

Abstract
Background/aim: Pancreatic cancer is still associated with poor survival rates due to the fact that it is most often diagnosed at advanced stages of the disease when local invasion is present. However, improvements of surgical techniques have enabled extended resections with curative intent. We present the case of a 43-year-old patient diagnosed with locally invasive pancreatic adenocarcinoma invading the portal vein and the common hepatic artery. Case Report: Surgery with curative intent consisting of pancreatoduodenectomy en bloc with hepatic artery resection and portal vein resection was successfully performed. The right hepatic artery was further anastomosed with the remaining common hepatic artery while the left hepatic artery was reconstructed using a reversed splenic artery patch. The continuity of the portal vein was re-established by placing a synthetic prosthesis. Conclusion: Combined arterial and venous resections might be useful in order to achieve a good local control of disease in patients with locally advanced pancreatic cancer.
- Hepatic artery resection
- portal vein resection
- reconstruction
- locally advanced pancreatic cancer
Pancreatic cancer remains one of the most aggressive malignancies worldwide, associated with poor rates of survival due to the biological aggressiveness of the tumor and to its high chemoresistance (1, 2). Moreover, pancreatic tumors tend to remain asymptomatic for a long period of time, being frequently diagnosed at advanced stages of the disease when invasion of vascular structures is already present or when disseminated metastases have developed (3). In such cases, the overall prognosis is extremely poor, with survival of less than 1 year being expected. Therefore, it is estimated that pancreatic cancer currently represents the fourth cause of cancer related death worldwide (1, 2). However, the development of vascular techniques of reconstruction have brought a benefit in terms of survival by providing the opportunity for achieving a radical surgical procedure in cases in which there are no distant metastases. As for the types of vascular structures which might provide a benefit in terms of survival if resected, intensive debates have been conducted. Therefore, in cases presenting venous invasion, the most recent guidelines from the International Study Group for Pancreatic Surgery support demonstrate that venous invasion should no longer be considered as a contraindication for resection, similar rates of long-term survival being reported in cases in which venous resection was needed when compared to cases in which standard pancreatic resections were performed (4). However, in cases with arterial invasion, a clear consensus is still lacking, the indication usually being tailored according to the particularities of each case (2, 5, 6).
In this light, we investigated a 43-year-old male with no significant previous history for diffuse upper abdominal pain and weight loss who was diagnosed with a locally invasive tumor of the pancreatic head.

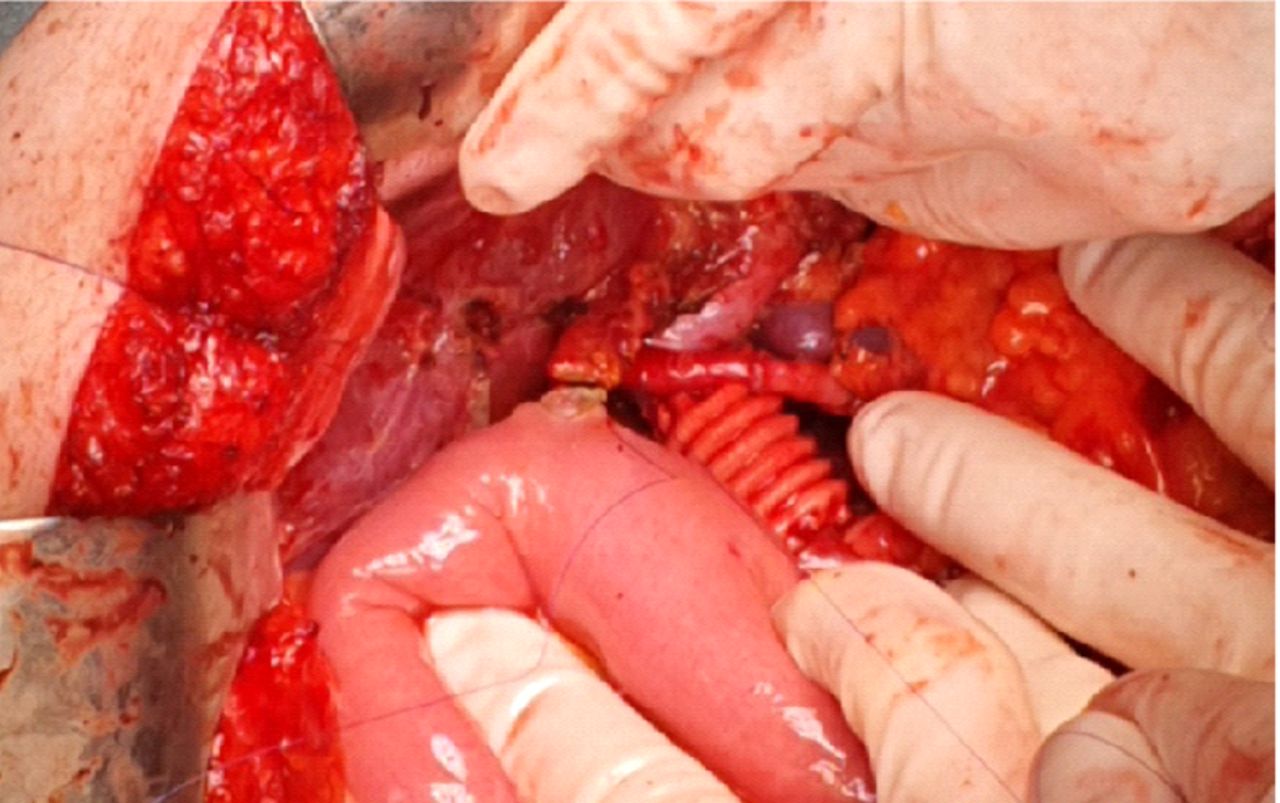
Intraoperative aspect after resection and portal vein reconstruction using a synthetic prosthesis. The celiac trunk is clamped.

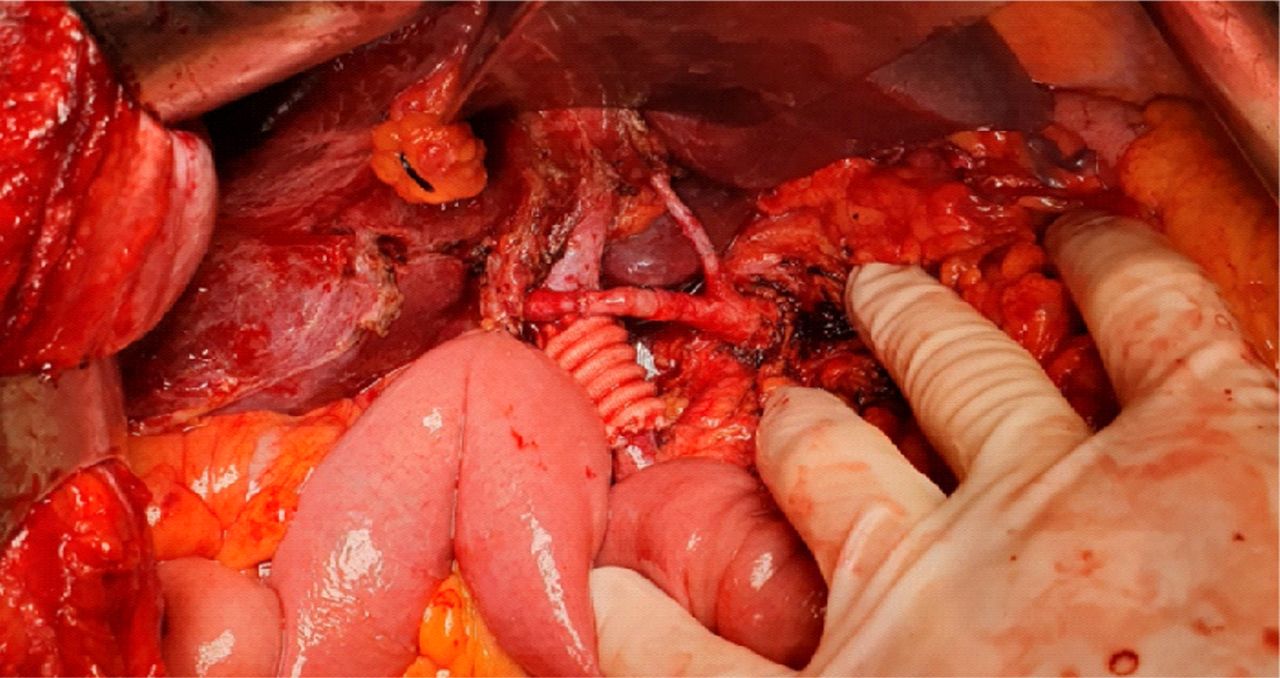
The final aspect after arterial and venous reconstruction.

Intraoperative ultrasound demonstrating the presence of adequate hepatic blood flow.
Case Report
The biopsy retrieved by endoscopic ultrasound revealed the presence of a moderately differentiated pancreatic adenocarcinoma; the method demonstrated the presence of portal vein invasion. The imaging studies were completed by performing computed tomography, which confirmed the presence of a tumor of the pancreatic head measuring 4.2×3.5×3.8 cm, with portal vein and hepatic artery invasion. Therefore, the patient was submitted to irinotecan, oxaliplatin, 5-fluorouracil/leucovorin - FOLFIRINOX-based neoadjuvant chemotherapy. One month after completing neoadjuvant chemotherapy another imagistic evaluation was performed, demonstrating a global decrease of the pancreatic head tumor (which now measured 3.9×3.5×3 cm), as well as an apparently disappearance of the hepatic artery invasion; however, the portal vein was still infiltrated. The patient was submitted to surgery with curative intent, the preoperative intention being a pancreatoduodenectomy en bloc with portal vein resection and reconstruction. Intraoperatively, persistence of the common and proper hepatic artery was found in association with portal vein infiltration; however, tumoral infiltration of the arterial structures proved to be on less than 180° of the vascular circumference. Consequently, the decision was made to continue and to perform surgery with curative intent; pancreatoduodenectomy en bloc with portal vein resection, common and proper hepatic artery resection were performed. The right hepatic artery was anastomosed with the remaining common hepatic artery, while the left hepatic artery was anastomosed with a reversed patch from the splenic artery by means of micro-surgery. The portal vein was reconstructed using a synthetic prosthesis (Figures 1, 2, 3, 4 and 5). Doppler ultrasound confirmed the presence of adequate blood flow at the hepatic level, while the biochemical tests at 48 hours postoperatively demonstrated a slight increase of the serum levels of liver enzymes (aspartate aminotransferase levels measuring 133 U/l). The patient was discharged with a satisfactory general status on the seventh postoperative day.

Bilio-enteric anastomosis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The final aspect after vascular and biliary reconstruction.
Discussion
Due to the close proximity of the pancreatic head with major vascular structures, in a significant number of cases venous and even arterial invasion might be encountered in cancer of the pancreatic head. Such cases have been considered for a long time as unresectable and were submitted to palliative chemotherapy; however, the long-term outcomes remained very poor. For this reason, since techniques of vascular surgery improved, vascular resections have been successfully incorporated into the therapeutic armamentarium for cancer of the pancreatic head (6-12).
However, while the utility of venous resection has been widely demonstrated, similar rates of survival being reported for standard pancreatoduodenectomy and pancreatoduodenectomy and venous resections, the issue of arterial resection and reconstruction has been widely debated (2, 4, 6, 7).
Although the rates of long-term survival after pancreatic resection en bloc with arterial resection and reconstruction seem to be poorer when compared to cases submitted to venous resection, these rates seem to be better when compared to cases submitted to palliative treatment (2, 6-8). A study conducted on this issue was published in 2019 by Del Chiaro et al. (2); it included 73 patients submitted to resection for borderline or locally advanced pancreatic cancer, their outcomes being compared to those of patients diagnosed at similar stages of the disease but submitted only to palliative surgery and chemotherapy. The authors demonstrated that although the rates of postoperative complications were similar for the two groups, the 1-, 3- and 5-year overall survival rates were significantly higher among cases submitted to surgery with curative intent. Regarding the types of vascular reconstructions, all cases necessitating portal vein resections benefited from end-to-end anastomosis, while in cases in which arterial resection was needed, reconstruction consisted of end-to-end anastomosis in 47% of cases, followed by the rotation of the splenic artery in 31% of cases. Other arterial reconstructions consisted of anastomosis on the gastroduodenal stump, autologous or synthetic graft interposition or Appleby procedure; however, the proportion of these reconstructions was significantly lower when compared to direct end-to-end anastomosis or splenic replacement. Interestingly, the authors underlined that the association of neoadjuvant chemotherapy did not significantly influence the long-term outcomes in cases in which radical surgery was achievable. Moreover, there was no significant difference in terms of survival between patients with and without histologically proven arterial infiltration, while cases in which isolated arterial resection was needed tended to have a more favorable outcome when compared to those in which both arterial and venous resections were needed. Therefore, the authors concluded that there is hope for arterial resection to have a similar fate to venous resection in locally advanced pancreatic cancer. While initially it was considered that the presence of venous invasion should be considered as a formal contraindication for resection in pancreatic cancer, further studies have demonstrated that once the perioperative management of these patients has improved, similar long-term outcomes are to be expected in cases submitted to standard resection or to pancreatoduodenectomy in association with venous resections (3, 8, 13, 14). In this respect, Del Chiaro et al. concluded that arterial resection may become widely accepted and part of the standard therapeutic protocol for locally advanced pancreatic cancer with arterial involvement (2).
A similar conclusion was also presented by Amano et al. after studying the long-term outcomes of 17 patients submitted to neoadjuvant chemotherapy followed by pancreatoduodenectomy en-bloc with arterial resection in an article published in 2015 (15). However, in that study, neoadjuvant therapy consisted of gemcitabine and neoadjuvant irradiation, while in Del Chiaro et al.'s study (2), most patients were submitted to the FOLFIRINOX protocol of neoadjuvant chemotherapy.
In regard to the prognostic factors after extended resection for locally advanced pancreatic cancer after neoadjuvant treatment, a recent study conducted by Maeda et al. demonstrated that the presence of arterial invasion did not significantly influence the long-term outcomes as long as negative resection margins were achieved (16); in their study, the authors included 305 patients from three tertiary centers diagnosed with borderline resectable pancreatic cancer submitted to neoadjuvant chemotherapy or chemo-irradiation followed by surgery. They reported a median overall survival of 29.8 months; elderly patients, cases with positive resection margins, presenting poorly differentiated tumors, positive lymph nodes, or positive perineural invasion, as well as those who required administration of adjuvant chemotherapy, had significantly poorer long-term survival rates. Among these 305 cases, 17 required arterial resection followed by reconstruction, negative resection margins being encountered in 88.2% of cases; however, the need for performing arterial resection itself was not a significant prognostic factor for poorer long-term outcomes as long as negative resection margins were achieved (16).
Conclusion
Combined arterial and venous resections seem to be feasible and effective in order to achieve curative resection in locally advanced pancreatic cancer. However, it should be stressed that this surgical procedure is a very demanding one, an attentive selection of cases being mandatory. Although arterial resection is currently not part of the standard therapeutic protocol for locally advanced pancreatic cancer, most recent studies report promising results, which enable us to consider that in the next decade, arterial resection will be considered along with venous resection as feasible and safe procedures in cases diagnosed with locally advanced lesions.
Footnotes
Authors' Contributions
V. Brasoveanu, D. Romanescu and I. Barbu performed the surgical procedure; I. Balescu reviewed literature data and prepared the draft of the article; N. Bacalbasa reviewed the final version of the article. All Authors read and approved the final version of the article.
This article is freely accessible online.
Conflicts of Interest
The Authors have no conflicts of interest to declare regarding this study.
- Received April 23, 2020.
- Revision received May 10, 2020.
- Accepted May 15, 2020.
- Copyright© 2020, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved