

Abstract
A patient treated for 4 months with hydroxycarbamide (hydroxyurea) for chronic myelomonocytic leukemia was admitted to hospital for recently developed severe dyspnea and acute respiratory failure. The computed tomographic scan of the chest showed diffuse ground glass opacities, some centrilobular low-density nodules (resembling hypersensitivity pneumonitis-like pattern), and minimal interstitial reticulation of the subpleural region. The analysis of bronchoalveolar lavage fluid excluded infection, as did serological examinations. The patient was started on oxygen therapy and with relief of thrombocytopenia and suspected hemolytic anemia, hydroxyurea treatment was discontinued. The patient underwent steroid therapy, with a rapid progressive improvement of clinical and radiological features. As hydroxyurea is increasingly used for a number of systemic disorders, physicians must be aware of its potential lung toxicity, requiring immediate cessation of the treatment and empiric corticosteroid therapy.
- Hydroxycarbamide
- hydroxyurea
- lung toxicity
- interstitial pneumonitis
- case report
Hydroxycarbamide (hydroxyurea) is a drug widely indicated for the treatment of myeloproliferative disorders (chronic myeloid leukemia) and sickle cell anemia (1-3). As a rule, this antineoplastic drug is well tolerated (1), and is commonly used for ovarian neoplasms, squamous cancer of the head and neck, and glioblastoma multiforme. The most common toxic effects include hematological alterations associated with bone marrow failure and T-cell reduction, thrombocytopenia, anemia and neutropenia (1-3). Other common side-effects (10% or more) include asthenia, azoospermia, malaise, dysuria, blood creatinine increase, disorientation, hallucination, fever, gastrointestinal disorders (such as pancreatitis, nausea, vomiting, diarrhea, stomatitis, mucositis, dyspepsia, melena), and dermatological lesions (vasculitis, alopecia, popular rush, skin atrophy and exfoliation or ulcers) (1-3). In 1-10% of cases, the drug can lead to hepatotoxicity, hepatitis and neuropathy. Potential carcinogenic effects include an increased risk of skin cancer. Hydroxycarbamide can induce lung toxicity with pulmonary edema, lung infiltration and dyspnea (4-8), and pulmonary fibrosis in a minority of patients (5). Herein we report the clinical history of a patient experiencing acute interstitial lung injury secondary to hydroxyurea administration.
Case Report
An 83-year-old man was admitted to our hospital for acute respiratory distress. The patient was a former smoker with only 5 pack/years of exposition. The patient's past clinical history revealed systemic arterial hypertension, treated with calcium channel blockers. Twenty years earlier he had undergone surgery for an abdominal liposarcoma and during the previous 4 months had started hydroxyurea treatment (500 mg/day), following the diagnosis of chronic idiopathic myelofibrosis. The patient complained of breathlessness and a dry cough, which had worsened over the previous week. He was afebrile, the arterial blood gas analysis revealed severe hypoxemia and routine blood tests showed thrombocytopenia (63,000×106/l). The electrocardiogram was normal and echocardiography excluded acute heart failure. The serological microbiological assays revealed an uncertain positivity for Mycoplasma pneumonia, while blood cultures were negative. Chest examination revealed bilateral basal crackles and the chest X-ray showed bilateral diffuse shadows. The computed tomographic (CT) scan of the chest excluded pulmonary embolism and showed ground glass opacities with mosaicism in both lungs. In the upper lobes, small ground-glass zones were observed. Some centrilobular low density nodules resembling a hypersensitivity pneumonitis-like pattern and minimal interstitial reticulation of the subpleural regions were observed, especially in the dorsal parts of lower lobes. Some mediastinal and hilar lymphadenopathies were also present without pleural or pericardial effusions (Figure 1). The patient was started on oxygen therapy and intravenous broad-spectrum antibiotics. Bonchoscopy with bronchoalveolar lavage was performed. Microscopy and cultures for mycobacteria, common bacteria, viruses and fungi were negative. Polymerase chain reaction for Legionella pneumophila, Chlamydia pneumoniae and Mycoplasma pneumoniae, Herpes simplex virus (HSV) 1 and 2, Adenovirus and Pneumocystis jiroveci were also negative, as well as galactomannan and aspergillus antigen tests. The cytological examination and transbronchial needle aspiration of the right hilar lymph nodes (station 11 R) excluded malignant abnormalities. The cellular count in bronchoalveolar lavage revealed 40% macrophages, 55% lymphocytes (with a normal CD4/CD8 ratio), and 5% neutrophils.

{kind=link}
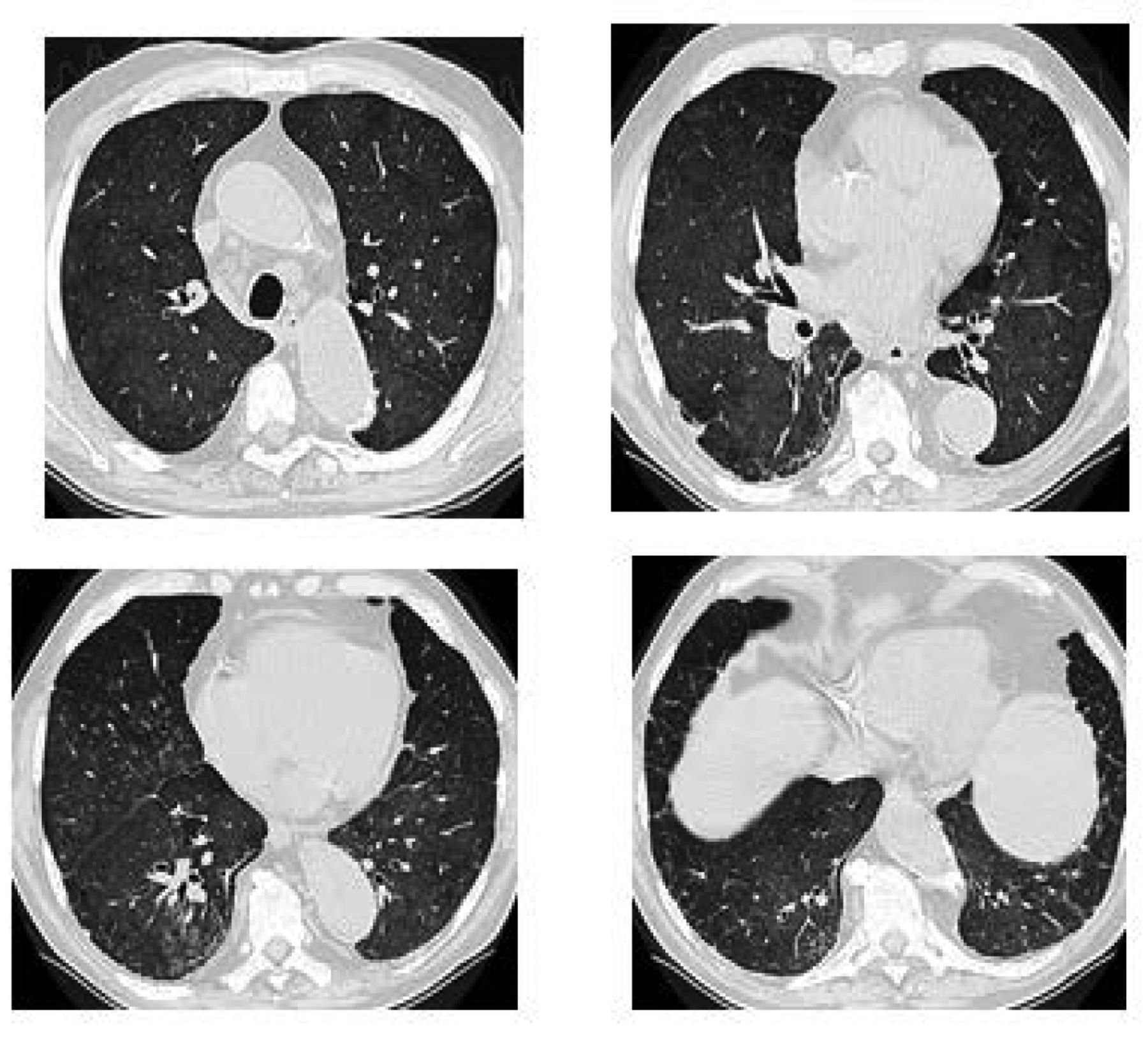
High-resolution computed tomography of the chest showing diffuse ground-glass opacities (a), bilateral peripheral reticulations (b), areas of subpleural thickening (c), and bilateral centrilobular low-density nodules (d).
With the relief of thrombocytopenia and suspected hemolytic anemia, in accordance with hematologists, hydroxyurea treatment was discontinued. A diagnosis of interstitial pneumonia associated with acute respiratory failure was made and we treated the patient with oxygen, low dose of diuretics, oral azithromycin and low dose of oral steroids (16 mg/day prednisolone). A month later the patient was referred to the pulmonologist for examination. Lung function tests evidenced a mild obstructive syndrome with a moderate-to-severe reduction of diffusion capacity for carbon monoxide. The results of arterial blood gas analysis with 2 l/min of O2 were: paO2=69.9 mmHg, paCO2=28.9 mmHg, and pH of 7.45. After 4 weeks, the abnormal chest radiography and CT findings had improved, therefore it was decided to increase the amount of prednisolone to 50 mg/day. Further improvements of the pulmonary situation were recorded after 3 months and adequate oxygenation became possible with 1.5 l/min of O2. The hydroxyurea treatment was not reintroduced and the patient is stable, his respiratory symptoms are improved as well as the lung function test parameters and the blood gas analysis. He requires oxygen only under effort.
Discussion
This case report underlines the risk of lung fibrotic toxicity in patients treated with hydroxyurea for a myeloproliferative disease. This is a rare event and very few cases have been reported in the literature (5-12). In this limited population, the interstitial lung toxicity generally occurred after a few weeks of exposure to hydroxyurea (9), while in our patient after 15 weeks. Lung toxicity is usually associated with dyspnea and fever (5-7). Fever may be the only sign of a drug reaction, resolving with withdrawal and recurring at re-challenge (4). As previously found by Cleverley et al. (13) in a similar case, fever was absent in our patient while dyspnea was severe, the lung toxicity was mainly documented by CT scan alterations and discontinuing hydroxyurea resulted in the improvement of clinical and radiological conditions. However, hydroxyurea-induced pneumonia was reported as being lethal in a recent case report in which steroids were also used at high dose with no benefit; the disease diagnosis was confirmed after autopsy and by a drug lymphocyte stimulation test positive for hydroxyurea (11).
As suggested by Rossi et al. (8) and others (11-13), the identification of ground-glass opacities at high resolution CT scan of the chest in a patient with acute respiratory symptoms treated with hydroxyurea requires a complex differential diagnosis with bacterial or viral pneumonitis, respiratory infections (aggravated by myelosuppressive therapy), and pulmonary hypertension. In our patient, the microbiological examinations allowed for exclusion of infections and the radiological high-resolution CT features were consistent with the phenomenon of drug-induced lung toxicity being similar to an hypersensitivity pneumonitis-like pattern and comparable to a histological picture of diffuse alveolar damage, already reported in Pneumotox associated with hydroxyurea exposure (14).
Mechanisms of hydroxyurea toxicity are unclear and further research is needed (15-17). This drug is increasingly used for a number of malignant and non-malignant disorders, however, as underlined by this case report, it can induce severe interstitial pneumonitis with diffuse alveolar damage and radiological pulmonary infiltrates requiring an early cessation of the treatment and empiric corticosteroid therapy (17). It is necessary that hematologists and physicians are aware of the lung toxicity of hydroxyurea and its severe and potentially life-threatening effects.
Footnotes
This article is freely accessible online.
Conflicts of Interest
All the Authors declare that they have no conflict of interest related with this topic of research.
- Received August 16, 2017.
- Revision received September 8, 2017.
- Accepted September 14, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved