

Abstract
Background/Aim: The neutrophil-to-lymphocyte ratio (NLR) and the density of tumor-infiltrating lymphocytes (TILs) have been reported as immunological prognostic factors for various cancers. We evaluated the association between the prognosis and the immunological status in patients who underwent complete resection of pulmonary metastases of colorectal cancer (CRC). Patients and Methods: We evaluated the associations between the NLR before the resection of pulmonary metastases and the relapse-free survival (RFS) or overall survival (OS), or between the density of TILs in the pulmonary metastasis and the RFS or OS. Results: The RFS and OS were significantly worse in the NLR-High group than in the NLR-Low group. The RFS was significantly longer in the CD3+TILs-High group than in the CD3+TILs-Low group. Conclusion: The NLR and the density of TILs may have prognostic significance in patients who undergo complete resection of pulmonary metastases of CRC.
- Neutrophil-to-lymphocyte ratio
- tumor-infiltrating lymphocytes
- pulmonary metastases of colorectal cancer
Pulmonary metastasis occurs in 10%-29% of colorectal cancer (CRC) patients and is the second most common site of CRC metastasis, after hepatic metastasis (1-6). Surgical resection is widely accepted as the first-line therapy for pulmonary metastasis (7-10). It is currently considered acceptable to resect pulmonary metastasis of CRC while maintaining an adequate pulmonary function, if complete treatment of the primary tumor as well as of all the other metastases have been achieved (7-10). However, the 5-year overall survival (OS) rate after resection of pulmonary metastases ranges from 30% to 68% according to reports (11, 12). Therefore, in order to determine the ideal treatment strategy of pulmonary metastases of CRC, the classification of patients by prognostic factors has been proposed (13-15).
The clinicopathological factors related to the prognosis after resection of pulmonary metastasis of CRC reportedly include the timing of metastasis (metachronous or synchronous) (16), number of metastases (9, 13), diameter of the metastasis (13), distribution of metastasis (ipsilateral or bilateral) (17), mediastinal lymph node involvement (9, 10, 18), carcinoembryonic antigen (CEA) levels before resection of pulmonary metastases (10, 13, 18, 19), primary T/N classification as defined by the Union for International Cancer Control (UICC) 8th (17, 20), and disease-free interval after resection of primary tumor (18). However, the prognostic factors after pulmonary metastasis of CRC have not yet been confirmed.
On the other hand, the immunological status of the host has also been reported to affect the effectiveness of cancer treatment (21, 22). Similar to the primary tumor of CRC, in pulmonary metastasis of CRC, the prognosis may be significantly altered by not only tumor factors but also the immunological status of the host. The neutrophil-to-lymphocyte ratio (NLR) as a systemic inflammatory marker (23-26) and the density of tumor-infiltrating lymphocytes (TILs), which reflects the immunological status in the tumor microenvironment (27, 28), have been reported as immunological prognostic factors for various cancers, including CRC. CRC is one of the few carcinomas with an established therapeutic strategy, which includes resection of distant metastasis. Thus, using the resected surgical specimen, we can examine the immunological status of the tumor microenvironment of pulmonary metastasis.
The present study evaluated the association between the prognosis of patients who underwent radical resection of pulmonary metastases of CRC and the immunological indices described above.
Patients and Methods
Patients. We retrospectively reviewed 17 patients who underwent potentially curative surgery for pulmonary metastases of CRC between January 1998 and December 2018 at Osaka City University. In this study, all primary tumors of CRC were resected radically, and all pulmonary resections that were performed were the first resections of pulmonary metastases of CRC. The 17 cases included patients who had either received chemotherapy or had undergone resection of hepatic metastasis before undergoing the resection of pulmonary metastasis. Pulmonary metastases detected at resection of the primary tumor were defined as synchronous metastases, while those detected after resection of the primary tumor were defined as metachronous metastases.
This retrospective study was approved by the Ethics Committee of Osaka City University (approval number: 3853, 4182) and conducted in accordance with the Declaration of Helsinki. All patients provided their written informed consent.
Methods. The associations between the clinicopathological factors and the relapse-free survival (RFS) or the overall survival (OS) were statistically evaluated. The clinicopathological factors were the primary T/N classification as defined by the Union for International Cancer Control (UICC) 8th (17, 20), synchronous/metachronous metastasis, distribution of metastasis (ipsilateral or bilateral) (17), the number of metastases, the maximum diameter of metastasis, and the CEA level before resection of pulmonary metastasis. In this study, the RFS was defined as the interval between the date of the first complete pulmonary resection and the date of the diagnosis of the first recurrence, the date of death due to any cause, or the date of the last follow-up. The OS was defined as the interval between the date of the first complete pulmonary resection and the date of death due to any cause, or the date of the last follow-up.
To evaluate the correlation between the prognosis and systemic inflammation, the association between the NLR and RFS/OS after resection of pulmonary metastases of CRC was investigated. The NLR was calculated from a blood sample obtained within two weeks before pulmonary resection by dividing the absolute neutrophil count by the absolute lymphocyte count. To determine the appropriate cut-off value, we used a receiver operating characteristic (ROC) curve analysis. Based on the cut-off value, patients were classified into the NLR-High or NLR-Low groups. The RFS or OS after resection of pulmonary metastasis was compared between the NLR-High and NLR-Low groups.
The immunological status in the tumor microenvironment was evaluated based on the association between the density of TILs in the specimen of the pulmonary metastasis and the prognosis after resection of pulmonary metastasis. Setting CD3 as the pan-T cell marker and CD8 as the cytotoxic T cell marker, the TILs of the pulmonary metastatic tumor sample were examined with immunohistochemical staining by anti-CD3 antibody and anti-CD8 antibody (CD3: Monoclonal Mouse Anti-Human CD3 CloneF7.2.38, 1:200 dilution; Dako, Glostup, Denmark; CD8: Monoclonal Mouse Anti-Human CD8 Clone C8/144B M7103, 1:200 dilution; Dako). The number of CD3+TILs and CD8+TILs at the invasive margin of the tumor was counted in 5 randomly selected fields at a magnification of ×400, and the mean of the values obtained was used (Figure 1). The cut-off value was determined using the ROC curve analysis. Based on this cut-off value, patients were classified into the TILs-High or TILs-Low groups. The RFS or OS after resection of pulmonary metastasis was compared between the TILs-High and TILs-Low groups.
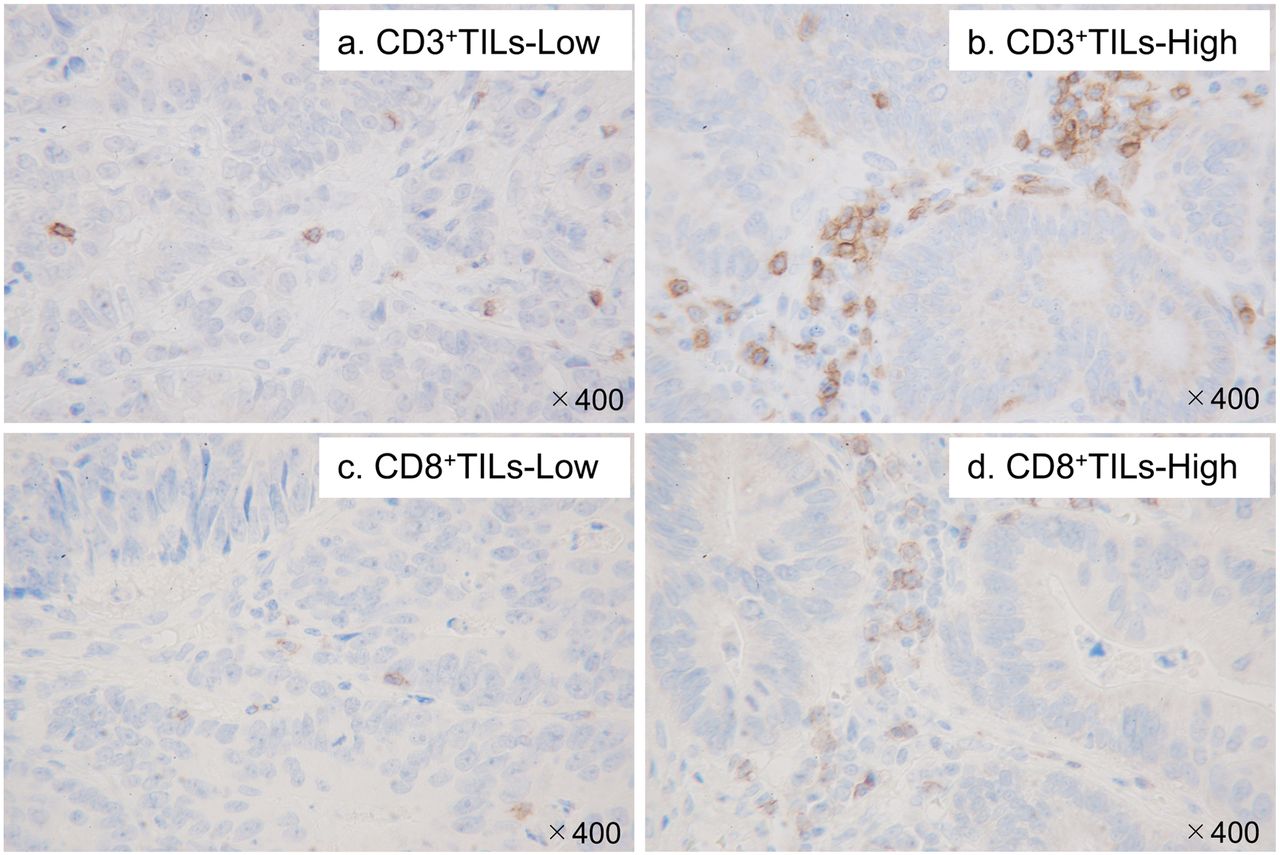
Tumor-infiltrating lymphocytes of pulmonary metastases of colorectal cancer. Immunohistochemical detection of the low (a) and high (b) presence of CD3+ tumor-infiltrating lymphocytes and the low (c) and high (d) presence of CD8+ tumor-infiltrating lymphocytes.
Statistical analyses. All statistical analyses were performed using the JMP software program, ver. 14.2.0 (SAS Institute, Japan, Tokyo). Fisher’s exact test was used to analyze the association between each high and low group. Survival curves were made using the Kaplan-Meier method. Differences in the RFS or OS were assessed using the log-rank test. A multivariate analysis of the clinicopathological factors that were correlated with the survival was performed using a Cox proportional hazards model. Factors with a p-value of <0.1 on the univariate analysis were included as a covariate in the multivariate analysis. A p-value of <0.05 was considered to indicate a statistically significant difference.
Results
Patient characteristics. The 17 patients’ characteristics are summarized in Table I. The study cohort included 8 males and 9 females, with a median age of 72 years old (range=57-84 years old). The primary tumor site was located on the right in 3 patients (from the cecum to transverse colon) and on the left in 14 patients (from the descending colon to rectum). The T factor was ≤T3 in 12 patients and T4 in 5 patients. The N factor was N0 in 7 patients and ≥N1 in 10 patients. The histological type of all patients was well- or moderately-differentiated adenocarcinoma. Ten patients had synchronous pulmonary metastasis, and seven had metachronous pulmonary metastasis. Eleven had only one lesion of pulmonary metastasis, and six patients had more than two lesions. Sixteen patients had pulmonary metastasis in one lung field, and one patient had pulmonary metastasis in both lung fields. The maximum diameter of pulmonary metastasis was <20 mm in 11 patients and ≥20 mm in 6 patients. The CEA level within 2 weeks before resection of pulmonary metastasis was ≤5 ng/ml in 12 patients and >5 ng/ml in 5 patients. Eight patients were treated with pulmonary resection alone, and nine patients were treated with pulmonary resection and postoperative adjuvant chemotherapy.
Patient clinicopathological characteristics before the resection of the pulmonary metastases and association between NLR/TILs and the clinicopathological characteristics.
The survival rate after complete resection of pulmonary metastases of CRC. In this study, twelve patients (70.6%) had recurrence, and the 5-year RFS rate after complete resection of pulmonary metastases of CRC was 22.6%. Seven mortality events (41.2%) occurred after complete resection of pulmonary metastases of CRC. The 5-year OS rate after complete resection of pulmonary metastases of CRC was 54.5%.
The association between the NLR and the RFS/OS. We used the NLR, which was a continuous variable, as the test variable and the occurrence of all-cause mortality as the state variable. When we investigated the cut-off value for the NLR using the ROC curve, we found that the appropriate cut-off value for the NLR was 2.5 (sensitivity of 71.4%; specificity of 90.0%) (Figure 2). We therefore set that value as the cut-off, and the patients were then classified into high and low groups.

Receiver operating characteristic curve of the neutrophil-to-lymphocyte ratio for the overall survival status. Area under the curve=0.714; 95% confidence interval=0.320-0.930; p=0.038.
Eleven patients were in the NLR-Low group, and six were in the NLR-High group. Regarding the patients’ characteristics before resection of pulmonary metastasis, a high NLR was significantly correlated with the lymph node metastasis of the primary tumor (p=0.035). However, no significant differences in any other characteristics were found between the NLR-Low and NLR-High groups (Table I). The RFS and OS after resection of pulmonary metastasis were significantly worse in the NLR-High group than in the NLR-Low group (p=0.001, p=0.003, respectively) (Figure 3a and b).

The association between the neutrophil-to-lymphocyte ratio and the survival status. (a) The association between the neutrophil-to-lymphocyte ratio and the relapse-free survival after resection of pulmonary metastases. (b) The association between the neutrophil-to-lymphocyte ratio and the overall survival after resection of pulmonary metastases.
The association between the density of TILs and the RFS/OS. We used the number of positive TILs, which was a continuous variable, as the test variable and the occurrence of all-cause mortality as the state variable. When we investigated the cut-off value for the number of positive TILs using the ROC curve, we found that the appropriate cut-off value for the CD3+TILs was 31 (sensitivity of 85.7%; specificity of 50.0%) (Figure 4a). Using the ROC curve in the same manner, we set the cut-off value for the CD8+TILs at 21 (sensitivity of 100.0%; specificity of 40.0%) (Figure 4b). We therefore set each value as the cut-off value, and the patients were then classified into high and low groups.

Receiver operating characteristic curve of the number of tumor-infiltrating lymphocytes for the overall survival status. (a) The overall survival status and CD3+ tumor-infiltrating lymphocytes. Area under the curve=0.714; 95% confidence interval=0.415-0.898; p=0.109. (b) The overall survival status and CD8+ tumor-infiltrating lymphocytes. Area under the curve=0.686; 95% confidence interval=0.378-0.887; p=0.240.
Seven patients were in the CD3+TILs-High group, and 10 were in the CD3+TILs-Low group. No significant differences were found between the CD3+TILs-Low and CD3+TILs-High groups in the patient’s characteristics before resection of pulmonary metastasis (Table I). The RFS after resection of pulmonary metastases was significantly longer in the CD3+TILs-High group than in the CD3+TILs-Low group (p=0.041) (Figure 5a). The OS after resection of pulmonary metastases tended to be longer in the CD3+TILs-High group than in the CD3+TILs-Low group (p=0.097) (Figure 5b).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The association between tumor-infiltrating lymphocytes and the relapse-free and overall survival. (a) The association between CD3+ tumor-infiltrating lymphocytes and the relapse-free survival after resection of pulmonary metastases. (b) The association between CD3+ tumor-infiltrating lymphocytes and the overall survival after resection of pulmonary metastases. (c) The association between CD8+ tumor-infiltrating lymphocytes and the relapse-free survival after resection of pulmonary metastases. (d) The association between CD8+ tumor-infiltrating lymphocytes and the overall survival after resection of pulmonary metastases.
Five patients were in the CD8+TILs-High group and 12 were in the CD8+TILs-Low group. No significant differences were found between the CD8+TILs-Low and CD8+TILs-High groups in the patient’s characteristics before resection of pulmonary metastasis (Table I). Furthermore, no significant differences in the RFS/OS were found between the CD8+TILs-Low and CD8+TILs-High groups (Figure 5c and d).
The evaluation of the prognostic factors for the RFS/OS. In the univariate analysis, the RFS after resection of pulmonary metastases was significantly shorter in the group with ≥2 pulmonary metastases, the NLR-High group and the CD3+TILs-Low group than the corresponding reference groups (p=0.013, p=0.025, p=0.038, respectively) (Table II). In the multivariate analysis, the number of pulmonary metastases and the NLR before resection of pulmonary metastasis were found to be independent prognostic factors of the RFS (p=0.007, p=0.002, respectively) (Table II). Furthermore, in the univariate analysis, the OS after resection of pulmonary metastases was significantly shorter in the NLR-High group than in the NLR-Low group (p=0.008), and the OS after resection of pulmonary metastases tended to be shorter in the CD3+TILs-Low group than in the CD3+TILs-High group (p=0.077) (Table III). In the multivariate analysis, the NLR before resection of pulmonary metastasis was the only independent prognostic factor of the OS (p=0.009) (Table III).
Univariate and multivariate analysis of relapse-free survival after resection of pulmonary metastases.
Univariate and multivariate analysis of overall survival after resection of pulmonary metastases.
Discussion
In recent years, advances in treatment, such as metastasectomy or systemic chemotherapy, have improved the prognosis of patients with distant metastasis of CRC. However, the mortality and recurrence rates can be improved further. The identification of patients who can most benefit from each treatment is therefore necessary, and to this end, various biomarkers have been reported as the prognostic predictors (13, 14, 29).
The systemic inflammatory response has been recognized as being associated with the tumor progression. Thus, the association between systemic inflammatory markers and the clinical outcome has been reported in various types of cancer, including CRC (23-26). Neutrophils play an important role in tumor growth, invasion, and metastasis. Thus, an increase in the neutrophil count has been considered to reflect the progression of cancer (30). In contrast, lymphocytes play an important role in anti-tumor immunity and are related to the immune system of the host. A decrease in lymphocytes reportedly reflects the deterioration of the anti-tumor immunity and is associated with a poor prognosis (31). Thus, a high NLR means that the status of the host is favorable for cancer progression, suggesting that the NLR is a useful prognostic predictive biomarker (32).
The association between the prognosis and the NLR in CRC patients has often been reported (23, 24, 33, 34). We have previously found that the preoperative NLR was a predictor of a poor prognosis after radical resection for CRC (35) and that the NLR was a prognostic predictor in patients with stage IV CRC who underwent palliative resection of asymptomatic primary tumor (29). Thus, the NLR appears to be useful for determining the prognosis of patients with radical resection of pulmonary metastases of CRC.
In the present study, patients with a high NLR before resection of pulmonary metastasis had a poor prognosis. Therefore, regarding patients with pulmonary metastasis of CRC, our findings suggested that clarifying the systemic inflammation status by sampling preoperative blood might be an easy and useful method for predicting the prognosis after the resection of pulmonary metastases.
On the other hand, the presence of immune cells in the tumor microenvironment is considered to be related to the progression of cancer. Indeed, the density of TILs, which reflects the anti-tumor immune status of the host, has been reported to be a useful biomarker for predicting the therapeutic outcome or prognosis (27, 28). In CRC in particular, the density of CD8+TILs and total T-lymphocytes is correlated with the anti-tumor immune status of the host, and these values are components of the ‘Immunoscore’, which is an immunological biomarker in CRC (36, 37).
The density of TILs in the primary tumor has often been reported to be a useful predictor of the therapeutic outcome; however, relatively few reports on the density of TILs in metastatic tumor have been published compared to reports on the density of TILs in primary tumor. In general, resection of metastatic tumors is rare, and the evaluation of the local immune status in metastatic tumor is not easy. However, the therapeutic strategy for CRC includes resection of distant metastases, and we can evaluate the local immune status in distant metastatic lesions. Our research group has previously shown that the density of TILs in the primary tumor of CRC correlated with the density of TILs in the hepatic metastasis removed by synchronous resection (38). In that study, we suggested that the evaluation of the local immunity of the primary tumor might be a substitute for the evaluation of the local immunity of the metastatic lesion (38). However, in cases of two-stage resection of a synchronous metastatic tumor or resection of a metachronous metastatic tumor, the immune status may change between the primary tumor and the metastatic tumor. This is due to the passage of time between resection of the primary tumor and that of the metastatic tumor or due to the treatments performed in that interval. In general, simultaneous resection is difficult in cases of pulmonary metastasis of CRC, so the immune status of the pulmonary metastasis of CRC may differ from that at the time of resection of the primary tumor of CRC. Therefore, the re-evaluation of the immune status of the host by evaluating the density of TILs in the metastatic tumor may be significant for the prediction of the prognosis. In the present study, the density of CD3+TILs was significantly associated with the RFS after resection of pulmonary metastasis. Therefore, the re-evaluation of the density of TILs in pulmonary metastasis may lead to predict the prognosis after resection of pulmonary metastasis of CRC.
The density of CD8+TILs, by contrast, was not shown to be associated with the RFS or the OS in the present study. However, this study was conducted in a small number of patients, so we considered the density of CD8+TILs to nevertheless be an important immunological factor, as in previous reports.
Several limitations associated with the present study warrant mention. First, this study was retrospective and included a relatively small number of patients who had received resection of pulmonary metastasis at a single institution. Second, in the past 20 years, advances in surgical techniques and chemotherapy have changed the criteria of resection of pulmonary metastasis, the regimens of adjuvant chemotherapy after resection of pulmonary metastasis and the regimens of systemic chemotherapy at the time of recurrence after resection of pulmonary metastasis. Thus, the patients’ background characteristics may have differed between older and newer cases. Therefore, a prospective study should be performed in the future.
In conclusion, the present study revealed that the immunological status of the host affected the therapeutic effects and the prognosis of patients with pulmonary metastasis of CRC, and immunological indices, such as the preoperative NLR and the density of TILs, may have prognostic significance as biomarkers for patients who undergo complete resection of pulmonary metastases of CRC.
Acknowledgements
This research received no specific grants from any funding agency in the public, commercial or not-for-profit sectors. The Authors thank Mr. Brian Quinn for providing medical writing services on behalf of Japan Medical Communication (JMC), Japan.
Footnotes
Authors’ Contributions
YO and MS designed the study. YO performed the statistical analysis and draft the manuscript. MS, HN, TF, YI and EW collected the clinical data and revised the manuscript critically. SK, HT, KM, KH and MO designed the study and critically reviewed the manuscript. All Authors read and approved the final manuscript.
This article is freely accessible online.
Conflicts of Interest
The Authors declare that they have no competing interests in regard to this study.
- Received November 13, 2020.
- Revision received November 27, 2020.
- Accepted November 28, 2020.
- Copyright© 2021, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved