

Abstract
Background/Aim: Carboplatin-containing treatment regimens demonstrate moderate efficacy in metastatic castration-resistant prostate cancer (mCRPC). In this study, we retrospectively analyzed the efficacy of carboplatin in relation to blood-based parameters. Patients and Methods: A retrospective chart review was performed for 20 patients with mCRPC who received carboplatin in a single center. Results: Median overall survival was 3.8 months (95%CI=1.5-7.1), median progression-free survival was 1.7 months. We observed two partial remissions (PR, 10%), four stable diseases (SD, 20%) and 14 disease progressions (PD, 70%), resulting in a clinical benefit rate of 30%. A doubling of NSE (neurone specific enolase) values was associated with a 19% absolute higher response rate (95%CI=14-23, p=0.027). All other laboratory parameters failed as predictive markers of response to carboplatin. In univariate Cox regression analysis, only NSE was significantly associated with impaired PFS (HR=0.7, 95%CI=0.56-0.96, p=0.030). Conclusion: Carboplatin showed moderate efficacy against mCRPC in this unselected population of patients and NSE levels may help to predict the success of this treatment.
- Metastatic castration-resistant prostate cancer
- carboplatin
- neurone specific enolase
Prostate cancer is the most common type of cancer in men and in the setting of metastatic spread still a leading cause of cancer-related deaths worldwide (1). In particular, treatment of metastatic castration-resistant prostate cancer (mCRPC) is still challenging. A number of drugs for men with advanced mCRPC are available, including inhibitors of the androgen receptor (AR) pathway (abiraterone acetate, enzalutamide), taxanes (docetaxel, cabazitaxel) and the radionuclide radium-223 (2, 3). Despite these, cross-resistance and progression on these drugs are challenging factors (4, 5). Early studies have reported moderate activity and pronounced effects on pain management for platinum-containing regimens (6, 7).
Given the moderate response rate and the potential side effects of carboplatin-containing regimens as well as the poor performance status and co-morbidities of heavily pre-treated mCRPC patients, the search for predictive biomarkers to better select patients is warranted. Recently, some smaller retrospective studies suggested that only mCRPC patients carrying specific genetic lesions or DNA repair defects, such as alterations in RB1 or BRCA2 might show an improved sensitivity to carboplatin treatment and could benefit from this chemotherapeutic agent (8, 9). Others studies have suggested that patients with neuroendocrine (-differentiated) prostate cancer or the rare small cell carcinoma of the prostate can expect an adequate response to carboplatin treatment, while only a minority of patients with adenocarcinoma histology demonstrate a clinical benefit (1, 10). Thus, data for the efficacy of carboplatin in patients with mCRPC remains controversial and there is currently no consistent recommendation with regards to the clinical scenario where carboplatin should be administered. Therefore, the aim of this study was to identify potential predictive blood-based biomarkers in mCRPC patients treated with carboplatin-based regimens in real-life conditions.
Patients and Methods
Study design, patient cohort and clinical outcome. In this single-center, retrospective cohort study, we included patients with histologically confirmed prostate cancer who were treated with carboplatin-containing regimen at the Division of Oncology, Medical University of Graz, Austria. Using our in-house electronic database, we identified 26 patients diagnosed with metastatic prostate cancer who were treated with carboplatin between 2009 and 2018. Of these patients, four were excluded due to a secondary malignant disease and two were excluded because they had a neuroendocrine (small cell) primary histology, which is well-known to behave differently to carboplatin-based drugs (1, 10). The final analysis population consisted of 20 patients with classical adenocarcinoma histology. Baseline and follow-up data were extracted from paper-chart archives and from our hospital's electronic health record database. Laboratory biomarkers were derived from routine laboratory analyses of whole blood samples and were extracted within a timeframe of maximum 6 days prior to start of carboplatin treatment. The biomarkers were: i) prostate-specific antigen (PSA), ii) neuron-specific enolase (NSE), iii) chromogranin A (CgA), iv) alkaline phosphatase (AP), v) aspartate aminotransferase (AST), vi) alanine aminotransferase (AST), vii) lactate dehydrogenase (LDH), viii) C-reactive protein (CRP), ix) absolute leukocyte count, x) absolute neutrophil count, xi) absolute lymphocyte count, xii) glomerular filtration rate (GFR), xiii) albumin and xiv) gamma-glutamyl transferase (GGT).
The primary endpoint of this study was the response rates defined according to RECIST 1.1 criteria and the Prostate Cancer Clinical Trials Working Group (PCWG2) (11). Secondary endpoints were overall survival (OS) and progression-free survival (PFS). We defined the start of carboplatin therapy as the baseline date. Follow-up was truncated at 12 months for OS and 6 months for PFS analyses.
Ethics statement. The local ethics committee (Ethikkommission der Medizinischen Universität Graz, IRB00002556) approved this study (number 31-282 ex 18/19). Written informed consent was not obtained from individual patients because the local ethics committee specifically granted a waiver of consent for this retrospective database study.
Statistical analysis. Statistical analyses were performed using Stata (Mac version 15.1, Stata Corp., Houston, TX, USA). Continuous variables were summarized as medians (25th-75th percentile) and categorical variables were reported as absolute counts and percentages. Laboratory biomarkers were log2-transformed due to their skewed distribution. Wilcoxon's rank sum test was used to analyze differences between two groups. Wilcoxon's sign rank test was used to analyze changes in laboratory biomarker levels over carboplatin treatment. The association between clinical benefit and continuous laboratory parameters (log2-transformed) was analyzed using univariate logistic regression and absolute changes of clinical benefit were reported as doubling per parameter (i.e. 1-unit increase of the log2-transformed variable). Probabilities of progression-free and overall survival were computed using Kaplan-Meier estimators, and compared between two or more groups using log-rank tests. For graphical illustration of Kaplan-Meier curves, baseline laboratory parameters were dichotomized into a binary variable with an empiric cut-off at their median values. Univariate modeling of PFS and OS was performed using COX proportional hazards models. Due to the low number of patients, multivariate analysis was not performed. The proportionality of hazard assumption was assessed by fitting an interaction between linear follow-up time and the variable of interest. A linear mixed-effects regression model with a random-intercept at the patient level was performed to examine changes in blood biomarkers during progression on carboplatin treatment. This model accounts for the unbalanced biomarker data (missing data) and for the clustered nature of biomarker measurements within individual patients. The model parameters were estimated using maximum likelihood and an independent variance-covariance structure was assumed for the random effects.
Baseline characteristics of the total study cohort.

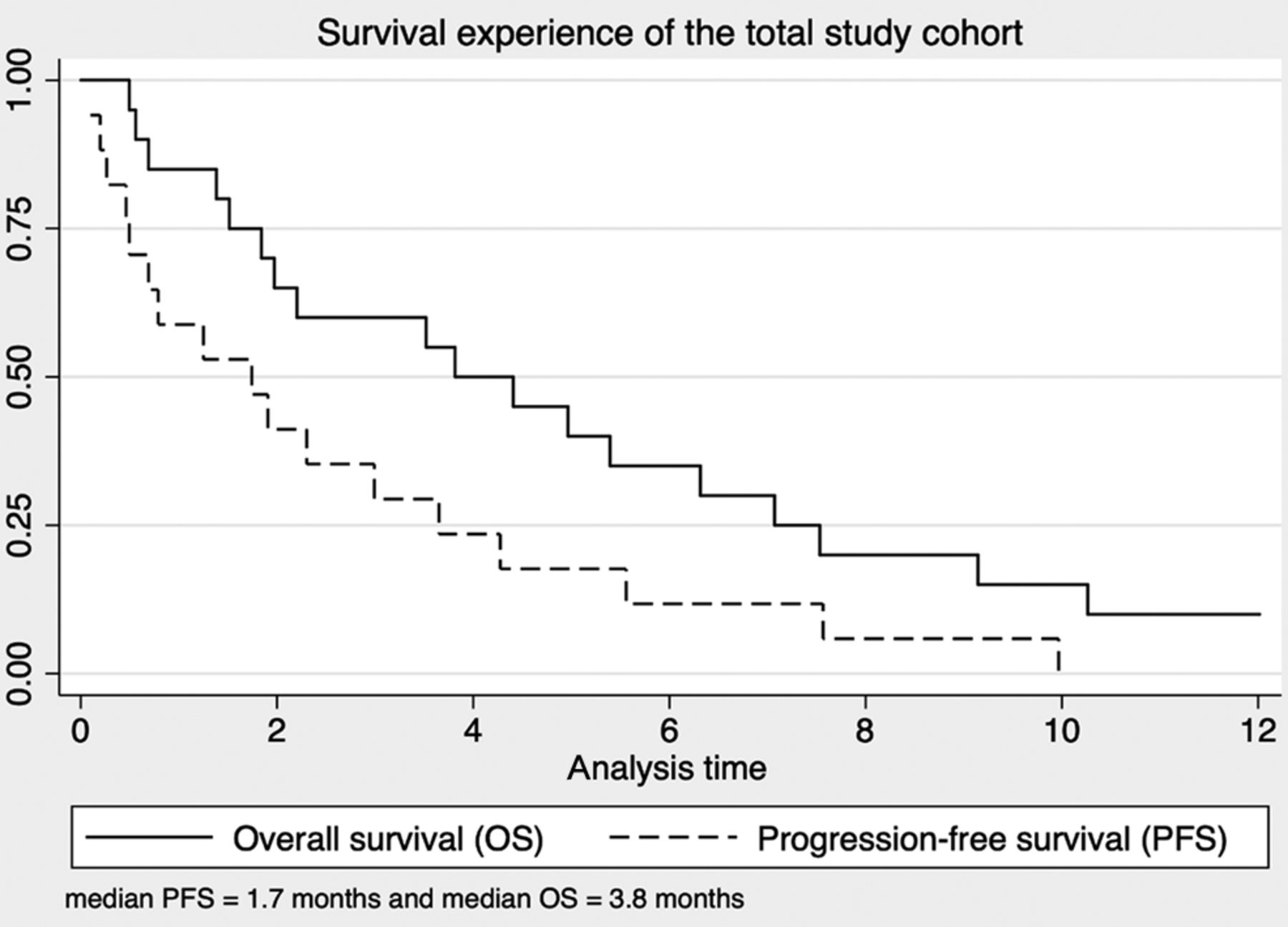
Kaplan-Meier estimates for overall survival (OS) and progression-free survival (PFS) of the total patient cohort.
Results
Patient characteristics at baseline. In this retrospective study, we included twenty consecutive patients with metastatic prostate cancer who received a carboplatin-containing treatment regimen (Table I). The median age of our patients was 65 years (interquartile range=62-69 years) at the start of carboplatin treatment. Nine patients (45%) had previously undergone a radical prostatectomy, three patients (15%) had been through radiation therapy of the prostate and eight patients (40%) had no local therapy. The majority of patients (60%) had visceral metastases and 70% of patients had a Gleason score ≥8. Most patients (80%) had previously received docetaxel treatment. All patients (100%) progressed and 18/20 patients (90%) died within one year of follow-up. Median OS was 3.8 months (95%CI=1.5-7.1), 6-month OS was 35% (range=16-55) and 12-month OS was 10% (range=2-27). Median PFS was 1.7 months and 6-months PFS was 12% (range=2-31) (Figure 1).
Association of baseline blood biomarkers with radiographic response. Based on RECIST 1.1. criteria, we observed i) two partial remissions (PR, 10%), ii) four stable diseases (SD, 20%) and iii) 14 disease progressions (PD, 70%) during the treatment course of these 20 patients with carboplatin. The corresponding clinical benefit rate (a composite of PR+SD as best response) was 30% (95%CI=12-54). In univariate logistic regression analysis (Table II), only NSE levels emerged as a predictor of clinical response. In detail, a doubling of NSE was associated with a 19% absolute higher response rate (95%CI=14-23, p=0.027). All other laboratory parameters, as well as age and Gleason score failed as predictive markers of response.
Baseline laboratory biomarkers as univariate predictors of clinical benefit.
Changes of blood biomarkers over carboplatin treatment. We examined changes in the levels of blood biomarkers over carboplatin treatment (Table III) and found only NSE to significantly decrease during carboplatin treatment (Wilcoxon sign-rank test, p=0.012). A linear mixed model with a random intercept at the patient level (Figure 2) showed that patients experiencing a clinical benefit had a significantly higher mean baseline estimate for NSE (7.8, 95%CI=6.8-8.7) compared to those with disease progression (5.7, 95%Cl=5.1-6.3, p=0.003). This difference at baseline was statistically significant (mean difference=2.1, 95%CI=0.9-3-2, p<0.0001). In contrast, after treatment, similar NSE estimates were observed between patients with PD and patients with a clinical benefit (mean difference=-0.6, 95%CI=-1.7-0.5, p=0.292). In addition, only patients with clinical benefit revealed a significant decrease in mean NSE estimates after carboplatin treatment (mean difference=-2.7, 95%CI=−3.8-1.5, p<0.0001), while patients with disease progression had rather constant mean estimate levels before and after treatment (mean difference=−0.5, 95%CI=−1.5-0.5, p=0.3611).
Changes of blood biomarkers over carboplatin treatment.
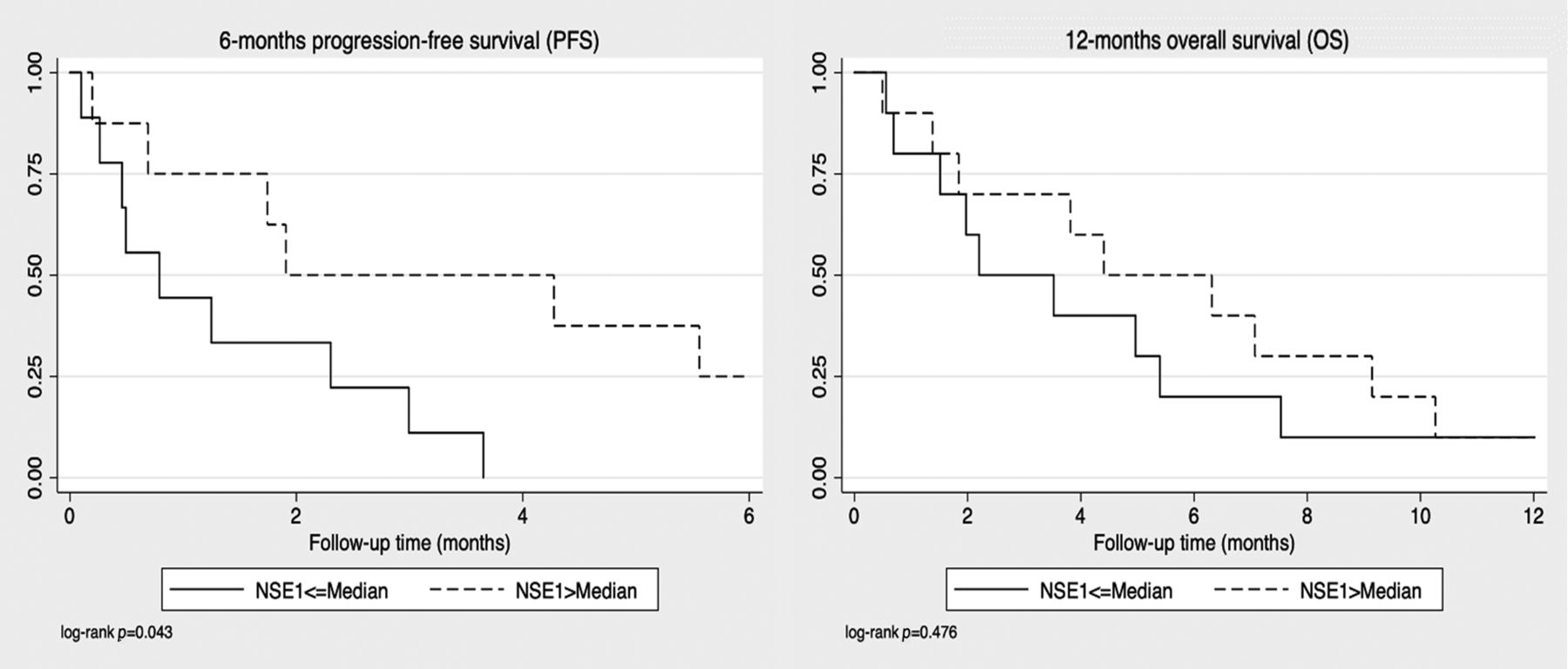
Association of blood biomarkers with clinical outcome. In univariate Cox regression analysis using laboratory biomarkers as continuous variables (Table IV) only NSE was significantly associated with impaired PFS (HR=0.7, 95%CI=0.56-0.96, p=0.030). ALT (HR=1.6, 95%CI=0.92-2.93, p=0.095), leukocytes (HR=0.5, 95%CI=0.22-1.07, p=0.073), and neutrophils (HR=0.5, 95%CI=0.25-1.04, p=0.063) were numerically associated with impaired PFS, but this was not statistically significant. In univariate Cox regression, none of the biomarkers was associated with impaired OS (Table IV). PSA (HR=1.1, 95%CI=0.99-1.26, p=0.074), ALT (HR=1.6, 95%CI=0.98-2.74, p=0.058), and GFR (HR=0.3, 95%CI=0.06-1.09, p=0.065) were numerically associated with impaired OS, but again this was not statistically significant. For Kaplan-Meier estimates, we used an empirically chosen cut-off at the median biomarker level. When using baseline NSE as a dichotomized variable, a lower median NSE was significantly associated with an impaired PFS (Figure 3 left panel, p=0.033, log-rank) but not with impaired OS (Figure 3 right panel, p=0.476, log-rank). When using dichotomized biomarker, only higher median PSA significantly associated with shorter OS (Figure 4 right panel, p=0.023, log-rank) but not with shorter PFS (Figure 4 left panel, p=0.129, log-rank).
Discussion
We examined the response rate, clinical benefit and median PFS/OS intervals in mCRPC patients treated with carboplatin, since the use of platinum agents in advanced prostate cancer is still controversially discussed.
In our study, 14 of 20 patients (70%) did not show radiological response under carboplatin treatment, resulting in a clinical benefit rate of only 30%. Of the 6 patients with clinical benefit, two had a partial remission, while 4 patients remained stable. A prospective clinical trial conducted by Fléchon et al. has obtained similar results (12). Of 55 patients treated with a combination of carboplatin and etoposide, 9% showed partial response and 26% stable disease, while 65% had progressive disease at the end of treatment, which lead the authors to the conclusion that the given combination treatment cannot be recommended in patients with mCRPC (12). In line with these findings, several other authors have suggested that carboplatin-containing treatment cannot be recommended for unselected patients with advanced prostate cancer due to rather low response rates and given toxicity (2, 3, 12, 13).

Predicted mean estimates of the log2-transformed NSE levels using a linear mixed model with a random intercept at the patient level. Each line corresponds to a different type of response to treatment (red line clinical benefit, black line progressive disease). PD: Progressive disease; NSE: neuron specific enolase.
Baseline laboratory biomarkers as univariate predictors of clinical outcome.
In our patient cohort, median OS and median PFS were moderate with 3.8 months and 1.7 months, respectively. Boumann-Wammes et al. have conducted a randomized controlled trial in mCRPC patients, comparing docetaxel monotherapy to a combination of docetaxel and carboplatin. This trial has demonstrated no significant difference in either PFS or OS for the two treatment groups, however, the combination therapy resulted in substantially increased toxicity. These data also support the assumption that the use of carboplatin is linked with little to no response but bears more side effects in unselected patients (3).
Other studies have suggested that specific subtypes of advanced prostate cancer, such as small cell prostate cancer, or carriers of DNA repair defects might in fact benefit from therapy with platinum agents (1, 8, 9, 13, 14). Histological and immunohistochemical features of small cell prostate carcinoma are found in 8-10% of patients dying from mCRPC, while it is rarely detected at the time of initial diagnosis. Aparicio et al. have shown that 74 of 113 patients with clinical features of anaplastic prostate cancer, defined as extensive local disease, visceral disease or low PSA levels with large tumor burden, show no progression after four cycles of carboplatin and docetaxel treatment (10, 15). As platinum-based chemotherapies are standard in small cell lung cancer (13), platinum treatment is also supposed to be efficient in small cell prostate cancer, although no randomized clinical trials have been performed so far to prove this hypothesis in this specific prostate cancer population.
Specific DNA repair defects have been associated with platinum sensitivity. For example, a case report of a patient with mCRPC and BRCA2 frameshift mutation has shown disease regression after six cycles of carboplatin and docetaxel (14). Pomerantz et al. have compared carboplatin response in patients with and without pathogenic germline BRCA2 variants and found a PSA decline >50% in 75% of patients with BRCA2 mutations compared to 17% non-carriers (9). Overall survival was 18.9 months from the start of chemotherapy for pathogenic BRCA2 carriers and 9.5 months for non-carrier. These results suggest that inactivating mutations in BRCA1 or BRCA2 might be predictive biomarkers for the response to platinum-based chemotherapy as was recently shown in analogy for the treatment of PARP inhibitors in the PROFOUND study (8, 9, 14). Similarly, ovarian and breast cancer patients with silencing germline BRCA2 mutations tend to show higher response rates when treated with platinum agents (9). Genomic mutations in RB1, PTEN or Tp53 have also been linked to a better response to platinum therapy (8, 9, 14). Analysis of DNA repair deficiency could be used to select patients who might be most likely to respond to platinum treatment (8, 9, 13, 14).
In our study, we aimed to identify easily accessible and cost-efficient routinely used blood-based biomarkers for the prediction of carboplatin response. The only predictor of clinical response that we identified was the level of NSE. In univariate logistic regression a doubling of NSE was associated with a 19% higher response rate. This association fits to the observation that NSE levels rise with the metastatic disease burden or with neuroendocrine trans-differentiation of prostate cancer. Some experimental data indicate that prostate cancer cells that are histologically identified as adenocarcinoma and depend on AR-signaling at the time of diagnosis might be able to develop features of neuroendocrine carcinoma after exposure to androgen-deprivation therapy (16, 17). Neuroendocrine features might support tumor growth by inhibition of apoptosis and increased neo-angiogenesis, making neuroendocrine prostate cancer a more aggressive cancer type than adenocarcinoma (16).

Kaplan Meier estimates for 6-month PFS (left panel) and 12-month OS (right panel) of patients with NSE levels above and below the median. Patients with NSE levels below the median had a significantly lower PFS than patients above the median (p=0.030, log-rank). NSE: neuron specific enolase.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Kaplan Meier estimates for 6-month PFS (left panel) and 12-month OS (right panel) of patients with PSA levels above and below the median. Patients with PSA levels above the median had a significantly lower OS than patients below the median (p=0.023, log-rank).
A relevant example exists in lung cancer, where NSE has been identified as a biomarker for tumor burden and a predictor of prognosis and treatment response (16). Similarly, prostate cancer with neuroendocrine features might show a better response to carboplatin treatment, which could be the reason why in our study patients with higher NSE levels showed significantly better response to the platinum agent. Suzuki et al. reviewed nine patients with histologically-confirmed treatment-related neuroendocrine prostate cancer who received platinum-based chemotherapy as first line treatment. Seven of nine patients achieved an objective response, indicating that prostate cancer patients with neuroendocrine features can expect an adequate response to platin treatment (18).
In line with this finding, a lower median NSE was significantly associated with an impaired PFS (p=0.043) but not with impaired OS (p=0.476). Whether NSE levels are predictive of carboplatin response in mCRPC patients remains controversial.
A decrease in NSE after carboplatin treatment of mCRPC has been described in various studies (14). In our study, only patients with a clinical benefit revealed a significant decrease in mean NSE estimates after carboplatin treatment, while patients with disease progression had rather constant mean estimate levels before and after treatment. Interestingly, other studies in mCRPC could not identify baseline NSE as a significant predictor of neither response to carboplatin therapy nor of PFS (13, 15, 19, 20).
Our study is not without limitations, mainly due to its retrospective nature. First, the relatively small sample size and heterogenous treatment strategies, including local as well as systemic therapies, may lead to misinterpretation of results and lack of power to detect differences in other biomarkers. Second, we did not perform histological re-evaluation of neuroendocrine or other tumor suppressor gene expression markers, or any genetic testing for BRCA2, BRCA1 or other DNA-repair deficiencies, which will be helpful and necessary in future studies for addressing this agent. Other information, such as pain relief, reduction of use of opioids, life quality and side effects were also not covered by our study, but should be addressed in prospective studies.
The results of our retrospective study indicate that the clinical benefit rate and radiological response of carboplatin treatment for patients with mCRPC is moderate. Carboplatin treatment cannot, therefore, be routinely recommended for unselected patients. NSE could be a biomarker for predicting clinical responses under carboplatin treatment, and NSE should be at least included into prospective trials studying the efficacy of DNA-damaging agents, such as in studies using carboplatin or PARP inhibitors on mCRPC patients.
Footnotes
Authors' Contributions
MP and ND conceived and designed the study. JM collected the clinical information. JM, ND and MP performed statistical analysis and wrote the manuscript. TB, SM, TL and KP reviewed and edited the manuscript. All the Authors read and approved the final manuscript.
This article is freely accessible online.
Conflicts of Interest
The Authors declare no conflicts of interest.
- Received August 10, 2020.
- Revision received September 14, 2020.
- Accepted September 16, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved