

Abstract
Aim: To evaluate the efficacy of chemoembolization versus radioembolization in reducing lung shunt fraction (LSF) in patients with hepatocellular carcinoma (HCC). Patients and Methods: In this retrospective study, from March 2012 to January 2021, 457 patients with HCC underwent planning angiography and 99mTc-macroaggregated albumin imaging for possible yttrium-90 radioembolization. Ten patients underwent radioembolization, and seven patients underwent conventional chemoembolization for LSF reduction, and a second 99mTc-macroaggregated albumin imaging was obtained approximately 1 month later. LSF under both procedures was compared with the Mann-Whitney U-test and the Wilcoxon signed-rank test. Results: In the radioembolization group, the mean first and second LSF were 13.0±6.9% and 20.9±9.6%, respectively (p=0.059); after radioembolization, LSF was lower in three patients but higher in seven patients. In the chemoembolization group, the mean first and second LSF were 26.1±17.3% and 8.7±5.5%, respectively (p=0.018); after chemoembolization, LSF was reduced in all seven patients. Conclusion: Chemoembolization appears to be more effective in reducing LSF within 1 month compared with radioembolization.
- Hepatocellular carcinoma
- radioembolization
- lung shunt reduction.
Radioembolization with yttrium-90 microspheres is a potent form of transarterial therapy for patients with hepatocellular carcinoma (HCC), with minimal post-embolization syndrome (1). Boosted radioembolization (with a mean absorbed dose to the target tissue >150 Gy) has been found to prolong the survival of patients with good liver function (2). The recent LEGACY study demonstrated excellent tumor response in patients with solitary HCC (≤8 cm), with a median absorbed dose to the target tissue of 410 Gy (3). Unlike chemoembolization, however, radioembolization cannot be performed in patients with a high lung shunt fraction (LSF) because of possible radiation-induced pneumonitis (4). Using glass microspheres, a total lung dose of 30 Gy per treatment, or 50 Gy in a lifetime, is considered the upper limit (4). The lung dose depends on the absolute LSF as well as the target tissue volume and desired mean absorbed dose to the target tissue. For example, when LSF is 10% and the target volume is 1,800 ml, boosted radioembolization is not an option because the lung dose would be over 30 Gy with a mean absorbed dose to the target tissue of 150 Gy.
When the estimated lung dose is over 30 Gy, radioembolization may be tried after an LSF reduction procedure; alternatively, another treatment modality (chemoembolization, surgical resection, or systemic therapy) may be an option. Several methods can reduce LSF, including bland embolization, chemoembolization, low-dose radioembolization, hepatic vein occlusion with a balloon catheter, and systemic chemotherapy (5-11). At the Authors’ Institute, chemoembolization or radioembolization is commonly recommended for LSF reduction in patients with a high estimated lung dose. The purpose of this study was to evaluate the efficacy of chemoembolization versus radioembolization for LSF reduction in patients with HCC.
Patients and Methods
Patients. This single-center, retrospective study was approved by the Institutional Review Board (number 2101-165-1191), and informed consent was waived. From March 2012 to January 2021, 457 patients with HCC underwent planning angiography and 99mTc-macroaggregated albumin (MAA) imaging for possible yttrium-90 radioembolization. Three hundred and fifty-one patients underwent radioembolization, and 106 patients were managed with chemoembolization (n=76) or other treatment (n=30) (Figure 1).
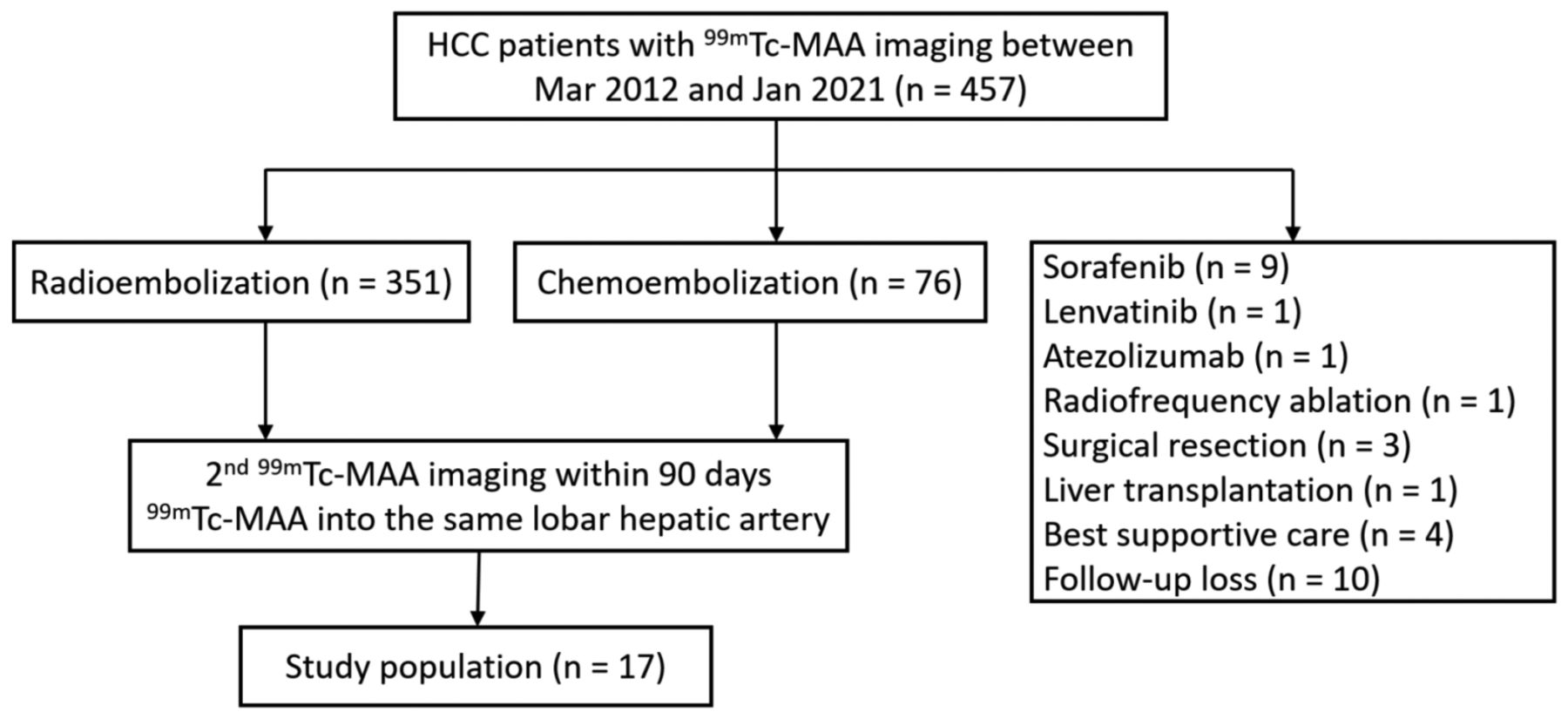
Flowchart of the study population. MAA: Macroaggregated albumin.
The inclusion criteria were as follows: i) Chemoembolization or radioembolization performed for LSF reduction; ii) a second 99mTc-MAA imaging performed within 90 days of the first treatment for the primary target tumor; and iii) the patient received a 99mTc-MAA injection into the same lobar hepatic artery for the first and second 99mTc-MAA imaging. Exclusion criteria were i) Previous chemoembolization, ablation therapy, or systemic therapy for the primary target tumor; and ii) repeated 99mTc-MAA imaging for bi-lobar sequential radioembolization (i.e., 99mTc-MAA injection into the contralateral lobar hepatic artery). Among the 457 patients, 10 underwent radioembolization, and seven patients underwent conventional chemoembolization for LSF reduction, after which a second 99mTc-MAA imaging was obtained (Figure 1).
Seventeen male patients (mean age: 59.9±13.4 years; age range: 37-83 years) therefore comprised the study population. The demographic characteristics of the patients are summarized in Table I. The mean primary tumor size was 12.6±2.4 cm (range=7.4-18.6 cm). Nine patients (53%) had vascular invasion (portal vein/hepatic vein).
Clinical and radiological findings in 17 patients (all male) with hepatocellular carcinoma.
Yttrium-90 radioembolization. The detailed protocol for radioembolization has been described in previous studies (12-15). Two interventional radiologists (H.C.K., with 15 years of experience in interventional oncology and M.L. with 10 years of experience) performed all radioembolization procedures. In the early study period (March 2012 to June 2016), radioembolization was performed with standard dosimetry of TheraSphere or SIR-Spheres as recommended by the manufacturers. In the late study period (July 2016 to January 2021), boosted radioembolization (240-360 Gy mean absorbed dose to the target tissue) was used when applicable (i.e., when the estimated lung dose was less than 30 Gy, and liver function was preserved). Low-dose, regular, and boosted radioembolization were defined as <80 Gy, 80-150 Gy, and >150 Gy mean absorbed dose to the target tissue, respectively.
Chemoembolization. The detailed protocol for chemoembolization has been described in previous studies (16-18). Under this protocol, an iodized oil emulsion (a mixture of doxorubicin and iodized oil) is injected until the peritumoral portal vein is filled with iodized oil, followed by embolization with gelatin sponge particles. In large HCCs (>7 cm), an alternative injection of iodized oil emulsion and polyvinyl alcohol particles (45-150 μm) is given through the main tumor-feeding branches until near-stasis of the target vessel is achieved, then gelatin sponge particles are added to achieve complete stasis. In all patients, the maximum doses of iodized oil and doxorubicin were 10 ml and 50 mg, respectively. In patients with vascular invasion, an additional infusion of cisplatin (50-70 mg) was performed after conventional chemoembolization (17, 18).
Lung shunt reduction. Between March 2012 and December 2014, only resin microspheres were available at the Authors’ Institute. When LSF was greater than 20%, chemoembolization was recommended as a method of LSF reduction. A second planning angiography and a second 99mTc-MAA imaging after chemoembolization were performed for only one patient (Figure 2A).

Flowchart of the study population according to the study period. A: Study population between March 2012 and December 2014. B: Study population between January 2015 and June 2016. C: Study population between July 2016 and January 2021. MAA: Macroaggregated albumin.
Between January 2015 and June 2016, only glass microspheres were available at the Authors’ Institute. When the mean absorbed dose to the target tissue was less than 100 Gy, chemoembolization was recommended as a method of LSF reduction. However, a second planning angiography was not performed for any of the patients treated during this time (Figure 2B).
Between July 2016 and January 2021, both glass and resin microspheres were available, and boosted radioembolization (with a mean absorbed dose to the target tissue dose >240 Gy) was primarily performed. When the mean absorbed dose to the target tissue dose was less than 240 Gy, patients and their referring physicians were given three options: Switching to another treatment modality, undergoing boosted radioembolization after chemoembolization, or undergoing boosted radioembolization after first radioembolization. Sixteen patients underwent a second planning angiography and a second 99mTc-MAA imaging after chemoembolization (n=6) or after first radioembolization (n=10) (Figure 2C). The second planning angiography and second 99mTc-MAA imaging were performed approximately 1 month after the LSF procedure.
Patients chose their LSF reduction procedure (chemoembolization or radioembolization) after being informed about the benefits and risks of each. The performance of a second planning angiography and a second 99mTc-MAA imaging was determined in consultation with the referring physician and interventional radiologists.
Analysis. Radiological and clinical data were retrospectively collected, and tumor response was evaluated with modified response evaluation criteria in solid tumors (mRECIST) (19). The Mann-Whitney U-test was used to compare LSF between the two groups. The first and second LSF in each group was compared using the Wilcoxon signed-rank test. A p-value of less than 0.05 was considered statistically significant. All statistical analyses were performed with SPSS version 25.0 software (IBM, Armonk, NY, USA).
Results
In the radioembolization group, the mean first and second LSF were 13.0±6.9% and 20.9±9.6%, respectively (p=0.059) (Table II). Only one patient underwent low-dose radioembolization (mean absorbed dose of 47 Gy), while nine patients underwent regular (n=6) or boosted (n=3) radioembolization. After radioembolization, LSF was lower in three patients but higher in the remaining seven. All 10 patients showed stable disease at the time of the second planning angiography (Figure 3). Three patients underwent a second session of radioembolization, while seven patients did not.
Statistical analysis of lung shunt fraction (LSF).

A 68-year-old man (patient number 9) with hepatocellular carcinoma. A: Computed tomography showing ill-defined tumor (arrowheads) in the right lobe of the liver and a tumor thrombus in the right portal vein (arrow). B: Common hepatic arteriogram showing ill-defined hypervascular tumor blush in the right lobe of the liver. 99mTc-Macroaggregated albumin was injected into the right hepatic artery (arrow), and the lung shunt fraction was 7.21%. Radioembolization was performed via the right hepatic artery; radiation activity at administration was 7.89 GBq, and the estimated lung dose was 27.87 Gy. C: Computed tomography 3 weeks after radioembolization showing stable disease of ill-defined tumor (arrowheads) and portal vein thrombus (arrow). A second macroaggregated albumin imaging was performed 4 weeks after radioembolization, and lung shunt fraction increased to 18.98%.
In the chemoembolization group, the mean first and second LSF were 26.1±17.3% and 8.7±5.5%, respectively (p=0.018) (Table II). LSF after chemoembolization was reduced in all seven patients. All seven patients showed a partial response at the time of the second planning angiography (two underwent two sessions of chemoembolization) (Figure 4). Five patients underwent subsequent radioembolization. One patient was not able to undergo radioembolization due to severe arterioportal shunt caused by portal vein tumor thrombosis, and another patient underwent surgical resection instead of radioembolization based on the referring physician’s recommendation.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
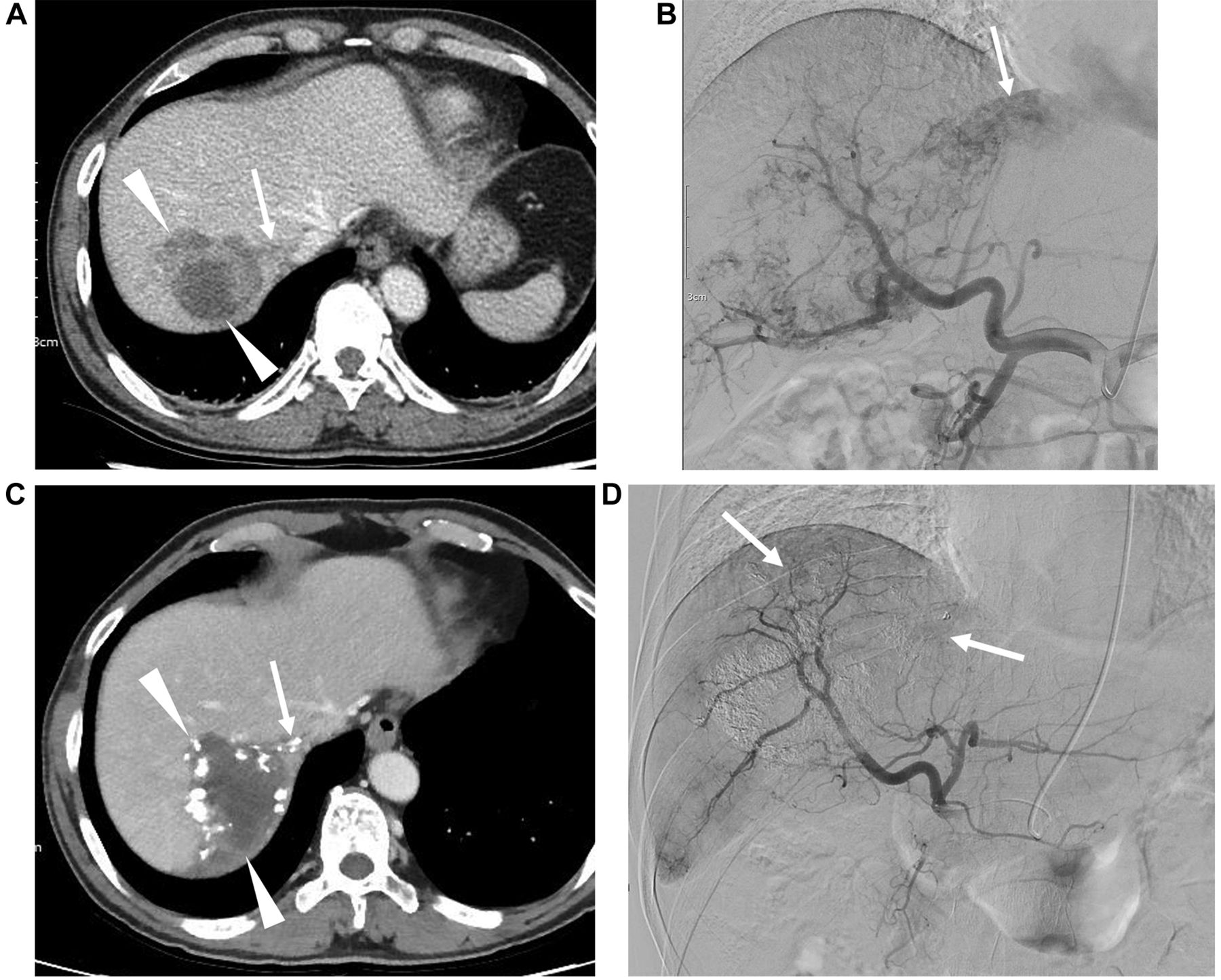
A 60-year-old man (patient number 17) with hepatocellular carcinoma. A: Computed tomography scan showing a large mass (arrowheads) in the right lobe of the liver and a tumor thrombus in the right hepatic vein (arrow). B: Celiac angiogram showing hypervascular tumor blush in the right lobe of the liver and hepatic venous shunting through the right hepatic vein (arrow). 99mTc-Macroaggregated albumin was injected into the right hepatic artery, and the lung shunt fraction was 63.3%. Chemoembolization was performed via the right hepatic artery, caudate artery, and right inferior phrenic artery with alternative injection of iodized oil emulsion (10 ml of Lipiodol and 40 mg of doxorubicin) and gelatin sponge particles. Additional infusion of 50 mg of cisplatin was performed via the right hepatic artery. C: Computed tomography 3 weeks after chemoembolization showing abundant tumor necrosis (arrowheads) and iodized oil accumulation in the right hepatic vein thrombus (arrow). D: A second macroaggregated albumin imaging was performed 5 weeks after chemoembolization. A hepatic angiogram showing a small multifocal residual tumor blush (arrows), and the lung shunt fraction decreased to 7.65%.
Whereas the first LSF of the chemoembolization group was higher than that of the radioembolization group (p=0.01), the second LSF was lower (p=0.005) (Table II).
Discussion
Chemoembolization and bland embolization have been reported to be effective in reducing LSF (6, 8-10), and the results of this study are compatible with those of previous studies. However, LSF tended to increase after radioembolization in this study. Low-dose radioembolization (an estimated lung dose less than 30 Gy) was mentioned in one review article (11) but we found no further case reports or original articles.
Since radioactive microspheres and MAA are a little larger than the diameter of the liver sinusoid, LSF through normal liver would be negligible. In a recent study with a large study population (20), LSF was clinically negligible in patients with United Network for Organ Sharing T1/T2 HCC, and 99mTc-MAA imaging can be eliminated when segmental injections are planned. It has been reported that a high LSF is associated with a large tumor burden and vascular invasion (21, 22). Thus, we speculated that radioactive microspheres and MAA would be able to pass through HCCs with abnormally dilated vessels, and a reduction of tumor mass might be a direct way of reducing LSF in patients with high LSF.
Chemoembolization and bland embolization exert their antitumor effect by immediate ischemic injury to the tumor, and partial response may be easily observed on imaging 1 month later. Thus, chemoembolization was effective in reducing LSF in this study. On the other hand, radioembolization does not result in ischemic injury, and it may take several months for radioembolization to show a radiological response (23). In this study, all the patients in the radioembolization group showed stable disease at 1-month imaging. Thus, radioembolization was not effective in reducing LSF.
After external radiation therapy, the irradiated liver tissue shows variable enhancement changes that are explained by radiation-induced veno-occlusive disease or fibrotic change (24). Histopathological changes after radioembolization have not yet been described in detail in the literature (25). Radioembolization may cause distortion of the hepatic microvascular structure, which may be the reason why LSF increased in seven patients in this study.
This study has some limitations. Firstly, the study population was relatively small, and further studies are required to draw solid conclusions. Secondly, in the radioembolization group, nine patients received regular or boosted radioembolization rather than low-dose radioembolization. In addition, most patients in the radioembolization group had mildly elevated LSF. Thus, there is a possibility that low-dose radioembolization may be effective in reducing LSF in patients with highly elevated LSF. Thirdly, because the first LSF in the chemoembolization group was higher than that of the radioembolization group, it may be that LSF reduction was more easily achieved in the chemoembolization group. Fourthly, the second LSF was measured approximately 1 month after radioembolization in this study. It is not known how long it takes to reduce LSF with radioembolization. If LSF had been measured 3 months after radioembolization, it is possible that it would have been shown to have decreased further. Finally, baseline characteristics such as tumor type, vascular invasion and first LSF were a little different between the two groups. Because of the small study population, the baseline characteristics were not compared with statistical analysis.
In conclusion, chemoembolization appears to be more effective in reducing LSF within 1 month compared with radioembolization.
Footnotes
Authors’ Contributions
Guarantor of integrity of the entire study: Hyo-Cheol Kim. Study concepts and design: Hyo-Cheol Kim. Literature research: Hyo-Cheol Kim, Myungsu Lee and Jin Chul Paeng. Clinical studies: Hyo-Cheol Kim, Jin Woo Choi, Myungsu Lee, Yoon Jun Kim, Jin Chul Paeng and Jin Wook Chung. Data analysis: Hyo-Cheol Kim, Jin Woo Choi, Myungsu Lee and Jin Chul Paeng. Stastitical analysis: Hyo-Cheol Kim, Myungsu Lee and Yoon Jun Kim. Article preparation: Hyo-Cheol Kim. Article editing: Jin Woo Choi, Myungsu Lee, Yoon Jun Kim, Jin Chul Paeng and Jin Wook Chung.
This article is freely accessible online.
Conflicts of Interest
The Authors have no conflicts of interest to disclose in relation to this study.
- Received April 20, 2021.
- Revision received May 9, 2021.
- Accepted May 17, 2021.
- Copyright © 2021 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved