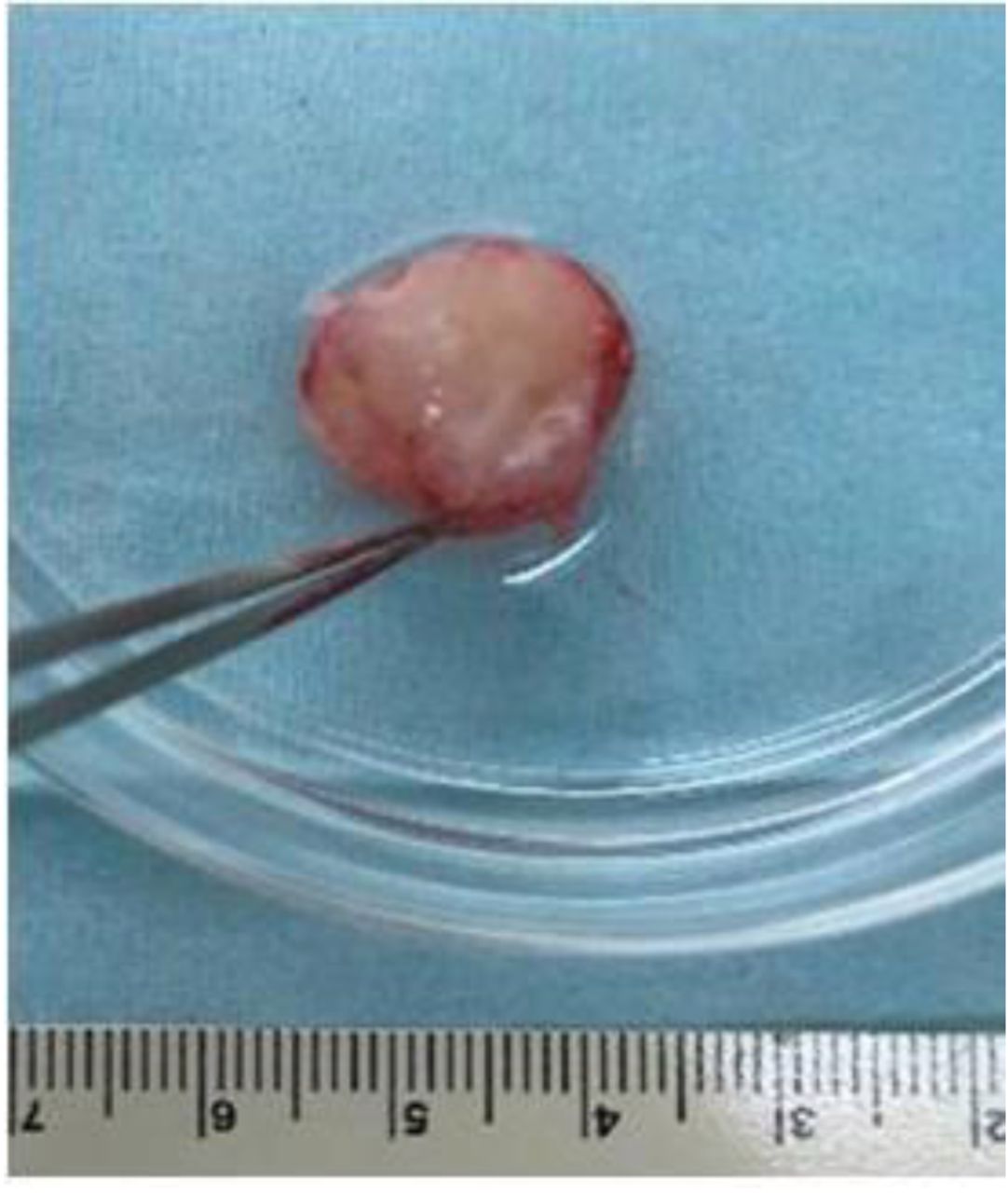
Establishment of an MD carcinoma PDX nude mouse model. The surgical specimen, comprising tumor and surrounding normal tissues, was prepared for implantation by mincing with a surgical scissors into approximately 50 mm3 pieces (Figure 1A and B). Mice were coimplanted with tumor and surrounding normal tissue using the method of Hozumi (7). Mice were anesthetized with a ketamine mixture. A 1-cm skin incision was made in the middle of the back of the nude mice. The skin was detached from the dermis with surgical scissors and pockets were created in the bilateral lateral abdomen. Fragments of MD carcinoma were inserted into the pocket along with surrounding normal tissue. The wound was closed with 5-0 PDS-II sutures (Figure 2). The implanted tumor was observed for 6 months. The tumor volume was calculated as short axis × short axis × long axis/2. All mice were sacrificed at 6 months after implantation and tumors were harvested for histological evaluation.

A surgical specimen of Meckel’s diverticulum (MD) carcinoma and surrounding normal tissue. (A) MD carcinoma tissue and surrounding normal tissue. (B) Fragmentation of MD carcinoma tissue and surrounding normal tissue.

Meckel’s diverticulum (MD) carcinoma patient-derived xenograft (PDX) mouse model immediately after co-transplantation of tumor and surrounding normal tissue. Black arrows indicate tumors under the skin of the bilateral lateral abdomen.
Histopathology. Tumor tissues were cut into 7-mm fragments and fixed in 10% formalin for 48 hours at room temperature. To remove formalin from the tissue, it was rinsed with 70% alcohol. The treatment schedule consisted of dehydration with ascending grade of alcohols (70%, 80%, 90% and 100% alcohol with two exchanges, 1 h each) and with two changes of xylene (1 h each). Tissue samples were then treated with three exchanges of graded paraffin wax for 1 h each. After embedding, using a sliding microtome, paraffin blocks were sectioned at a thickness of 4 μm. Warm water at 37°C was used for extension of the sections. Tissue sections were mounted on glass slides and dried overnight in a slide warmer at 60°C. Specimens were stained according to standard hematoxylin-eosin protocols for histopathological evaluation (8).
Results
Establishment of an MD-carcinoma PDX mouse model. Five mice were implanted with patient-derived MD carcinoma subcutaneously in the bilateral abdomen along with surrounding normal tissue (Table I). Tumors grew in three of the five mice implanted with MD carcinoma; one died the day after tumor implantation, and another died one week after tumor implantation. The cause of death was unknown. Six months after transplantation, the three mice with growing tumor were sacrificed for specimen collection. Grossly, the tumor was confined to the subcutaneous region and there were no organ metastases observed (Figure 3A and B). The smooth surface of the harvested tumor was milky white and similar to the tumor obtained from the patient (Figure 4).
MD carcinoma tumor volume and mouse weight.

A nude mouse six months after MD tumor transplantation. (A) The tumor on the left side of the abdomen grew to approximately 10 mm after 6 months. (B) The tumor was confined to the subcutaneous region, and there was no invasive metastasis observed in other organs.

The circumferential surface of the mouse-grown tumor was milky white, similar to the original patient tumor.
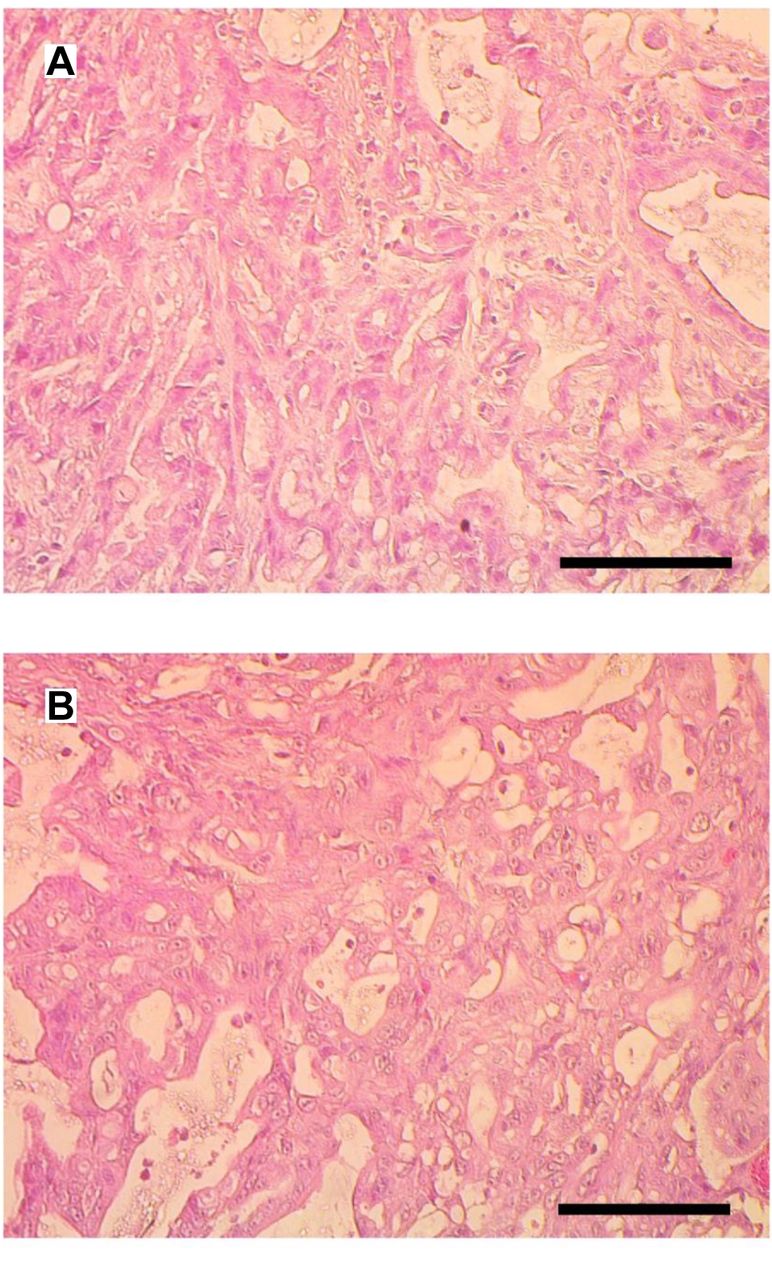
Histological comparison of MD carcinoma in the patient and the PDX nude-mouse model established from the patient. H&E staining showed that the carcinoma in the PDX mouse model consisted of dense cancer cells with a luminal structure characteristic of adenocarcinoma, and the lumen was filled with serous fluid, concordant with the original patient tumor (Figure 5A and B).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Representative photomicrographs of H & E-stained Meckel’s diverticulum (MD) carcinoma. (A) Patient carcinoma. (B) Patient- derived xenograft (PDX). Scale bar: 50 μm.
Discussion
MD cancers go undetected because they develop in the MD that resides in the small intestine. Therefore, by the time the MD cancer is diagnosed, it is often at an advanced stage (5). If the cancer is found to be advanced, chemotherapy is required, but due to the small number of cases, little research has been done to develop first-line chemotherapy, in part due to the lack of an MD-carcinoma mouse model. In the present study, we have succeeded in establishing an MD-carcinoma PDX mouse model. In order to establish the MD-carcinoma PDX mouse model from a patient-derived tumor, Hozumi’s method of co-transplanting tumor tissue and surrounding normal tissue was used (7). Previously, we were able to successfully establish the first PDX mouse model of osteosarcoma of the mammary gland using Hozumi’s method (9). The inclusion of normal tissue around the tumor tissue seems to be effective in increasing the frequency of tumor establishment in nude mice (7).
In the present study, it took approximately six months for the tumor to grow from 50 mm3 to 1,000-3,000 mm3. Generally, tumors in PDX mouse models grow for 2 to 8 months (10).
The present study has successfully established the first PDX mouse model of the extremely-rare MD carcinoma. Establishment of MD carcinoma in nude mice effectively immortalizes the tumor and allows it to be cryopreserved for future transplantation into nude or other immunocompromised mice. The successful establishment of the first PDX mouse model of MD carcinoma can enhance scientific research on the MD carcinoma. At present, no first-line drug for MD carcinoma has been identified. Drug-sensitivity screening will be conducted in future experiments on the MD-carcinoma PDX model established in the present study. An orthotopic mouse model of MD carcinoma will also be established in future studies (11).
Footnotes
Authors’ Contributions
N.M. conceived the study, N.M. and C.S. performed the experiments and Y.Y., N.F.W., C.H., Y.K., Y.A., M.B., J.M. and R.M.H. provided scientific advice. N.M. wrote the paper and R.M.H. revised the paper.
Conflicts of Interest
The Authors declare that they have no conflicts of interest.
- Received March 31, 2022.
- Revision received May 3, 2022.
- Accepted May 20, 2022.
- Copyright © 2022, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved
This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY-NC-ND) 4.0 international license (https://creativecommons.org/licenses/by-nc-nd/4.0).