

Abstract
Background/Aim: To date, multiple different surgical techniques have been established for hallux valgus surgery, with each technique having its unique advantages and limitations. The open distal chevron osteotomy is widely accepted, but increasing patient demands have led several minimally invasive (MIS) techniques to be described in recent years. The aim of this study was to compare outcomes after minimally invasive (MIS) distal chevron osteotomy and the minimally invasive Reverdin-Isham method. Patients and Methods: We assessed clinical and radiographic outcomes after MIS chevron osteotomy in 57 feet of 49 consecutive patients with a mean follow-up of 58.9 (range=39.0-85.4) months. Outcomes after MIS Reverdin-Isham osteotomy were analyzed by means of a systematic literature review with a minimum follow-up of 6 months. Results: Radiographic outcomes were significantly better in the MIS chevron cohort for intermetatarsal angle (p<0.001), hallux valgus angle and distal metacarpal articular angle (p<0.05). Concerning clinical outcomes, both methods provided comparable improvement. Conclusion: MIS distal chevron osteotomy in mild to moderate hallux valgus deformity correction results in superior radiographic outcomes compared to the MIS Reverdin-Isham osteotomy. Sufficient correction of IMA cannot be achieved with the MIS Reverdin-Isham osteotomy.
- Chevron
- Reverdin-Isham osteotomy
- Hallux valgus
- minimally invasive surgery
- review
To date, multiple different surgical techniques have been established for hallux valgus surgery, with each having its unique advantages and limitations. The open distal chevron osteotomy is widely accepted as a method for correcting mild to moderate hallux valgus deformities (1) with numerous studies presenting good radiological (2, 3) and clinical outcomes (4, 5). Scarring and decreased range of motion of the greater toe joint after open surgery (6) as well as increasing patient demands have led several minimally invasive (MIS) techniques to be described in recent years (7-10). The corrective power and its stability, as well as the clinical outcome of different MIS techniques are discussed controversially to date (11-13). Recently, two prospective randomized studies comparing the MIS and the open distal chevron osteotomy were published with comparable clinical and radiographic outcomes after short- and long-term follow-up (14, 15). Whereas most studies presented good clinical and radiological results (9, 14-16), the group of Crespo-Romero found insufficient radiographic hallux valgus angle (HVA) correction (17). Nevertheless, in various systematic review studies of MIS hallux valgus correction a clear recommendation could not be made although early results were encouraging (18-22). The uncertainty of outcome following minimally invasive hallux surgery might be a consequence of analyzing different surgical techniques without methodological differentiation between these techniques. Thus, it might be beneficial to evaluate outcomes after MIS surgery with regard to the applied technique.
Given the above-mentioned lack of evidence it was the aim of the study to compare the results of two different specific MIS techniques for hallux valgus correction. Since MIS distal chevron has been shown to provide comparable results to the open technique for correction of mild to moderate hallux valgus deformities (14, 15), we analyzed this technique in comparison to the Reverdin-Isham procedure, which is known as the technique that made MIS surgery popular (19). It was hypothesized that the two techniques would show significant differences with regard to radiological outcome (Hypothesis 1) and clinical outcome (Hypothesis 2).
Patients and Methods
The study was conducted in accordance with the ethical standards outlined in the 1964 World Medical Association Declaration of Helsinki and its later amendments following the Consolidated Standards of Reporting Trials (CONSORT) guidelines. The local ethics committee approved the present study (1062/2018). The study has been listed on ClinicalTrials.gov (identifier: NCT04288297). The review was designed according to the recommendations in the literature (23) for systematic reviews of the literature and meta-analysis (24).
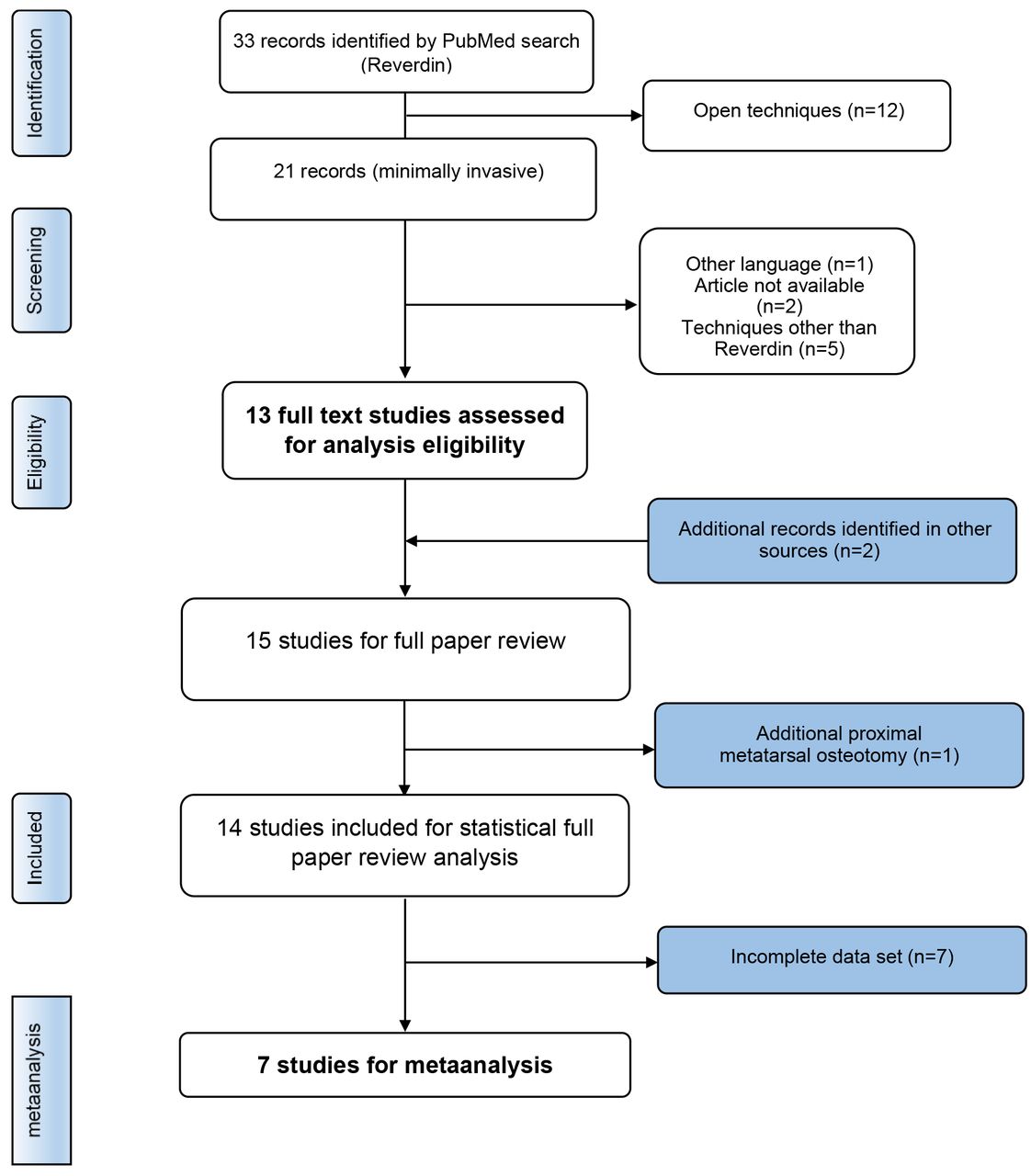
Search strategy. In October 2019, a bibliographic search was conducted in the PubMed/Medline and EMBASE databases. The search terms used were “hallux valgus” and “Reverdin Isham” or “minimally invasive” or “percutaneous” or “distal osteotomy” or “oblique osteotomy”. Exclusively articles in English or Spanish, without limitation of year of publication, assessing the described surgical method with a minimum follow-up of 6 months and presenting results in terms of clinical or radiological data were included. Primary selection was made after reading the title and the published abstracts. The selected articles were read and checked for eligibility by two authors independently (GK and ML). Our search strategy produced 33 studies for “hallux valgus” and “Reverdin Isham”. In combination with “percutaneous” or “minimally invasive” 21 studies remained. After exclusion of articles published not in English or Spanish language, and of studies presenting data on patients treated not with distal Reverdin-Isham osteotomies 15 studies remained. Two selected abstracts found in Pubmed were not available as full papers (25, 26). Two other studies were identified in the reference list of another included study (27, 28). After double-checking for duplicates, 15 studies were available for full paper review (7, 17, 25, 28-39) and all were reviewed. One study had to be excluded, because a proximal metatarsal osteotomy was performed in addition to the Reverdin osteotomy (39). Seven of these studies could not be used for statistical meta-analysis because the data set was incomplete (no defined follow-up time, missing radiological and/or clinical data). The selection process and reasons for exclusion are shown in the flow diagram in Figure 1. Overall standardized mean correction of specific radiographic angles was performed using a forest-plot analysis. For this analysis another study had to be excluded, because an additional metatarsal osteotomy had been performed in 27% of the study cohort (17). One study analyzed outcomes after unilateral and bilateral Reverdin-Isham osteotomy separately (29). Therefore, these two groups were regarded as two original studies in our meta-analysis.

Flow diagram of studies included and excluded in the present analysis.
The results after MIS Reverdin-Isham osteotomy presented in the published literature were compared with a prospective series of 57 feet in 49 patients with mild to moderate hallux valgus deformity treated with MIS distal chevron osteotomy performed at our department between October 2012 and November 2016. All patients were invited to participate and gave written informed consent prior to inclusion. Exclusion criteria were: 1) age <18 years, 2) previous surgical hallux valgus correction on the same foot, 3) tarsometatarsal joint instability of the first ray, defined as painful motion in this joint, 4) symptomatic osteoarthritis of the first metatarsophalangeal joint, 5) preoperative hallux valgus angle (HVA) of less than 20 degrees (40, 41), 6) an intermetatarsal angle (IMA) of less than 10 degrees (42) with regard to the definition of hallux valgus deformity or IMA surmounting 15 degrees to exclude patients with more severe deformities.
Outcome parameters. For all examined patients clinical outcome in terms of 1) range of motion (ROM) of the first metatarsophalangeal joint, categorized in three groups (group 1: ROM <30°; group 2: ROM 31°-75°; group 3: ROM >75°), 2) a pain score (visual analogue scale – VAS 0-10), 3) and the AOFAS (American Orthopaedic Foot & Ankle Society) Forefoot Scale was assessed as it has been described previously (14, 15). Radiographic outcome was measured on weightbearing radiographs in digital manner using the Icoview software (syngo.share, ITH icoserve healthcare GmbH, Siemens, Innsbruck, Austria) in the form of a single researcher single measurement approach (MB). All the evaluated parameters were the following and have been previously described (14, 15): lateralization of the sesamoids (4-fold, 7-fold), the hallux valgus angle (HVA), the intermetatarsal angle (IMA), the distal metatarsal articular angle (DMAA), the proximal to distal phalangeal articular angle (PDPAA), and the joint congruity angle (JC), shown by tangential lines running along the edges of the joint of the metatarsal head and the base of the phalangeal bone. Additionally, osteoarthritis was assessed in our chevron cohort with the 4-fold Kellgren-Lawrence grading scale (43). Outcome was evaluated preoperatively, after six weeks, 12 weeks and nine months postoperatively and at final follow-up.
Surgical technique. All surgeries were performed by one single consultant foot and ankle surgeon (GK). The surgical technique of this V-shaped osteotomy has already been described in the literature (14). MIS distal chevron osteotomy was performed percutaneously through a dorsomedial incision of 3-5 mm. With a sliding osteotomy of the metatarsal head the correction the IMA is intended. In 45 feet a phalangeal Akin osteotomy was added. The MIS Reverdin-Isham osteotomy technique has been well described in the literature as well (32). The concept of this osteotomy is a medial based closing wedge osteotomy of the metatarsal head without addressing the IMA.
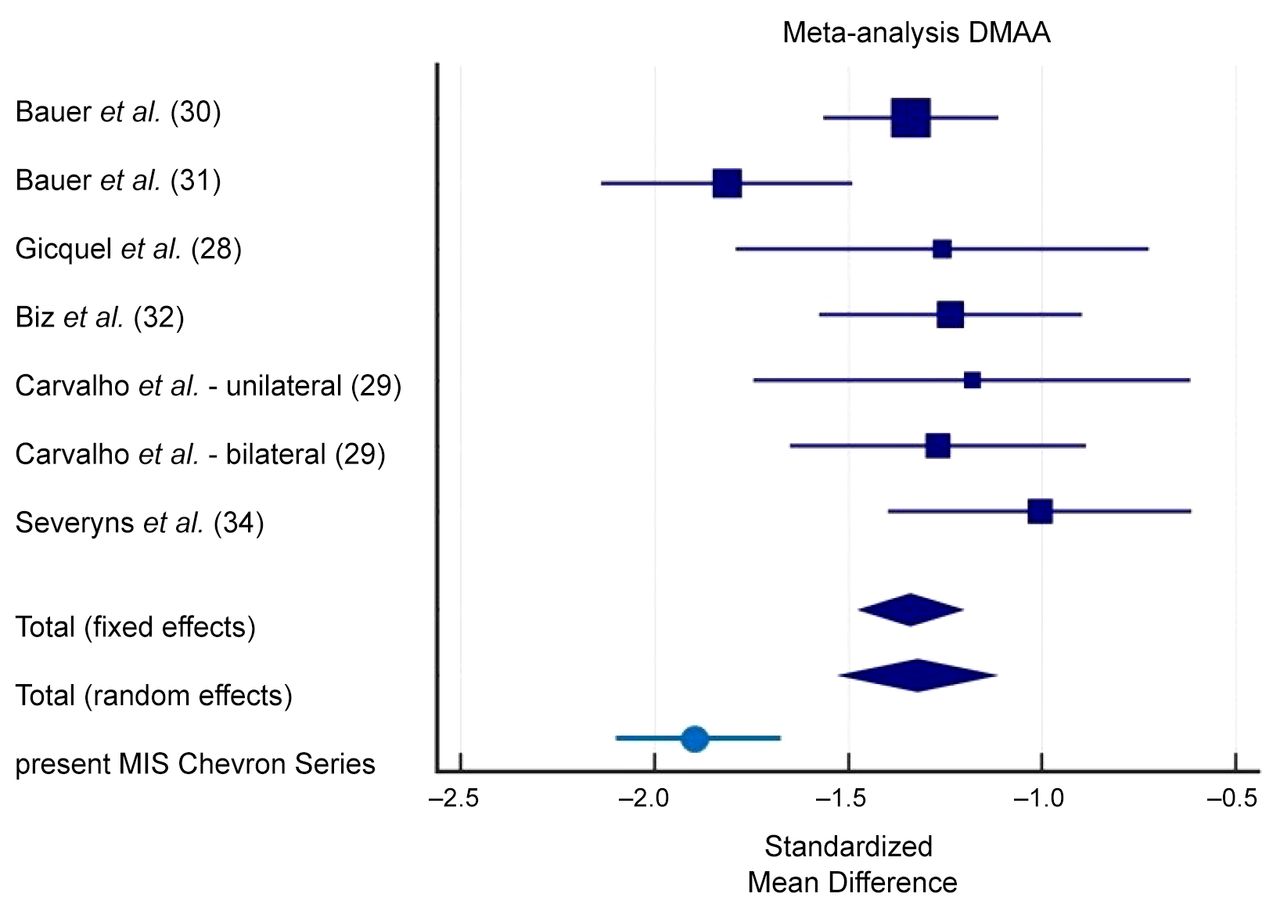
Statistical analysis. Statistical analysis was performed using the IBM SPSS Statistics for Windows, Version 24.0 (IBM Corp., Armonk, NY) and MedCalc Statistical Software version 18.2.1 (MedCalc Software bvba, Ostend, Belgium). Descriptive statistical analyses included the calculation of means (range) and medians (IQR) for continuous measures, and numbers (n, with percentages) for categorical variables. Three meta-analyses were performed to integrate the quantitative findings with regard to IMA, HVA and DMAA deformity angles of the selected studies. For the meta-analyses, Hedges g statistics was used as a formulation for the standardized mean differences between baseline and follow-up measurement of the deformity angles. The standardized mean difference Hedges g is the difference between the two means divided by the pooled standard deviation, with a correction for small sample bias. The forest plots show, for each deformity angle, the results of the different studies included in the meta-analysis, with 95% confidence intervals for the standardized mean differences. The diamonds display the aggregated differences (95% confidence intervals), both, for the fixed and the random effects calculation method. Results of our own patients’ series were added to the forest plots. A statistically significant difference (p<0.05) is indicated if the results of the own series does not overlap with the aggregated results of the meta-analysis displayed by the diamonds in the forest plots.
Results
In a first approach the methodological and thus scientific quality of the included papers was investigated using the previously described Methodological Index for Non-Randomized Studies (MINORS) (44), the Coleman Methodology Scale (22) and the level of evidence. Concise details of the included studies concerning the methodological limitations are given in Table I. The reporting criteria are in reference to the critical appraisal tool proposed previously (45). Quality assessment revealed low scientific quality of the analyzed Reverdin-Isham studies. In a second step the studies were assessed with regard to the reported clinical and radiological outcome.
Quality assessment for Reverdin-Isham studies at latest follow-up, MIS chevron (present series) and a Level I MIS chevron study from the literature.
Table II presents patient demographics for the analyzed Reverdin-Isham studies. Concise clinical and radiological data from each included study are presented in Tables III and IV. A significant number of the analyzed Reverdin-Isham studies showed radiographic recurrence for IMA and HVA (Table III). However, scientific quality of the published Reverdin-Isham studies was low.
Demographic data from Reverdin-Isham studies at latest follow-up, MIS chevron (present series) and a Level I MIS chevron study from the literature.
Radiological results from included Reverdin-Isham studies at latest follow-up, MIS chevron (present series) and a Level I MIS chevron study from the literature.
Clinical results from Reverdin-Isham studies at latest follow-up, MIS chevron (present series) and a Level I MIS chevron study from the literature.
Clinical and radiographic results after MIS distal chevron osteotomy are presented in Tables V and VI. Mean follow-up was 58.9 (range=39.0-85.4) months. The MIS chevron showed good correction of all relevant angles of the hallux valgus deformity to all points of survey without major loss of correction until follow-up. Clinical outcome in terms of VAS and AOFAS also showed major improvement to all points of assessment. ROM stayed consistent from pre- to postoperative. Two feet showed radiographic recurrence with a IMA above ten degrees and five feet with a HVA above 20° at latest follow-up. However, only two of these feet showed a reduced AOFAS score as well.
Clinical data of the present MIS Chevron cohort.
Radiological data of the present MIS Chevron cohort.
Radiographic outcomes of the MIS chevron and of the meta-analysis of the MIS Reverdin-Isham osteotomy are shown in Figures 2, 3, and 4 using the forest plot analysis. Outcomes of IMA, HVA, and DMAA are presented separately. Radiographic outcomes were significantly better with the MIS chevron than with the Reverdin-Isham osteotomy (p<0.05).

Forest plot meta-analysis showing the intermetatarsal angle (IMA) results for the various Reverdin-Isham studies (squares) and the present MIS chevron series (circle) with 95% CI. The overall standardized mean difference as well as random effects are shown as well (diamonds).

Forest plot meta-analysis showing the hallux valgus angle (HVA) results for the various Reverdin-Isham studies (squares) and the present MIS chevron series (circle) with 95%CI. The overall standardized mean difference as well as random effects are shown as well (diamonds).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot meta-analysis showing the distal metatarsal articular angle (DMAA) results for the various Reverdin-Isham studies (squares) and the present MIS chevron series (circle) with 95%CI. The overall standardized mean difference as well as random effects are shown as well (diamonds).
Discussion
Our results showed superior radiographic outcomes with regard to IMA, HVA, and DMAA after MIS distal chevron osteotomy compared to MIS Reverdin-Isham osteotomy. However, clinical outcomes were comparable with both techniques.
With the distal MIS chevron osteotomy, we were able to correct IMA, HVA, and DMAA in patients with mild to moderate hallux valgus. The degree of correction found in our study is well in line with the published literature on MIS distal chevron osteotomy (15, 16, 27, 46). PDPAA, joint congruity angle, and sesamoid position showed good correction until final follow-up at a mean of 58.9 (range=39.0-85.4) months as well.
The concept of the MIS distal chevron osteotomy is a sliding maneuver of the first metatarsal head, whereas for the Reverdin-Isham it is a closing wedge technique. In accordance to this, the correction of the deformity can be expected to a greater extent using a MIS distal chevron osteotomy. In our study, a better correction of IMA could be found with the MIS chevron osteotomy than with the MIS Reverdin-Isham technique. Mean postoperative IMA amounted to 11.6° with the Reverdin-Isham method, while with the MIS chevron technique IMA was corrected to 6.1° on the mean. Three of the analyzed Reverdin-Isham studies reported a total correction of 3° for IMA (30-32), while the other three studies even less than 3° (31, 36, 42). Insufficient radiographic correction following the MIS Reverdin-Isham osteotomy has been already described (47). Nevertheless, this procedure was meant to be a valid procedure for correcting a hallux valgus deformity and is still a frequently used minimally invasive technique for hallux valgus correction (47).
Preoperative radiological deformity in terms of IMA, HVA, DMAA, joint congruence and sesamoid position as well as insufficient hallux valgus correction has been linked to hallux valgus recurrence after long-term follow-up (48). Consequently, we feel that for sufficient hallux valgus deformity correction these specific pathological radiographic angles should be corrected to normal. With regard to the definition of a hallux valgus recurrence with a HVA of more than 15° and an IMA of more than 10° (48), radiographic recurrence is likely with the Reverdin-Isham method. In our meta-analysis mean postoperative IMA amounted to 11.6° with the Reverdin-Isham method, what does equate to radiographic recurrence. Interestingly, clinical outcome in terms of AOFAS forefoot score was generally good in the Reverdin-Isham studies as well. This might be a consequence of the variable and short follow-up times of the analyzed studies. At long-term follow-up this might result in clinical appearance of hallux valgus recurrence.
Improvement of clinical outcome in terms of AOFAS forefoot score and VAS, comparable to that in the published literature (15, 30, 38) was found in our cohort of MIS distal chevron osteotomies as well as in the Reverdin-Isham studies (28-32, 34). We did not observe loss of ROM of the first metatarsophalangeal joint after MIS chevron osteotomy. ROM was reported only in 3 of our included Reverdin-Isham studies and showed a slight reduction of ROM. However, this finding had no impact on clinical outcome in terms of AOFAS forefoot score (30, 31, 34).
Our meta-analysis of published literature on MIS Reverdin-Isham osteotomy revealed a high probability of random effects. We ascribe this finding to the poor scientific quality of some Reverdin-Isham publications. Full text assessment revealed a large variety of methodological descriptions, number of included feet and follow-up time. Additionally, demographic data were partially incomplete and the statistical description unprecise. Consequently, only half of the included studies could be used for meta-analysis.
A major limitation of our study stems from the study design, namely a comparison of the results of a cohort treated by the authors with one distinct surgical method and the results of another cohort treated with a different surgical technique. The poor scientific quality of the studies on MIS Reverdin-Isham osteotomy found in the literature is another limitation. The single-observer single-measurement analysis of the present MIS chevron series and the design as a single-center study is another limitation. The most positive aspect remains the size of the patient cohort treated with the MIS distal chevron osteotomy at our department with no drop-outs until follow-up.
Conclusion
MIS distal chevron osteotomy in mild to moderate hallux valgus deformity correction results in superior radiographic outcomes compared to the MIS Reverdin-Isham osteotomy. Sufficient correction of IMA cannot be achieved with the MIS Reverdin-Isham osteotomy.
Acknowledgements
The Authors would like to thank Mary Heaney Margreiter for providing language correction.
Footnotes
Authors’ Contributions
G. Kaufmann: Study protocol, study design, literature research, data analysis, editing and writing of the article. D. Weiskopf: Literature research, data analysis, editing, writing and proofreading of the article. M. Liebensteiner: Co-editing, proofreading of the article. H. Ulmer: Data analysis and proofreading of the article. M. Braito: Literature research, supervised the study results and proofread the article. F. Endstrasser: Co-editing, proofreading of the article. M. Wagner: Co-editing, proofreading of the article. M. Ban: Literature research, Co-editing, proofreading of the article. D. Dammerer: Study protocol, study design, literature research, data analysis, editing and writing of the article. All Authors made pertinent contributions to the article, and proofread and approved the final article before submission.
This article is freely accessible online.
Conflicts of Interest
The Authors declare that there are no conflicts of interest.
- Received April 6, 2021.
- Revision received April 20, 2021.
- Accepted May 19, 2021.
- Copyright © 2021 International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved