

Abstract
Background/Aim: Breast cancer survivors in adjuvant therapy, frequently experience the estrogen deficiency with genitourinary symptoms mostly represented by recurrent bacterial cystitis. The objective of the present study was to evaluate the effectiveness of N-acetylcysteine, D-mannose and Morinda citrifolia fruit extract (NDM), when associated to antibiotic therapy, in reducing the persistence of recurrent cystitis in this risk population. Patients and Methods: Sixty breast cancer survived women with recurrent cystitis were retrospectively examined. Group 1, comprised of 40 patients treated with antibiotic therapy associated with NDM lasting for six months, Group 2 comprised of 20 patients treated with antibiotics alone. Results: The use of NDM in combination with antibiotic therapy showed a significant reduction in positive urine cultures, compared to antibiotics alone. Subjects of Group 1 rather than those of Group 2, showed improvement in symptoms score of urgency, frequency, urge incontinence, recurrent cystitis, bladder and urethral pain. Conclusion: In breast cancer survived women affected by genitourinary discomfort, the combination of NDM and antibiotic therapy showed a greater efficacy in reducing urinary tract infections and urinary discomfort with respect to antibiotic use only.
- Breast cancer
- cystitis
- vaginal atrophy
- N-acetylcysteine
- D-mannose
Every day worldwide women are diagnosed with malignant breast cancer with aggressiveness related to the age of patients (1). Today life expectancy of breast cancer patients is very high, but is often affected by the long-term side effects of oncological treatments. Breast tumors are often hormone-sensitive, and among the therapeutic options, endocrine therapy is currently used and includes tamoxifen, aromatase inhibitors and LHRH analogues (2). The decreased level of circulating estrogens due to the above-mentioned therapy, in addition to the menopause condition, are responsible for atrophic vaginitis and urinary disorders. The latter are characterized by symptoms ranging from moderate to severe. Today an increasing interest on patient's quality of life is taken by physicians, especially medical oncologists, by focusing both on the most effective treatment and on minimizing the treatments' side-effects, including those of uro-gynecological nature. Estrogen deficiency due to the oncological treatments, chemotherapy and endocrine therapy, induces the uro-genital syndrome as much as is the case of postmenopausal women. The genitourinary postmenopausal syndrome is defined as a set of signs and symptoms associated with the reduction of circulating estrogens that determines changes in the vagina, vulva, bladder and urethra and that severely impairs women's quality of life.
Women with breast cancer in endocrine adjuvant treatment, if not yet in physiological menopause, experience a temporary estrogen deficiency induced by the treatment itself. Similarly, to the aggressiveness of the tumor, the symptoms and signs of uro-genital syndrome may be more debilitating the younger the women are (3). The uro-genital symptoms of estrogen deficiency are vaginal dryness, burning and irritation, sexual symptoms such as the lack of lubrication and dyspareunia and urinary symptoms such as urgency, frequency, incontinence and recurrent urinary tract infections. The genitourinary syndrome, that is accompanied by atrophy of the urological mucosa, is characterized by recurrent bacterial cystitis and post-coital cystitis mostly incurred from gram-negative bacteria (4). The most bothersome urinary symptoms associated with bacteriuria are urgency, increasing voiding frequency, pain and urinary incontinence. Bacteria that colonize the bladder are mostly gram negative and of intestinal origin. They have a specific pathogenesis activity underlying the chronicity of the phenomenon which hardly allows conventional antibiotic therapies to be effective acute and chronically. Usually the time interval between an infection and is within three to six months after the initial infection.
The uropathogenic bacteria in patients affected by estrogen deficiency syndrome are usually Enterobacteriaceae (Escherichia coli, Klebsiella, Shigella, Pseudomonas) and they are able to generate biofilms, a complex of mucopolysaccharide matrix created by bacterial secretions which represent a strategic and effective weapon of defense against antibiotics and immune defenses. Inside the bacterial biofilm, frequently of polymicrobial nature (bacterial and fungal), the microorganisms are protected from the immune system cells and from the action of antibiotics, which are unlikely to penetrate the urothelium deeper layers (5). The persistence of bacteria within the biofilm favors the onset of phenomena of both genetic and phenotypical resistance to antibiotics, caused by a metabolic slowdown that allows the development of multi-resistant quiescent cells, called persistent cells. Even if in quiescent status, the persistent cells are always able to be reactivated, if necessary, by developing a new infection locally or at distant sites from the biofilm source as well (6).
Recently, this theory has allowed us to change our therapeutic approach to cure these women affected by estrogen deficiency with recurrent bacterial cystitis. In order to minimize the chronicity of an infection and improving the efficacy of antibiotics, the current prophylaxis in uroginecology has been previously demonstrated by urodynamic and is based on D-mannose, N-acetylcysteine (NAC) and Morinda citrifolia fruit extract (NDM) with antibacterial, anti-inflammatory, analgesic and immunomodulatory activity (7). D-Mannose has a binding affinity to the E. coli surface adhesins in order to reduce the adhesion between the bacteria and urothelium (8, 9). NAC has the ability to disrupt the pathogen polymicrobial biofilm and Morinda citrifolia fruit extract is a natural strong anti-inflammatory, immunostimulating, antimicrobial and cancer chemopreventive phytotherapeutic product (7, 10-12). In particular, literature has shown an increase in the efficacy of phosphomycin, nitrofurantoin or quinolones when associated with NAC in disrupting biofilm and reducing the number of vital bacterial forms, respectively, against Staphylococcus aureus, Escherichia coli and Pseudomonaceae. These last findings support the therapeutic perspective of the association antibiotics/NAC, opening new and important therapeutic solutions in chronic infectious diseases of the respiratory and urinary tract, both supported by forming biofilm microorganisms (13-15).
Even if there is no discussion on the efficacy of antibiotics in terms of bactericidal activity, we believe that in this population of patients it is possible to increase the therapeutic efficacy of the antibiotic alone by adding the effect of NAC and D-Mannose.
Objectives of this study are represented by two end-points: i) to verify if a product containing NAC, D-Mannose and Morinda citrifolia added to antibiotics therapy was able to eliminate both bacterial urinary infection with no recurrent cystitis episodes within six months from the first visit, and ii) to reduce urinary discomfort such as urgency, increasing voiding frequency, bladder and urethral pain and urinary incontinence in cancer patients.
Patients and Methods
This observational retrospective clinical study was conducted on 60 patients with recurrent cystitis, both in physiological menopause and in childbearing age affected by breast cancer. All patients observed in this study were submitted to a uro-gynecological visit, since they complained uro-genital discomfort, in the period between March 2015 and January 2017. A total of 58 of the 60 patients were in adjuvant hormonal treatment. The 60 patients observed were divided into two groups. Group 1 included 40 patients treated with D-mannose 500 mg, N-acetylcysteine 100 mg and Morinda citrifolia fruit extract 200 mg (NDM) for two months with the following regimen: NDM 1 vial every 12 h after emptying the bladder for 60 days and then 1 vial every 24 h after emptying the bladder for 4 months, associated with variable antibiotic therapy, depending on microbial sensitivity. The antibiotics used were fosfomycin, a sachet of 3 grams per day for two days, to be repeated every 15 days for a total of three cycles, nitrofurantoin 1cprs 100 mg three time a day for 6 days and ciprofloxacin 1,000 RM or prulifloxacin 600 mg 1 cps/day for 6 days.
The group 2 included 20 patients treated only with antibiotic therapy following the treatment regimens described for group 1.
All patients went at the first visit (before treatment), and repeated the visit at 2 months. After six months from first visit only patients from group 1 and those of group 2 with negative urine cultures at second visit were evaluated to measure symptoms' intensity and urine culture. At a second visit all patients had repeated urine cultures at least 10 days after the last intake of antibiotics to verify appropriate and rapid bacterial killing effect. All women were asked to report their symptoms intensity through a verbal rating scale (VRS) created specifically to explore the following 5 urological domains: urge incontinence, urgency, voiding frequency, episodes of recurrent cystitis, bladder and urethral pain The symptomatology related to each domain was measured at every visit associating a degree of intensity to the symptoms ranked from 0 (absence of symptoms) to 4 (severe symptom), depending on the discomfort felt by the patient (Figure 1).
Results
Only 10 of the 60 patients were not in menopause at the time of diagnosis. Among the patients enrolled in the study 28/60 (46.6%) were in treatment with aromatase inhibitors, 20/60 (33.3%) with tamoxifen therapy, 10/60 (16.6%) with tamoxifen and LHRH analogue, 2/60 (3.3%) with an aromatase inhibitor and tamoxifen, and 2/60 (3.3%) did not assume any adjuvant therapy (Table I). All patients subjected to a first visit had a history of recurrent cystitis and showed positive urine cultures with bacterial prevalence of Escherichia coli and Klebsiella (Figure 2).
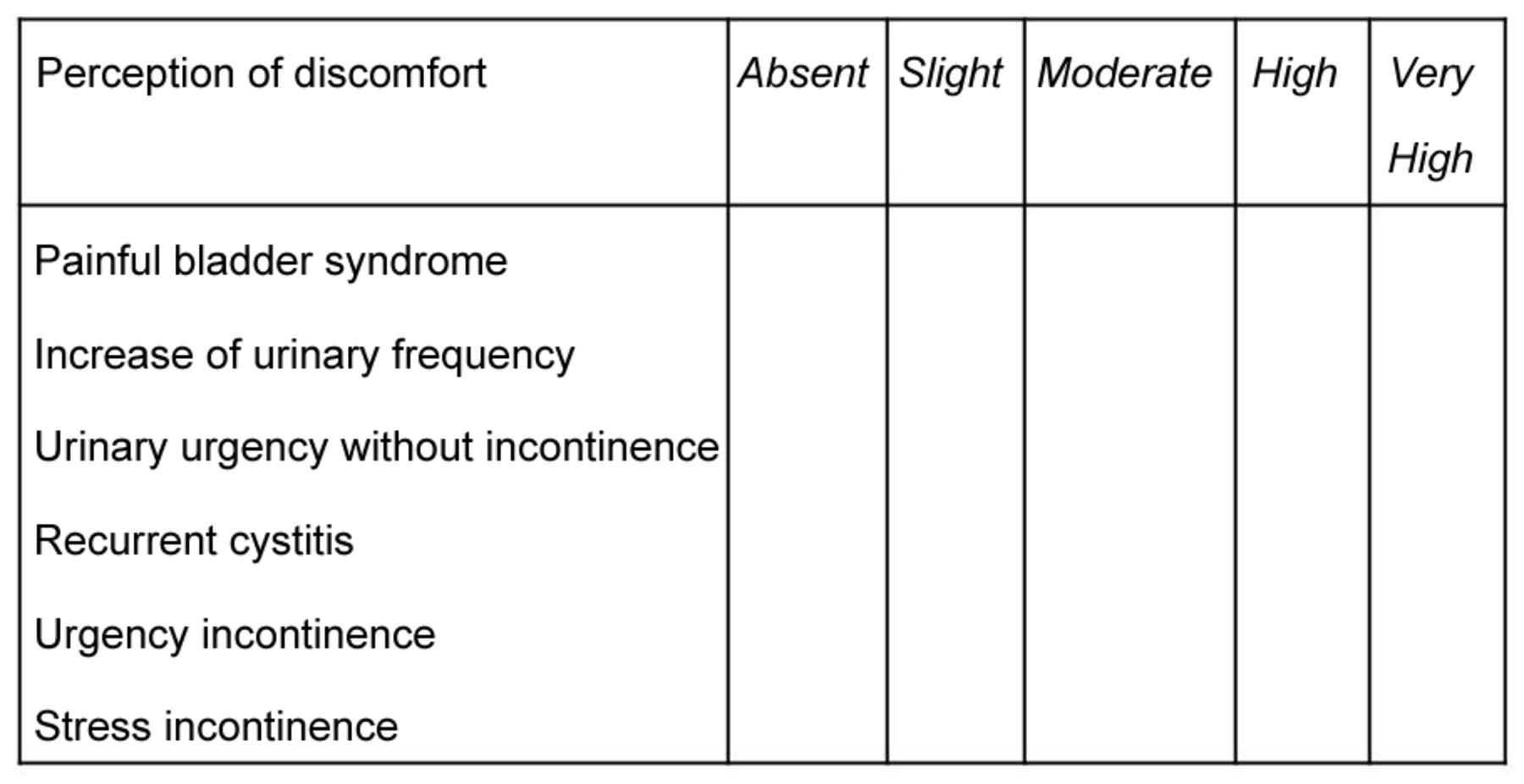
Verbal evaluation sheet to be completed at the first and at the second visit by patients, for quantifying the intensity of urinary symptoms.
Characteristics of recruited population patients for the clinical study.
At the second visit, two months from the first visit, only 5 patients (12.5%) of group 1 had positive urino-culture, two of which were diabetics, two had a rectocele, and one had a neurological bladder. No difference was found in this group regarding the type of antibiotic taken: 2 patients took fosfomycin, 1 patient took nitrofurantoin and 2 patients took ciprofloxacin according to dosage indicated in Materials and Methods.
In patients of group 2, treated with antibiotic therapy alone, after two months positive urine cultures were observed in 18 patients (90%), in the absence of other significant comorbidities. In both groups the distribution of the various antibiotic therapies was quite random. From the analysis of urine cultures after two months, group 1 showed an important reduction of 87.5% (from 40 to 5) of patients with positive urine cultures, as compared to group 2, which showed a reduction of only 10% of positive urine cultures (20 to 18) (Figure 2). Patients of group 1 and group 2 with persistence of positive urine cultures at second visit were not evaluated at 6 months because they were subjected to other than antibiotic therapies, and no comparison was possible between the two groups: at 6 months only 35 patients of Group 1 and Group 2 were evaluated. The 2 patients of Group 2 that showed negative urine cultures at second visit, showed positive urine cultures at six months, while the 35 patients of Group 1 showed persistence of negative urine culture after treatment with 1 vial of NDM every 24 h, after emptying the bladder, for 4 months.

Number of Group 1 (antibiotic associated at NDM) and Group 2 (antibiotic only) patients, positive for E. coli in urinary tract registered at the first (before treatment) and at the second visit (two months later).
Looking at the symptoms by using the verbal rating scale (VRS) for the 5 explored urological domains: urge incontinence, urgency, voiding frequency, recurrent cystitis, bladder and urethral pain, it is possible to observe a significant reduction in symptoms score registered at the second visit after two months, in patients of Group 1, treated with antibiotics associated at NDM, if compared to Group 2, treated with antibiotics alone (Figure 3).
Table II shows the intensity of the perceived symptoms reported at the first and at the second visit of the two groups: urgency incontinence, imperious urination, increasing voiding frequency, bladder and urethral pain, and the intensity of symptoms is referred to as mild, medium or severe. The results allow to observe that patients of Group 1 reported an improvement in perceived symptoms, especially for those affected by severe urinary bothersome; while for patients of Group 2 there was no improvement at clinical investigation carried out during the second visit.

{kind=link}
{kind=link}
{kind=link}
distribution of experienced discomfort in the five urological domains investigated in Group 1 (Antibiotic associated at NDM) and Group 2 (Antibiotic only) patients before and after treatment and at 1st and at the 2nd visit respectively.
Intensity of the symptoms experienced by patients in Group 1 (antibiotic and NDM) and Group 2 (antibiotic) before and after treatment, reported at the first and second visit.
At the second visit only 15 patients in Group 1 showed mild to severe symptoms as follows: 2 mild, 6 moderate and 7 severe, while at 6 months, only 8 patients of group 1 showed persistent symptoms (3 mild, 4 moderate and 1 severe). At six months, the 2 patients of Group 2 with positive urine culture showed also the recurrence of severe urinary bothersome.
Discussion
The genitourinary syndrome of menopause (physiologically as well as the one hormonally induced), especially in women with breast cancer, is accompanied by atrophy of the genital mucosa and episodes of recurrent cystitis, with a strong emotional and physical impact on women's health. In addition, the indiscriminate use of antibiotics often worsens the severity of symptoms and creates a chronicity of the recurrence increasing the frustration of the persistent failing of the antibacterial therapies (5). At the origin of the recurrence there is the possibility that the uropathogenic bacteria will create a biofilm, a mucopolysaccharide complex structure which tends to generate a chronic site of infection with the consequent developing of antibiotic resistance (14, 15). The results obtained in this study suggest that the integration of NDM to the antibiotic therapy, here evaluated in women who had breast cancer, could be an effective available tool to reduce bacteriuria, recurrent cystitis and urinary symptoms represented by the five urological domains explored.
Despite the small number of patients involved in the two study groups and the difference in the number of patients recruited in the two groups, the results are promising for even large-scale assessment. In Group 1, the persistence of symptoms after 6 months, though mild, in 8 women, is probably justified by the presence of various comorbidities and the different response of our immune system to inflammation. In fact, in group 1 were included 5 patients with persistent positive urinary culture, and those who, regardless of bacterial positivity, had a hypersensitive bladder as they suffered from genitourinary postmenopausal syndrome, which further complicates the effects of endocrine treatment on the genitourinary tract. The duration and the schedule of antibiotic therapy in recurrent cystitis is currently unknown because it is not possible to predict the time lead between a bladder infection to another in this risk population. It's very important to consider that the uro-genital syndrome severely impacts quality of life of patients both in their social relationships and in their daily work.
The results obtained demonstrate that the association of N-acetylcysteine, D-mannose and Morinda citrifolia fruit extract, with conventional antibacterial therapy, could reduce the need of antibiotic therapies responsible for chronic systemic resistances, that when used alone can often cause precarious vaginal and intestinal environments, favoring the phenomenon of infectious recurrence. In this sample of sixty women affected by breast cancer, the risk of recurrent urinary tract infections is very high due to tissue atrophy induced both by hormonal therapies used in the treatment of hormone-sensitive tumors, and by the effects of physiological estrogen deficiency if the cancer has been generated post-menopausaly. Therefore, antibiotic therapy associated with NDM allows to give more effectiveness to the antibiotics in reducing both the infection at the time and the risk of its recurrence. In addition, the above-mentioned therapy regimen provides a benefit in terms of reduced toxicity associated with prolonged antibiotic therapy, that may add further disadvantages to breast cancer survivors, already physically and psychologically affected by the side-effect of common anticancer drugs.
In conclusion, in selected patients, the association of NAC, D-mannose, and Morinda citrifolia fruit extract, allow to improve the effectiveness of antibiotic therapy maintaining the result over time in fighting the pathogenic effect and resistance of uropathogenic bacteria. It is also very important to point out how the therapeutic efficacy is associated with a reduction in urogenital discomfort that in women with long-life expectancy impacts their intimate and daily sphere.
Footnotes
This article is freely accessible online.
Conflicts of Interest
Dr. Pier Paolo Zanello and Dr. Debora Marchiori are Deakos scientific consultants.
- Received May 31, 2017.
- Revision received June 19, 2017.
- Accepted June 20, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved