

Abstract
Background/Aim: Droplet digital polymerase chain reaction (ddPCR) is an exact method of measuring nucleic acids. The aim of this prospective study was to evaluate minimal residual disease (MRD) using ddPCR in chronic myeloid leukemia (CML) patients. Patients and Methods: Between May 2013 and November 2014, CML patients treated with nilotinib were enrolled in our study. BCR/ABL1 transcripts levels were evaluated using ddPCR at the first time of complete molecular response (CMR). We enrolled 15 patients from 7 Institutions. The treatment period and median follow-up period were 45 months and 47 months, respectively. Results: Patients with a high level of BCR/ABL1 transcript had a greater tendency to lose the CMR during the follow-up period (p=0.095). In addition, patients with a low level of BCR/ABL1 transcript showed a longer duration of CMR compared to those with a high level (p=0.032). Conclusion: We found that ddPCR is a sensitive method for detecting MRD and that MRD could affect the duration of the treatment response.
- Chronic myeloid leukemia
- droplet digital polymerase chain reaction
- minimal residual disease
- complete molecular response
- treatment outcome
Chronic myeloid leukemia (CML) is cytogenetically characterized by the translocation of t(9; 22) (q34;q11.2), which produces the BCR/ABL1 fusion oncogene (1). Since the success of imatinib, the first targeted agent in human history, more effective tyrosine kinase inhibitors (TKIs), such as dasatinib and nilotinib have been introduced to the frontline treatment of CML and show a 76-82% major molecular response rate (2, 3). CML is now thought to be a life-long disease with a 5-year overall survival rate>90% (4).
Previous reports have demonstrated that achievement of an early molecular response is a strong predictive marker of improved outcomes (5). Therefore, the European LeukemiaNet guidelines recommended that the optimal response is a percentage of BCR/ABL1 fusion transcript on the International Scale (BCR/ABL1IS) of <10% at 3 months after initial treatment, followed by <1% at 6 months and 0.1% at 12 months, using quantitative real-time polymerase chain reaction (qRT-PCR) (6). In addition, recent evidence has shown that achievement of a deep molecular response (DMR), including MR4 (BCR/ABL1IS≤0.01%) or MR4.5 (BCR/ABL1IS≤0.0032%), is a surrogate marker of favorable survival and treatment-free remission (7). Currently, selected patients who achieve a DMR can attempt to discontinue TKIs to improve their quality of life and alleviate financial strain (8). Although qRT-PCR is generally used for regular monitoring, additional sensitive methods are needed to detect minimal residual disease (MRD).
Droplet digital polymerase chain reaction (ddPCR) allows the precise quantification of nucleic acids. Due to its positive outcomes, it has been used to detect MRD of hematologic disorders (9). In CML, ddPCR has been validated for the exact measurement of BCR/ABL1 fusion transcripts (10).
We hypothesized that ddPCR would be more sensitive compared to conventional qRT-PCR for measuring oncotranscript levels in patients with a DMR. Therefore, the aim of this study was to evaluate MRD using ddPCR in nilotinib-treated CML patients who firstly achieved a complete molecular response (CMR) as assessed by qRT-PCR. We also evaluated the relationship between ddPCR positivity and patient prognosis.
Patients and Methods
Patient characteristics. From May 2013 to November 2014, we prospectively enrolled Philadelphia chromosome (Ph)-positive CML chronic phase patients who achieved a CMR during treatment with nilotinib. All patients were treated with nilotinib 300 mg twice daily as the first-line target therapy.
Inclusion and exclusion criteria were the same as those in the open-label, multi-institutional phase 4 ENESTKorea trial (11). This study included adult patients diagnosed as Ph-positive CML chronic phase. The diagnosis was confirmed using cytogenetic analysis of at least 20 bone marrow metaphase cells within 6 months before enrollment. The exclusion criteria were as follows: i) CML with atypical BCR/ABL1 transcripts (transcripts other than e13a2 or e14a2, ii) previous treatment with myelosuppressive agents except for hydroxyurea and anagrelide, iii) previous treatment with TKI for over two weeks, iv) previous hematopoietic stem cell transplantation, v) previous irradiation involving 25% or more of the bone marrow tissue, vi) cytopathologically-confirmed central nervous system involvement of CML, vii) Eastern Cooperative Oncology Group performance status≥3 (12), viii) cardiac abnormalities including: a) corrected QT interval≥480 milliseconds on electrocardiogram, b) complete left bundle branch block, c) permanent pacemaker implantation, d) congenital long QT syndrome, e) history of tachyarrhythmia requiring treatment, f) clinically significant resting bradycardia, g) history of acute coronary syndrome within 12 months, and h) decompensated congestive heart failure, ix) organ dysfunction defined by: a) total serum bilirubin levels≥1.5×the upper limit of the normal range (ULN), b) creatinine≥1.5×ULN, c) aspartate or alanine aminotransferase≥2.5×ULN, d) amylase or lipase≥1.5×ULN and e) alkaline phosphatase≥2.5×ULN not directly related to the CML, x) Active and uncontrolled malignancy other than CML, xi) uncontrolled hypertension and/or diabetes, xii) active and uncontrolled infection, xiii) major surgery within two weeks or incomplete recovery from the previous surgery, xiv) congenital or acquired bleeding tendency, xv) Impaired gastrointestinal absorption, xvi) history of small bowel resection or bypass surgery, xvii) history of acute pancreatitis within 12 months or chronic pancreatitis, xviii) concomitant administration of strong irreplaceable CYP3A4 inhibitors or inducers, QT prolonging agents, or coumarin derivatives, and xix) any other uncontrolled medical conditions that would present substantial safety risks or compromise compliance with the study treatment. Among the patients enrolled in the ENESTKorea trial (11), we selected patients who achieved a CMR during the follow-up period and in whom we could evaluate the level of BCR/ABL1 fusion transcripts using ddPCR at the time of firstly achieving CMR. CMR was defined as an undetectable BCR/ABL1 transcript level by qRT-PCR (13). During the follow-up period, all patients were evaluated, and BCR/ABL1 fusion transcripts were quantified and standardized to BCR/ABL1IS by qRT-PCR performed at the central laboratory (BML, Daejeon, South Korea) every 3 months. This study used the protocol of qRT-PCR in ENESTKorea trial (11). The qRT-PCR used in this study had a sensitivity of MR4.5.
Clinical information, including patient demographics, BCR/ABL1 fusion transcript level, and adverse events (AEs), were collected through medical record reviews at each institution.
Measurement of BCR/ABL1 fusion transcript level-Quantitative RT-PCR analysis of the mRNA levels. The isolated total RNA was reverse-transcribed into first-strand cDNA using SuperScript® III First-Strand Synthesis (Invitrogen, Carlsbad, CA, USA) according to manufacturer's instruction. One μg of total RNA was included in the final reaction volume of 20 μl. The reaction mixture was incubated at 50°C for 50 minutes, then heated to 85°C for 5 minutes to stop the reaction, and was then stored at −20°C until the next step. After reverse transcription, 2 μl from the reverse transcription reaction was used as a template in each PCR reaction for the BCR/ABL1 and BCR amplification. PCR was performed in a total volume of 15 μL using the SsoAdvanced™ Universal SYBR® Green Supermix (Bio Rad, Hercules, CA, USA) and CFX384 Real-Time System thermocycler (Bio Rad). The amplification profile involved denaturation at 95°C for 30 seconds for 1 cycle and then denaturation at 95°C for 15 seconds and one step of annealing and elongation at 65°C for 30 seconds for 45 cycles. Following completion of the PCR, the amplification pattern of BCR/ABL1 and BCR was checked using a melting curve analysis. The threshold cycle number (CT) of each sample was used to determine the copy number and was compared to a corresponding standard curve generated with 7 different copy numbers (from 106 to 100 copies) for each recombinant plasmid, including the BCR or BCR/ABL1 amplified region. The primer set for BCR/ABL1 was 5’-GATGCTGACCAACTCGTGTG-3’ for the forward and 5’-AACGAAAAGGTTGGGGTCAT-3’ for the reverse. The primer set for BCR was 5’-TTCTGGACCACCTGAAAAGG-3’ for the forward and 5’-TGCTCTGTCTCTTGCTGTCC-3’ for the reverse.
Droplet generation. ddPCR was performed in a total volume of 20 μl containing 10 μl EvaGreen supermix (2×, Bio-Rad Laboratories), each primer set (final concentration of 150 nM), DNase/RNase-free sterile water, and a variable volume of diluted cDNA (40, 20, or 5 ng) to achieve a higher sensitivity and to define the threshold. Primer sequences are as follows; BCR forward primer: 5’-TTC TGG ACC ACC TGA AAA GG-3’; BCR reverse primer: 5’-TGC TCT GTC TCT TGC TGT CC-3’; BCR/ABL1 forward primer: 5’-GAT GCT GAC CAA CTC GTG TG-3’; BCR/ABL1 reverse primer: 5’-AAC GAA AAG GTT GGG GTC AT-3’. Each ddPCR mixture was loaded into each sample well of a DG8 droplet generator cartridge (Bio-Rad Laboratories), followed by the loading of 70 μl droplet generation oil for EvaGreen (Bio-Rad Laboratories) into each oil well of the DG8 cartridge. The cartridge was placed inside a QX200 droplet generator (Bio-Rad Laboratories). When droplet generation was completed, approximately 20,000 droplets were generated in each droplet well. Droplets in each droplet well were transferred to a 96-well PCR plate (Bio-Rad Laboratories) and were sealed using a PX1 PCR plate sealer (Bio-Rad Laboratories) for 5 seconds at 180°C before thermal cycling. The PCR plate was placed in a deep-well C1000 Touch thermal cycler (Bio-Rad Laboratories) for amplification. Thermal cycling conditions were: i) 5 minutes at 95°C, ii) 40 cycles of denaturation for 30 seconds at 95°C and iii) annealing/extension for 1 minute at 58°C, and three final steps iv) at 4°C for 5 minutes, v) 90°C for 5 minutes, and vi) 4°C infinite hold. All PCR steps were conducted with a change of 2°C/s. A no template control and a positive control (cDNA synthesized from K562 total RNA) were included in each assay.
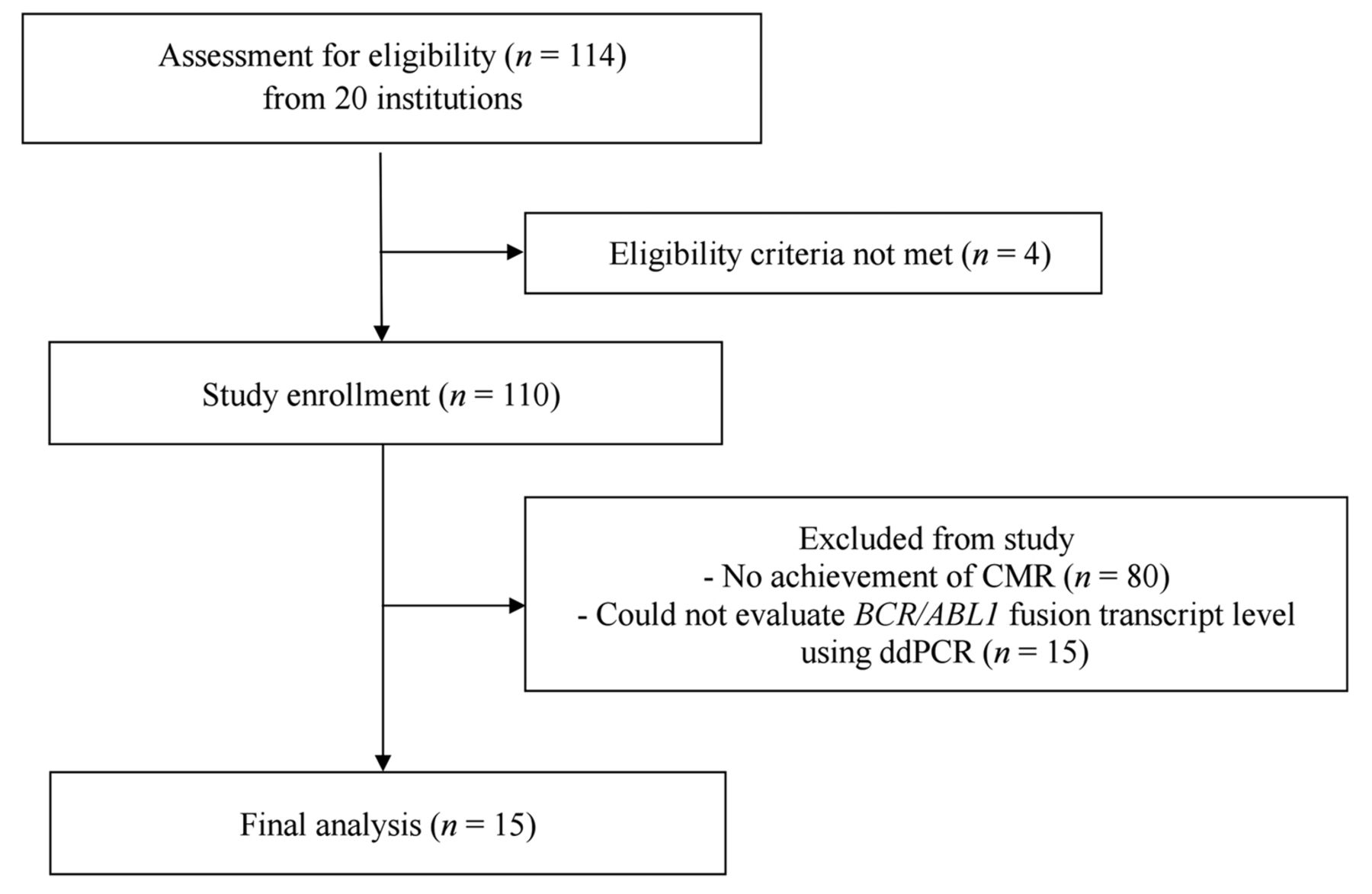
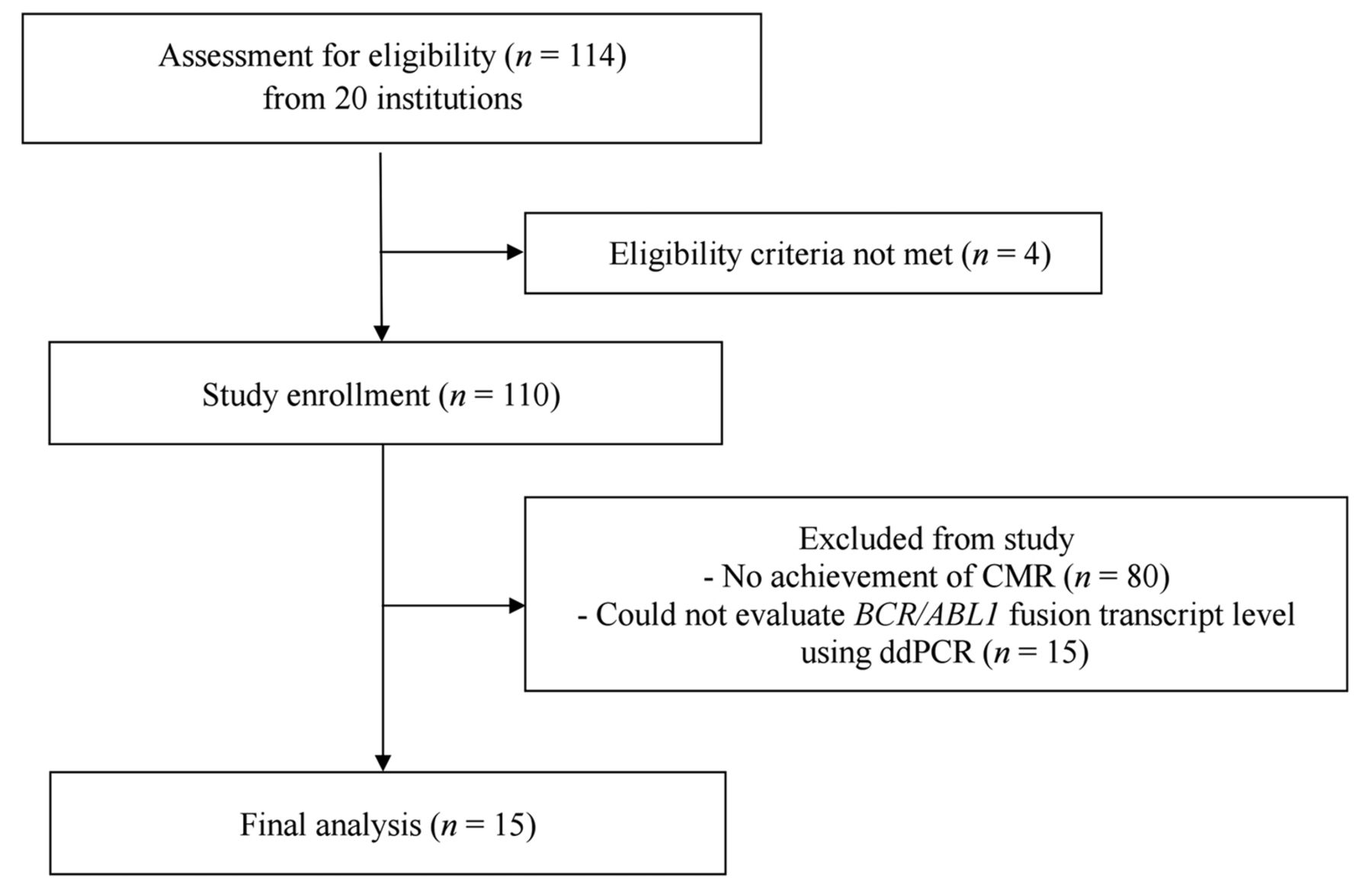
CONSORT flow diagram. CMR: Complete molecular response; ddPCR: droplet digital polymerase chain reaction.
ddPCR. Following thermal cycling, the PCR plate including the droplets was loaded onto the QX200 droplet reader (Bio-Rad Laboratories), which identified the fluorescence intensity of each droplet for EvaGreen fluorophore, using a multi-pixel photon counter. This detector reads the droplets to identify those that do (+) or do not (−) contain a target gene by plotting fluorescence droplet-by-droplet. We determined droplets to be positive ones only for samples whose fluorescence levels differed significantly from the back-ground fluorescence level. We used QuantaSoft software version 1.7.4 (Bio-Rad Laboratories) to determine the concentration of the target gene in copies/μl.
Statistical analysis. Comparisons of categorical variables were performed using Fisher's exact tests. The Kaplan-Meier method was used to analyze the period of treatment response. The duration of CMR was defined as the period of undetectable BCR/ABL1 transcript (BCR/ABL1IS=0%) by qRT-PCR. The duration of MR4.5 was defined as the period from no detection of BCR/ALB1 (i.e., the day ddPCR was performed) firstly to the loss of MR4.5 (BCR/ABL1IS=0.0032%) by qRT-PCR. The cut-off value of BCR/ALB1 transcript level was the median value (3.6 copies/20 μL) of the total level of BCR/ABL1 transcripts measured using 40, 20, or 5ng of RNA (Table II).
Ethical considerations. The study protocol was reviewed and approved by the Institutional Review Board of each of the 7 hospitals and was in accordance with principles established by the Declaration of Helsinki for biomedical research (14). Informed consent was obtained from all patients for being included in the study.
Results
Patient characteristics. Between May 2013 and November 2014, 15 patients from 7 institutions who met the inclusion criteria were enrolled in this study (Figure 1 and Table I). The median follow-up period for a total of 110 patients was 22.7 months (range=0.1-54.2 months), and for the 80 patients who did not achieve CMR, it was 22.5 months (range=0.1-37.0 months), respectively. The median follow-up period for the 15 patients who were included in this study was 47 months (range=39-61 months). All patients received nilotinib at a starting dose of 300 mg twice daily. Median patient age was 56 years (range=38-83 years). Ten (66.7%) and five (33.3%) patients were male and female, respectively.
Baseline patient characteristics (n=15).
BCR/ABL1 transcript levels using ddPCR at IS 0%.
ddPCR measurement. We measured the levels of BCR/ABL1 and BCR transcripts using ddPCR three times when CMR was firstly achieved, as verified by qRT-PCR (Table II). The median values of total BCR/ABL1 and BCR transcript levels were 3.6 copies/20 μl (range=1.2-6.8 copies/20 μl) and 15,758 copies/20 μl (range=1802-34140 copies/20 μl), respectively.
ddPCR results and treatment outcome. The median treatment and follow-up periods for the 15 patients were 45 months (range=37-55 months) and 47 months (range=39-61 months), respectively. Except for one patient who switched to imatinib 37 months after initiation of nilotinib due to a nilotinib-induced cardiovascular event, 14 patients were treated with nilotinib continuously. During the follow-up period, all patients maintained a major molecular response (BCR/ABL1IS≤0.1%). Among 15 patients, 2 patients lost CMR during the follow-up period. One patient lost CMR after sustaining it over 21.3 months, and 0.002% of BCR/ABL1 was detected by qRT-PCR. The other patient lost CMR, and 0.012% of BCR/ABL1 was detected after sustaining it for 20.5 months. However, they did not lose MMR during the last follow-up period (9 months for one patient and 8 months for the other patient after the loss of CMR).

{kind=link}
{kind=link}
Kaplan Meier graphs. (A) The duration of complete molecular response depending on BCR/ABL1 transcript level (median: 3.6 copies/20 μL) as measured by ddPCR. (B) Period of no BCR/ABL1 detection using qRT-PCR to loss of MR4.5. IS: International Scale; MR4.5: molecular response at 4.5-log reduction; ddPCR: droplet digital polymerase chain reaction; qRT-PCR: quantitative real-time polymerase chain reaction.
Tendency for loss of CMR during the follow-up period.
In subsequent analyses, we used the median value of total BCR/ABL1 transcript levels (3.6 copies/20 μl) as a cut-off value. Although patients with a high level (>3.6 copies/20 μl) of BCR/ABL1 transcripts had a tendency to lose the CMR during the follow-up period, there was no significant difference in CMR loss between patients with a low level (0/10, 0%) versus a high level (2/5, 40%) (p=0.095; Table III). CMR duration was prolonged in patients with a low level of BCR/ABL1 transcripts, as measured by ddPCR (rate of sustained CMR at 2 years: 100% for low level versus 37.5% for high level, p=0.032; Figure 2A). However, there was no significant difference between groups from the day of the first CMR to the day of MR4.5 loss (rate of sustained MR4.5 at 2 years:100% for low level versus 75.0% for high level, p=0.186; Figure 2B).
Discussion
MRD is considered very important in various cancers because a low or negative MRD after treatment is associated with a longer response duration and survival (15-17), and the achievement of a DMR predicts a better clinical outcome in CML patients (18). Due to the remarkable results of withdrawal clinical studies (i.e., STIM and TWISTER studies), the appropriate selection of patients with a “true” CMR is important for predicting the success of treatment-free remission (19, 20).
Currently, qRT-PCR is the primary method for monitoring the TKI response and MRD and for predicting early relapse (6, 21). Although qRT-PCR is relatively sensitive, it has several limitations due to its poor standardization and labor-intensiveness (22). To overcome these limitations, recent emerging technologies, such as next-generation sequencing, next-generation flow, and ddPCR, have been applied for precision medicine (23, 24). Among these, ddPCR is an advanced method with results that strongly correlate with those of qRT-PCR (25, 26). ddPCR enables the measurement of absolute copy numbers without requiring a reference standard curve (9, 10, 27). Furthermore, it can detect nucleic acids with a sensitivity exceeding 10−6 and is less influenced by inhibitory substances, non-target RNA, and nonspecific amplification (10, 27). Because of these advantages, ddPCR has been used to evaluate circulating tumor DNA, mutations, and tumor burden in cancer research (28). ddPCR has also been used to detect MRD and predict prognosis in hematologic malignancy (9, 25). Therefore, ddPCR could be an optimal alternative modality for qRT-PCR; however, disadvantages of ddPCR, including its high cost, time-intensiveness, and limited data in the clinical setting, must be solved to allow its wider use (29).
Our results indicate that ddPCR could be a sensitive tool for detecting MRD as a complement to qRT-PCR. BCR/ABL1 transcripts were detected in all patients by ddPCR even though a CMR state (BCR/ABL1IS=0%) was verified by qRT-PCR. In addition, we noted that the duration of CMR differed significantly depending on MRD, as detected by ddPCR at the time when CMR was firstly achieved. This finding suggests that a low MRD is an important factor for maintaining longer remission periods, consistent with the results of previous studies (18). However, because all our patients maintained a major molecular response during their treatment with TKIs, it is questionable whether an elevated BCR/ABL1 transcript level detected by ddPCR is clinically meaningful as a treatment failure (6). Additionally, because of the superior treatment response to nilotinib, with an approximately 80% rate of complete cytogenetic response, all patients might maintain an optimal response during the follow-up period (30). Therefore, for an evaluation of long-term outcomes, further follow-up might be needed.
Additional limitations of this study were that we could not routinely use ddPCR for response monitoring every 3 months. Because ddPCR is not yet widely commercialized, frequent use of ddPCR was limited. In addition, some patients did not show homogeneous results according to the input RNA, which is also another limitation. The standardization of the quantitative measurement of BCR/ABL1 by ddPCR has not yet been well-established. Therefore, there has been a concerted effort to obtain precise results with less false-positive droplets (e.g. using an adequate volume of cDNA) (26). Nevertheless, a previous study has shown that the false-positive rate can be 2% even when healthy donors are used (31). Therefore, further standardization and validation of the protocol are needed for a higher sensitivity of ddPCR.
Another limitation of our study was that sample size was small despite this being a multi-institution study. Therefore, a large-scale study is needed to confirm these results. Despite these limitations, to the best of our knowledge, this is the first study reporting a difference in outcomes depending on BCR/ABL1 transcript level measured by ddPCR in CML patients with a CMR state.
In conclusion, we demonstrated the sensitivity of ddPCR for detecting MRD at the time of undetectable BCR/ABL1 transcripts, as measured by qRT-PCR in CML patients. Additionally, the duration of CMR differed significantly depending on MRD at the time when the CMR was firstly achieved. Future large-scale trials and rigorous validation of the ddPCR are needed to widely use ddPCR for monitoring treatment response and for detecting MRD.
Acknowledgements
KI and SSK contributed equally to this study as corresponding authors. This work was funded by Novartis Pharmaceuticals Corporation (CAMN107AKR11T).
Footnotes
Authors' Contributions
HP, DYS, IK and SKS designed the research study. YK, JHL, KHL, DYK, HJK, JSA, JOL, SMB, JWC, SGP, SP, YJL and SYA conducted the study and collected the data. HP, DYS and IK analyzed the data. HP, DYS, IK and SKS wrote the paper. All authors read and approved the final manuscript.
This article is freely accessible online.
Conflicts of Interest
The Authors have declared that they have no conflicts of interest.
- Received July 10, 2019.
- Revision received July 21, 2019.
- Accepted July 22, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved