

Abstract
Background/Aim: In Korea, small breed dogs including Maltese, Pomeranians, and Yorkshire Terriers are most common. These small dogs are at increased risk for the development of delayed union or nonunion fractures, particularly when the fracture occurs at a site with insufficient surrounded soft tissue such as the ulna and radius. To treat failed bone fracture healing, stable fixation of the fracture and implantation of bone grafts are needed. Among the various types of bone grafts, autograft is considered to be the gold standard. However, the amount of autograft available for harvesting in small dogs is limited. In this study, we report on a novel canine cancellous allograft (C350C) that was prepared using chemicals and low heat treatment (350°C). Patients and Methods: We applied C350C in two cases with failed bone fracture healing. Due to the poor osteoinductive capabilities of C350C, we also used recombinant human bone morphogenetic protein-2 (rhBMP-2) and Matrigel as osteoinductive and delivery agents, respectively. Results: In both cases, the fractures healed successfully. Conclusion: C350C can be used as a bone graft material that could replace autografts in cases with failed bone fracture healing.
- Cancellous allograft
- structural support
- failed bone fracture healing
- dog
Bone grafting is a surgical procedure commonly used to promote bone healing and reduce complications in both veterinary and human medicine. It is indicated for use in cases with orthopedic surgeries such as highly comminuted fractures, fractures with bone loss, arthrodesis, and failed bone fracture healing (1, 2). Delayed union or nonunion is associated with failed bone fracture healing, which can be caused by fracture instability, infection, impaired blood supply to the bone and surrounding tissue, and bone loss at the fracture site (2, 3). To treat delayed union or nonunion fractures, surgery involving rigid stabilization of the fracture ends and implantation of bone graft, which is able to fill the fracture gap and stimulate bone healing, is required (2).
Bone graft material is categorized as autograft, allograft, xenograft, and alloplast. Among these, the autograft is considered the gold standard because it has osteogenic, osteoconductive, and osteoinductive properties, which are ideal for bone grafts, and its use rarely results in infection or immunological problems (3-5). However, its use can increase the number of surgical sites, resulting in prolonged anesthetic times and potential donor site morbidity. Additionally, and most importantly, the amount of available bone grafts is limited (3, 6). Thus, effort has been focused on overcoming these limitations and on developing an alternative to the autograft. In particular, the allograft has been introduced as a possible replacement for the autograft (5, 7).
An allograft is a bone graft that has been harvested from the same species. The allograft is variable in its osteoinductive and osteoconductive properties. However, it has few cells due to the process of removing cells which can cause immune responses, so its osteogenic capabilities are less than those of the autograft (3). Advantages of the allograft are that it can be obtained in large quantities and it can be used in various configurations such as massive allograft, demineralized bone matrix, morselized bone chips, and whole bone segments (1). Most importantly, the allograft is structurally similar to the host bone. By contrast, bovine and porcine bones, which are mainly used as xenografts, have different chemical compositions and bone structures when compared to the canine bone (8).
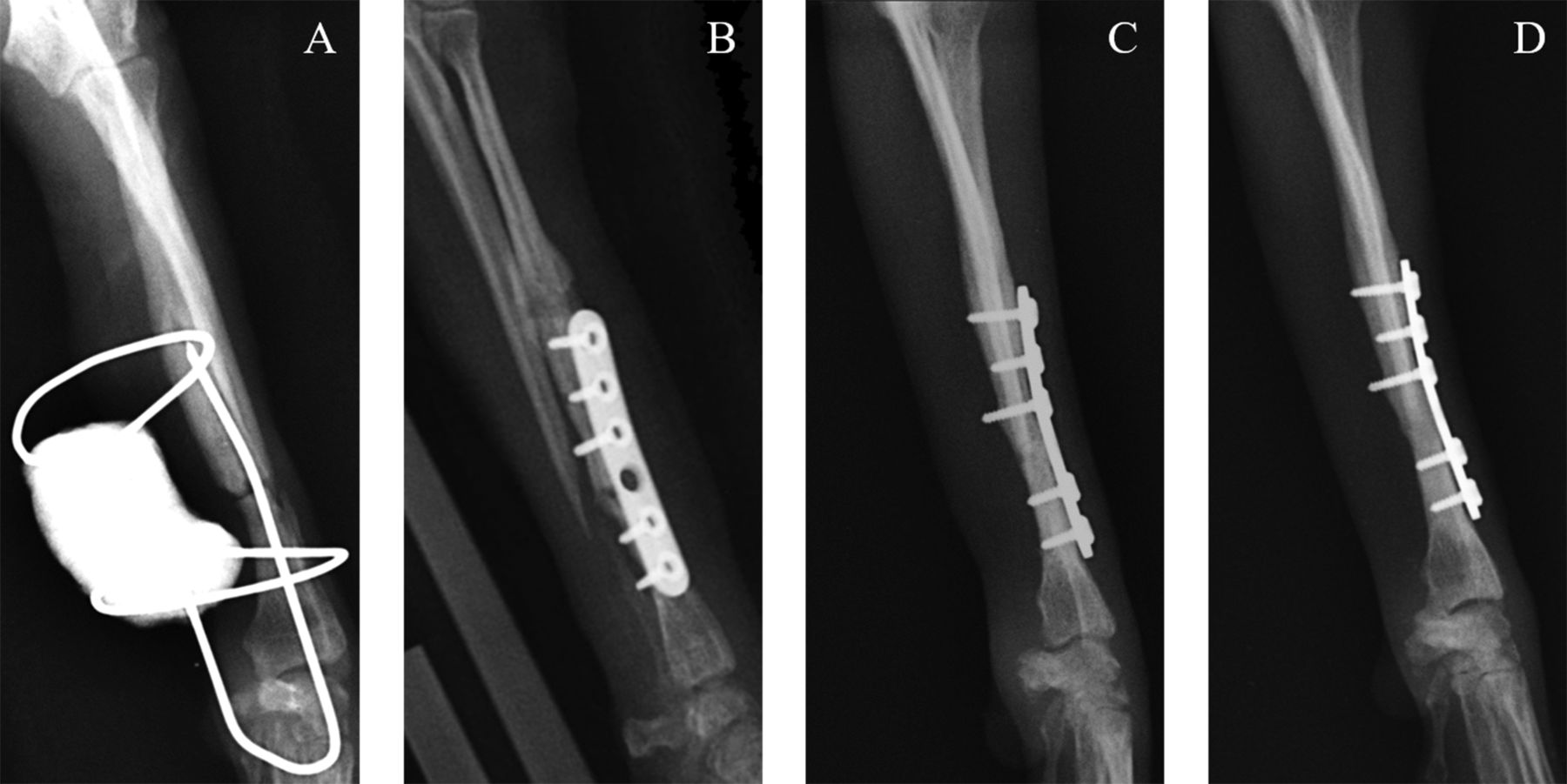
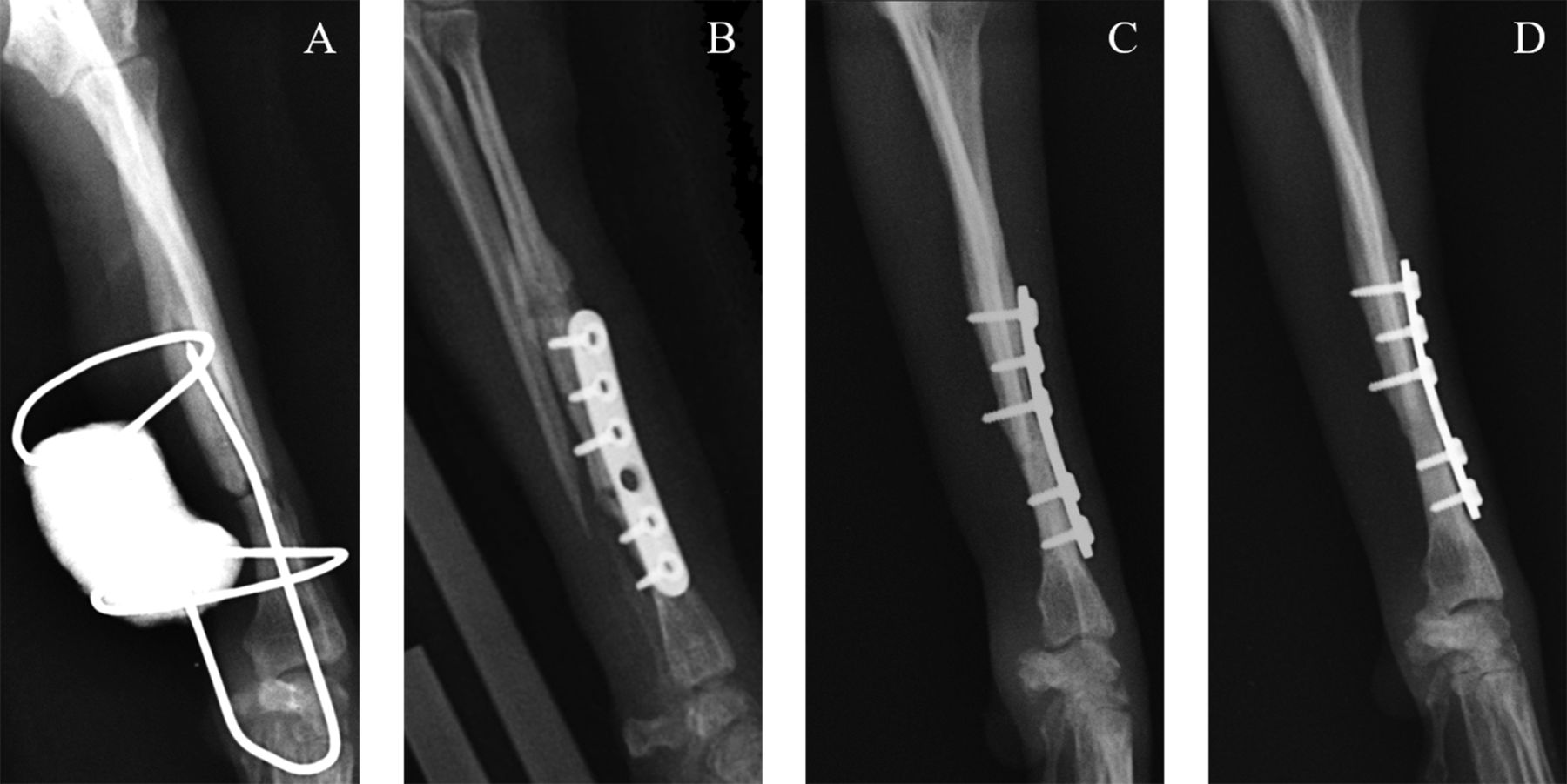
Radiographs of a 3-year-old castrated Pomeranian male with fractures of the distal third of the left radius and ulna. (A) Lateral radiograph showing a nonunion fracture of the radius and ulna prior to revision surgery. (B) Immediately postoperatively. (C) Seven weeks postoperatively. (D) Twelve weeks postoperatively.
The risks associated with the use of an allograft are disease transmission and the possible induction of an immune response. To reduce their immunogenicity, allografts are typically treated by deep-freezing at −70°C or freeze-drying. The processes of ethylene oxide gas sterilization, gamma irradiation, and electron beam irradiation are performed to eliminate infectious agents (6). However, these treatment methods do not entirely eliminate the possibility of infection, including virus (9). One study reported that ethylene oxide sterilization, irradiation, and dimethyl sulfoxide sterilization were not capable of completely destroying the human immunodeficiency virus (HIV) (10, 11). This result suggests that there is the risk of disease transmission in animals as well when using bone grafts. Also, the processing and storage methods of allografts not only reduce their mechanical strength, but affect their osteoinductive and osteoconductive capabilities (6). Using the decalcification method, which removes inorganic elements from the allograft, bone formation is fast. However, the mechanical strength of the allograft is not maintained long enough for there to be sufficient new bone formation, due to rapid biodegradation (3). Thus, allografts are typically used in orthopedic surgery in conjunction with xenograft or alloplast rather than alone.
To apply the use of allografts in orthopedic cases, we developed a canine allograft using a chemical and low heat treatment (350°C). This was expected to result in the maintenance of adequate mechanical strength for the duration of bone fracture healing period and provide a structure similar to that of the canine bone. We also evaluated the biocompatibility of the allograft. We then applied the allograft in two cases of failed bone fracture healing, resulting in delayed union in one and nonunion in the other. Because the osteoinductive properties of the allograft were nearly eliminated due to the chemical and heat treatments, we added recombinant human bone morphogenetic protein-2 (rhBMP-2) and Matrigel to our allograft as osteoinductive and delivery agents, respectively. Successful healing of the fracture was achieved in both cases, thus, herein, we report the results.
Materials and Methods
Manufacturing of canine cancellous allografts with chemical and 350°C heat treatment (C350C). Cancellous bone obtained from the femurs of cadaver beagles was used in the manufacturing of C350C. Cadavers of healthy beagle dogs were provided by the Korean Institute of Toxicology (Daejeon, Republic of Korea). The femur bones were harvested, and then all surrounding soft tissue and cartilage were surgically removed. Blocks measuring less than 2 cm were created from the cancellous bone and were cleaned with distilled water. The blocks were boiled for 24 h in distilled water, defatted with toluene in a Soxhlet extractor for 72 h, and finally deproteinized with 95% ethylenediamine for 50 h twice. Each deproteinization procedure was followed by a washing procedure. The first washing procedure lasted 6 days at a rate of 0.5-1.5 l/h, the second washing procedure lasted 17 days at the same flow rate. Then, the samples were heated at 350°C in a muffle furnace (MF-21G, Jeio Tech, Daejeon, Republic of Korea) for 20 h, and finally, grounded into particles of 350-1000 μm using a grinder (MM400, Retsch, Haan, Germany).
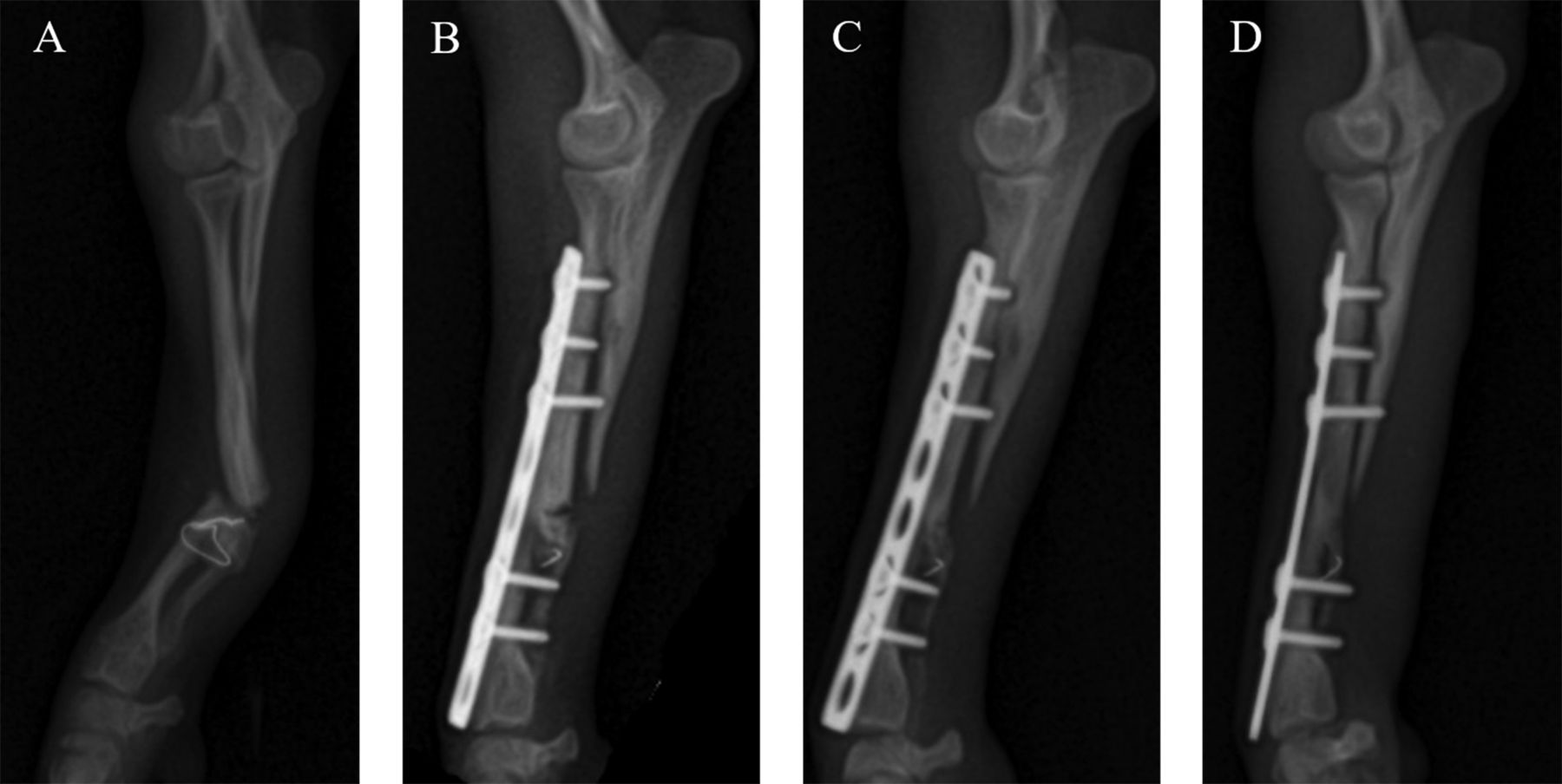
Radiographs of a 1-year-old Pomeranian male with fractures of the distal third of the left radius and ulna. (A) Lateral radiograph showing a delayed union fracture of the radius and ulna prior to revision surgery. (B) Two weeks postoperatively. (C) Seven weeks postoperatively. (D) Twelve weeks postoperatively.
Evaluation of the biocompatibility of C350C. The C350C particles were analyzed and their morphological features were assessed using a scanning electron microscope (SEM) (Hitachi, S-4300, Tokyo, Japan) with a 15.0 kV accelerating voltage and a working distance of 10.5 mm. The samples were gold sputter-coated to render them electrically conductive before examination. To evaluate the cytotoxicity of C350C, a Cell Counting Kit-8 (CCK-8; Dojindo molecular technologies Inc., Rockville, MD, USA) test was performed according to the manufacturer's instructions. Purified L929 cells (Murine fibroblast cell line) from KOREAN CELL LINE BANK (KCBL, Seoul, Republic of Korea) were seeded at a density of 5×103/well on a 96-well plate. The cells were grown in Dulbecco's modified eagle medium (DMEM), supplemented with 10% fetal bovine serum (FBS) and 1% penicillin-streptomycin for 24 h at 37°C in a 5% CO2 incubator. The culture medium was then removed, and the cells were treated with a leaching solution for 24 h. The leaching solution was prepared from 1 ml of DMEM supplemented with 10% FBS, and 0.2 g of C350C or Bio-Oss®, a commercialized xenograft, was soaked for 24 h at 37°C. The culture medium with or without the addition of 1% Triton X-100 detergent was used as a control. The CCK-8 solution was diluted with DMEM at a ratio of 1:9 and incubated at 37°C for 120 min. Absorbance was measured at 450 nm.
Case 1. A 3-year-old, 3.4 kg, castrated Pomeranian male presented with a nonunion fracture to Chonnam National University - Veterinary Medical Teaching Hospital (CNU-VMTH). The fracture site was located at the distal one-third of the left radius and ulna. The fractured bones had been stabilized twice before using external skeletal fixation (ESF) at a local animal hospital. Unfortunately, the fracture failed to heal. Nonunion of the radius with a marked fracture gap was observed in radiographs, and resorption of the distal aspect of the ulna was evident (Figure 1A). Therefore, re-operation using C350C was planned for the nonunion site. A mixture of rhBMP-2 (PeproTech, Rocky Hill, HJ, USA) and Matrigel (BD Korea, Seoul, Republic of Korea), was also applied to the fracture gap in conjunction with C350C.
Preoperatively, the patient received 5 mg/kg cimetidine (H-2®AMP; JW Pharmaceutical, Seoul, Korea) and 20 mg/kg cefazolin (Cefazolin CKD INJ 1 g; Chong Kun Dang Pharm, Seoul, Republic of Korea) intravenously. The patient was premedicated with 0.005 mg/kg glycopyrrolate (Glycopyrrolate Reyon AMP 1 ml; Reyon Pharm, Seoul, Republic of Korea), 0.3 mg/kg butorphanol (Butophan INJ 1 mg/ml; Myungmoon Pharm, Seoul, Republic of Korea) and 0.3 mg/kg midazolam (Vascam INJ 5 mg/ml; Hana Pharm, Seoul, Republic of Korea) by intravenous injection. Anesthesia was induced intravenously using 1.5 mg/kg etomidate (Etomidate-Lipuro INJ; Hanall Biopharma, Seoul, Republic of Korea). General anesthesia was maintained with 1.5% isoflurane (Forane®; JW Pharmaceutical, Seoul, Republic of Korea) in 100% oxygen administered via an endotracheal tube.
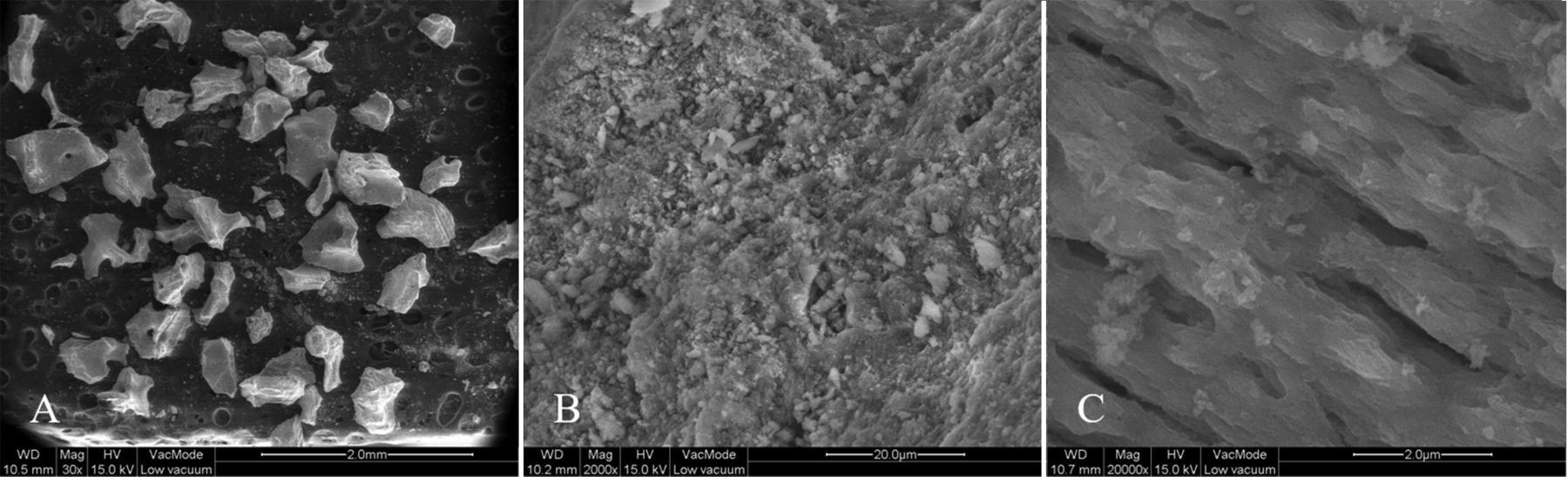
SEM images of the surface of C350C. (A) Original magnification 30×, various particle sizes are shown. (B) Original magnification 2,000×, the surface of C350C is rough. (C) Original magnification 20000×, the interconnected porous surfaces are shown.
A craniolateral approach to the left radius was used to expose the fracture site. The fracture ends were cleaned and trimmed with a bone file. Then the fracture was fixed with a 2.0 bone plate and screw system. Finally, the fracture gap was filled with C350C and 200 μl of Matrigel containing 60 μg of rhBMP-2.
Postoperatively, 10 mg/kg clindamycin (Fullgram® CAP; Samjin Pharm, Seoul, Republic of Korea) and 5 mg/kg enrofloxacin (Baytril® 50 mg; Bayer Korea, Seoul, Republic of Korea) were administered orally twice daily for 7 days. In addition, 5 mg/kg firocoxib (Previcox® 227 mg; Merial Limited, Duluth, GA, USA) was administered orally once daily for 7 days. A splint was applied postoperatively to support the fracture repair and was maintained for 4 weeks.
Case 2, A 1-year-old, 5.6 kg, Pomeranian male was referred to CNU-VMTH for management of a delayed union fracture. As in case 1, the fracture site involved the distal third of the left radius and ulna. The fractured bones had been stabilized using ESF at a local animal hospital 12 weeks prior. However, the fracture did not heal completely, and re-fracture occurred following removal of the ESF. Transverse fractures of the radius and ulna were identified on follow-up radiographs. A wire that had been used in the previous fracture repair was observed on the radiographs, and the bone density surrounding the wire appeared decreased (Figure 2A). Therefore, re-operation using C350C was planned to promote fracture healing.
Surgical preparation and the anesthetic protocol used were the same as in case 1. A craniolateral approach to the left radius was used to expose the fracture site. The residual wire was removed and the fracture ends were cleaned and trimmed with a bone file. The debris was removed, and the fracture was stabilized with a 2.0 bone plate and screw system. Finally, the fracture gap was filled with a combination of C350C and 200 μl of Matrigel containing 60 μg of rhBMP-2.
Results
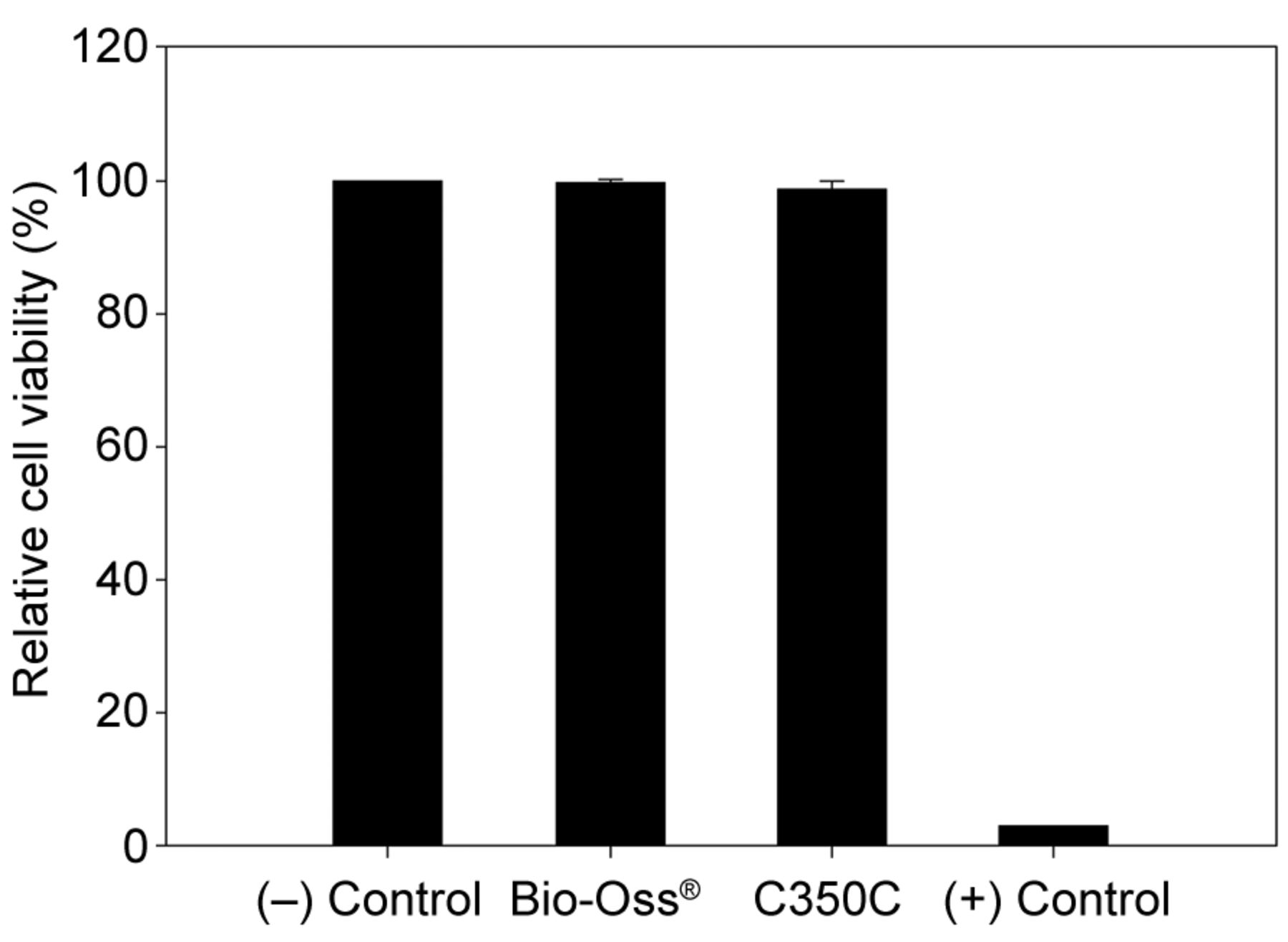
Evaluation of the biocompatibility of C350C. SEM images of C350C revealed that the bone graft material included a variety of particle sizes (Figure 3A). The surface of C350C appeared rough (Figure 3B) with an interconnected porous structure (Figure 3C). The relative cell viability of C350C was 98.68%, compared to the negative control group value of 100%. No significant difference was discovered between the relative cell viability of C350C and that of Bio-Oss® (99.59%) (Figure 4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Cell viability was assayed by CCK-8 assay in L929 cells. Cell viability was high with C350C (98.68%) and was not significantly different from the negative control (100%) or from Bio-Oss® (99.59%).
Case 1. Follow-up radiography was performed 7 and 12 weeks postoperatively (Figure 1B). Radiographic union between the radial bone fragments and the proximal fragment of the ulna was evident by 7 weeks postoperatively (Figure 1C). The fracture lines were no longer evident, indicating complete healing of fracture, on the 12-week postoperative radiographs (Figure 1D).
Case 2. Follow-up radiography was performed 2, 7, and 12 weeks postoperatively. At the second week recheck, radiolucent lines between the radial bone fragment remained, and there was evidence of a bridging callus between the proximal radial fragment and the distal ulnar fragment. A wire remnant was present in the ulna, which we had been unable to remove at the time of surgery (Figure 2B). At the 7-week recheck, narrowing of the fracture gap was evident (Figure 2C). By 12 weeks postoperatively, the proximal and distal radial bone fragments had united completely with the distal ulnar fragment (Figure 2D). The patient was free of lameness and pain.
Discussion
An allograft is a type of bone graft created with the intent of overcoming the limitations of the autograft. Although the osteogenic potential of the allograft is eliminated during processing, its osteoinductive and osteoconductive properties remain (9). Most commercial allografts available are treated by deep-freezing at −70°C or freeze-drying to reduce the immune response and extend the storage period. However, the mechanical strength of bone grafts treated with these methods can be reduced, making them more vulnerable to external forces in orthopedic surgeries (6). Thus, we developed canine allografts using chemical and heat treatments with the goal of achieving increased structural support in orthopedic surgeries.
The most common heat treatments for bone grafts are performed for several hours at temperatures above 1,000°C. However, grafts treated in such a way risk losing their microporosity, and therefore, their osteoconductive capacities may be reduced (8). In a previous study, we compared the characteristics of porcine bone grafts that had been heat treated at 400°C and 1,200°C (12). When the heat treatment was performed at the low temperature of 400°C, the crystallinity of the graft was lower than that observed at 1,200°C. Low crystallinity has some advantages over high crystallinity; larger surface area of bone graft, rapid absorption by osteoclasts, and more suitable conditions for bone remodeling (12, 13).
With heat-treatments above 600°C, all organic compounds capable of causing an immune response are removed from the graft (8). So, in this study, we defatted and deproteinized the C350C with chemicals intended to eliminate the organic compounds that could not be removed by the low heat treatment at 350°C.
In this study, the SEM and CCK-8 assays were performed to evaluate the biocompatibility of C350C. The SEM images showed that the C350C consisted of various particle sizes and an interconnected porous surface. Macroporosity is essential for vascularization, and microporosity affects bone remodeling with the graft itself (9). Thus, porosity can be one of the most critical factors associated with bone grafting, and the SEM results suggested that C350C had the potential to be a superior bone graft.
The CCK-8 assay was performed to assess cytotoxicity, and revealed none associated with C350C. Thus, we applied it in actual clinical cases with delayed or nonunion failure. In the first case, fracture healing had failed twice at the local animal hospital. Instead of an autograft, C350C was used because the dog was too small to allow harvesting of a sufficient quantity of graft material to fill the fracture gap. Follow-up radiographs showed complete union of the bone fragments 12 weeks postoperatively. In the second case, the delayed union fracture was repaired using the same surgical procedure and a combination of graft materials. By 12 weeks postoperatively, the fracture had healed, and normal function of the limb had been restored.
The treatment of failed fracture healing, particularly in cases of nonunion or delayed union, should satisfy the biological and mechanical requirements of fracture healing. The two major mechanical factors encountered during fracture healing are the stability of the fixation and the quality of the fracture reduction (14). In the cases in this study, surgical treatment included trimming the ends of the fractured bone fragments and provision of stable fixation using plate and screw system. The fragment gap was also filled with C350C, a novel allograft material. The osteoinductive properties of C350C were lost during the chemical and heat treatment, therefore, rhBMP-2 and Matrigel were added as osteoinduction and delivery agents, respectively. The rhBMP-2 has potent osteoinductive capabilities in animals and humans, inducing chondrogenesis, osteogenesis, and angiogenesis and regulation of extracellular matrix synthesis (15). Milovancev et al. (2007) (16) reported that the use of rhBMP-2 stimulated bone formation at delayed union or nonunion fracture sites without any adverse effects, resulting in an excellent outcome in four dogs.
Matrigel is a soluble and sterile extract of basement membrane proteins from the Engelbreth Holm-Swarm (EHS) tumor. It possesses several growth factors including transforming growth factor-ß, fibroblast growth factor, epidermal growth factor, platelet-derived growth factor, and insulin-like growth factor, all resulting in the promotion of cell differentiation and bone formation. It becomes a gel at the temperature of 37°C due to its thermoplastic properties (17). In a previous study, we demonstrated that Matrigel supported new bone formation in a rat calvarial defect model without any complications (18). In another study, we treated nonunion fractures using a cancellous autograft combined with 100 μl of Matrigel containing 20 μg rhBMP-2 and found that fracture healing was enhanced (19).
In the present study, both the in vitro and in vivo results suggest that C350C could be a safe and stable allograft for use in cases with failed bone fracture healing. Additionally, bone regeneration could be enhanced using a combination of rhBMP-2 and Matrigel with C350C.
Acknowledgements
This study was supported by a grant of the Next-Generation BioGreen 21 Program (no. PJ01135201) and the Rural Development Administration and Industrial Technology Innovation Program (no. 10048358) funded by the Ministry of Trade, Industry, & Energy (MI, Korea), Republic of Korea.
Footnotes
Authors' Contributions
Kil Jun Jeong and Seong Soo Kang designed the study conception. Kwangsik Jang collected the data. Kil Jun Jeong and Euisin Yang analyzed the data and wrote the manuscript. Kyung Mi Shim, Chun-Sik Bae and Se Eun Kim critically revised the manuscript for important intellectual content. Se Eun Kim and Seong Soo Kang supervised the study. All Authors read and approved the final version of the manuscript.
This article is freely accessible online.
Conflicts of Interest
The Authors have no conflicts of interest to declare regarding this study.
- Received August 14, 2019.
- Revision received September 15, 2019.
- Accepted September 16, 2019.
- Copyright© 2019, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved