

Abstract
Background: Bronchial carcinoid tumors (BCTs) are rare neuroendocrine neoplasms of the lung that mainly have a central distribution. They are classified as typical and atypical, with the former variant generally conferring a more favorable survival. Central tumors are usually symptomatic with features of bronchial obstruction, whereas peripheral tumors may remain silent. Case Report: A 36-year-old woman presented to our hospital due to an episode of massive hemoptysis 5 days prior to admission. She had experienced another episode of hemoptysis 4 years before, for which a chest x-ray had shown no pathological findings. A new chest x-ray showed complete collapse of the left lung, with remarkable tracheal deviation. Computed tomography revealed a large endobronchial lesion causing occlusion of the left main bronchus and significant mediastinal shift to the left. Despite the collapse of the left lung, no symptoms of bronchial obstruction were evident. The patient underwent a successful left pneumonectomy and pathology of the resected specimen revealed a typical stage pT2b N1 Mx endobronchial carcinoid tumor. Conclusion: Central tumors are usually symptomatic with features of bronchial obstruction, whereas peripheral tumors may remain silent. Although a significant amount of bronchial occlusion may be present, symptoms of obstruction might not be apparent. Hemoptysis should always be thoroughly investigated, as it may be the only sign of a severe underlying disease.
- Pneumonectomy
- mediastinal shift
- tracheal deviation
Bronchial carcinoid tumors (BCTs) are neuroendocrine neoplasms of the lung and represent about 1-2% of all primary lung tumors. Although first classified as benign tumors, they are nowadays considered as low-grade malignant neoplasms (1). BCTs originate from Kulchitsky cells in the bronchial mucosa, neuroepithelial bodies, or pluripotential bronchial epithelial stem cells (2). Based on their pathological features, they are also classified as typical and atypical, with the former variant generally conferring a more favorable survival (3). About one-third of patients are asymptomatic, whereas cough, recurrent pneumonia and hemoptysis account for the majority of the symptoms, especially in the case of centrally located tumors (4). Herein, we report a case of a large BCT totally occluding the left main bronchus without producing symptoms of bronchial obstruction.
Case Report
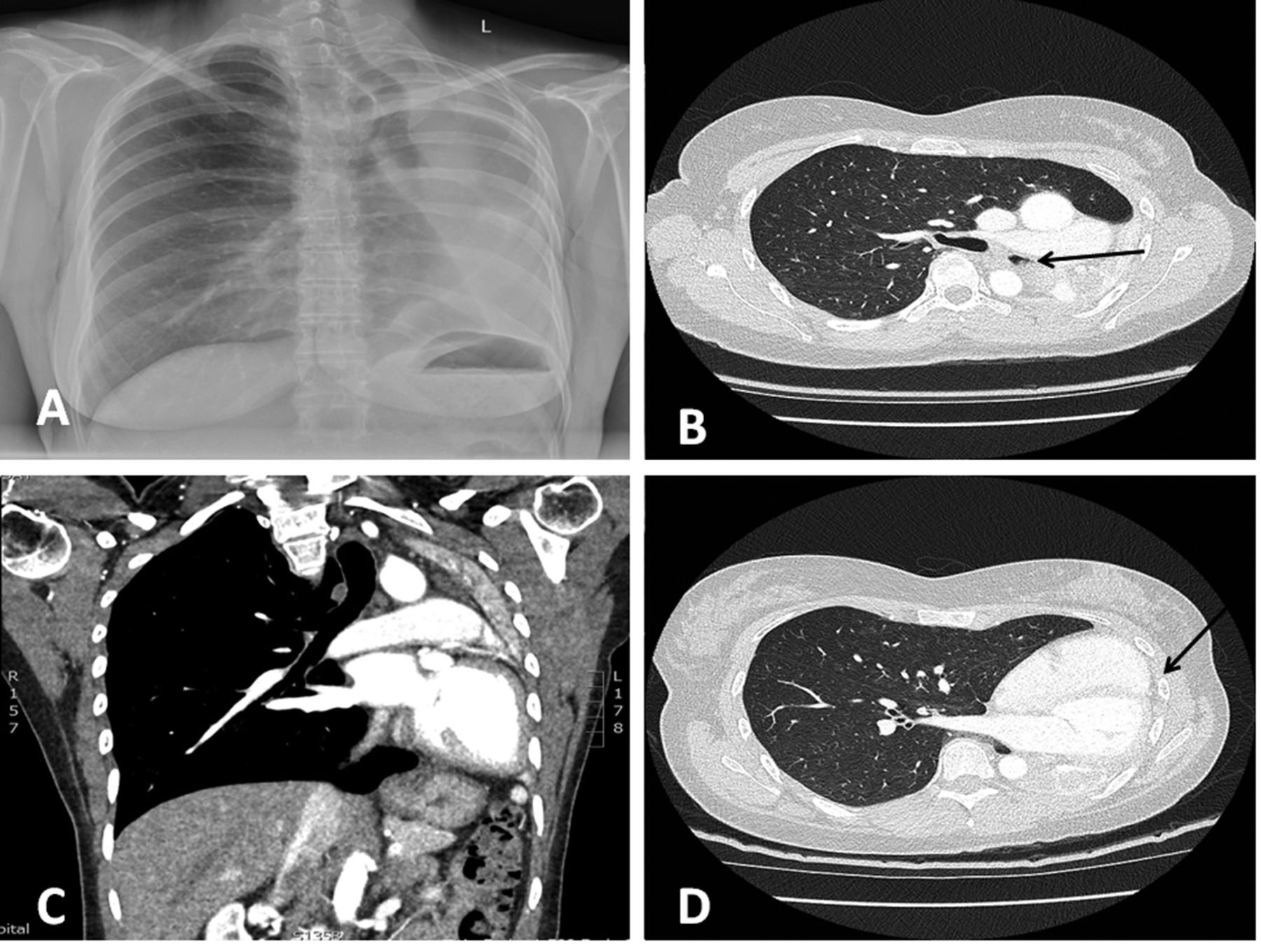
A 36-year-old woman presented to our hospital due to an episode of massive hemoptysis 5 days prior to admission. She was a cannabis smoker and her past medical history was only remarkable for an episode of hemoptysis 4 years before, for which a chest x-ray was performed, but no pathological findings were shown. Therefore, it was considered as incidental and no further investigation was recommended at that time. However, a new chest x-ray showed complete collapse of the left lung, with remarkable tracheal deviation (Figure 1A). Computed tomography revealed a large endobronchial lesion causing occlusion of the left main bronchus (Figure 1B) and significant mediastinal shift to the left (Figure 1C and D). Despite the collapse of the collapse left lung, no symptoms of bronchial obstruction were evident. The patient underwent successful left pneumonectomy through thoracotomy and pathology of the resected specimen revealed a typical stage pT2b N1 Mx endobronchial carcinoid tumor. At a follow-up of 12 months, she remains alive and all examinations have failed to reveal any recurrent disease.

{kind=link}
A: Chest x-ray showing left lung atelectasis with remarkable tracheal deviation. B: Computed tomography showing a 59-mm endobronchial lesion (arrow) causing occlusion of the left main bronchus. C: Coronal computed tomographic view of the chest. D: Significant mediastinal shift to the left, leading to the heart being in contact with the lateral chest wall (arrow).
Discussion
BCTs are rare neoplasms, with a reported annual incidence of 0.2-3 per 100,000 people (1, 3). No clear sexual or racial predilection has been documented. Typical BCTs have been reported in all age groups but a peak around the fourth decade has been documented (1, 3). On the contrary, the atypical variant occurs more frequently during the fifth decade of life (1). BCTs are capable of synthesizing, storing, and secreting peptide hormones, as well as serotonin, adrenocorticotropic hormone, somatostatin and bradykinin (4, 5).
The vast majority of BCTs arise centrally in the main, lobar or segmental bronchi and demonstrate no specific lobar distribution (6). Central tumors are usually symptomatic with features of bronchial obstruction and ball-valve effect for polypoid tumors, whereas peripheral tumors are usually asymptomatic (6). The main complaints include cough, fever, expectoration, wheezing, hemoptysis, chest pain or symptoms simulating asthma (7, 8). Due to the high tumor vascularity, hemoptysis occurs in at least 50% of patients (8, 9), whereas approximately one-fourth of patients are diagnosed incidentally (9). In our case, despite the total occlusion of the left main bronchus leading to collapse of the left lung, the patient had no symptoms of bronchial obstruction, but only two episodes of hemoptysis with a time interval of 4 years between them.
Due to its rarity and the low index of suspicion, diagnosis is often missed or delayed even in symptomatic patients (1, 4). It is, therefore, of paramount importance to evaluate and examine in detail every episode of hemoptysis rather than considering it as an incidental finding. In our case, notably, if a thorough investigation had been performed at the first episode, the patient could probably have avoided pneumonectomy.
In contrast to other types of lung cancer, BCTs generally confer a better prognosis. In particular, typical BCTs are associated with superior survival compared to the atypical variant, with 5- and 10-year survival rate of 91-95% and 86-89%, respectively (1, 3). Furthermore, atypical BCTs have been identified as a risk factor for recurrence (10, 11). Fortunately, our patient was diagnosed with a typical BCT and remains healthy 12 months after pneumonectomy.
Conclusion
BCTs are rare, low-grade malignant tumors of the lung that mainly have a central distribution. Central tumors are usually symptomatic with features of bronchial obstruction, whereas peripheral tumors may remain silent. Although a significant amount of bronchial occlusion may be present, symptoms of obstruction might not be apparent. Hemoptysis should always be thoroughly investigated, as it may be the only sign of a severe underlying disease.
Footnotes
This article is freely accessible online.
Conflicts of Interest
The Authors declare no conflicts of interest.
- Received June 11, 2017.
- Revision received June 21, 2017.
- Accepted July 3, 2017.
- Copyright© 2017, International Institute of Anticancer Research (Dr. George J. Delinasios), All rights reserved