

Abstract
Background: Extrdural granulation or abscess is a possible complication of chronic suppurative otitis media (CSOM) with cholesteatoma. However, due to development of newer antibiotics and advances in bacteriology and imaging techniques, the incidence of extradural granulation or abscess has significantly decreased. The present study analyzed the clinical presentation, imaging findings, and surgical treatment of eight patients with CSOM with cholesteatoma extending to the cranial fossa. Patients and Methods: From 2000 to 2012, 1,010 patients were surgically treated for CSOM with cholesteatoma. Patients with extension to the cranial fossa were studied. Clinical presentation, imaging studies, operative findings, surgical treatment, and postoperative results were evaluated. Results: Twenty cases (1.9%) in a series of 1,010 patients with CSOM with cholesteatoma had bony destruction of the cranial fossa in the temporal bone computed tomography (cr). Of the 20 cases, eight (0.79%) were identified as extradural granulation by magnetic resonance imaging. One patient exhibited nodular enhancement, but it disappeared on preoperative antibiotic treatment. Surgical access for removal of cholesteatoma with extradural granulation was accomplished through canal wall-down tympanomastoidectomy. Conclusion: CSOM with cholesteatoma can extend to either the middle or posterior cranial fossa. While CT is sufficient to reveal bony destruction of the cranial fossa, magnetic resonance imaging is required to differentiate and define intracranial extension of CSOM with cholesteatoma.
- Chronic suppurative otitis media
- extradural granulation
- MRI
The spread of infection from the middle ear to the intracranial space involves four major routes: bone erosion, thrombophlebitis, periphlebitis, and other pathways (1-4). The most common cause of the extension of chronic suppurative otitis media (CSOM) is osteitis or cholesteatoma erosion. In contrast to other complications of CSOM, extradural abscess or granulation results exclusively from destruction of the bone in CSOM with cholesteatoma. When there is destruction of the bone adjacent to the dura, the purulence contacts the dura and an epidural abscess forms. Temporal bone high-resolution computerized tomography (CT) has greatly contributed to the understanding of the pathological processes by which CSOM and its complications develop. However, magnetic resonance imaging (MRI) is superior to CT in showing suppurative intracranial lesions (5). Due to the development of newer antibiotics, and advances in bacteriology and imaging techniques, the incidence of extradural granulation by CSOM with cholesteatoma has significantly decreased (4). The purpose of this study was to analyze clinical presentation, imaging findings, and surgical treatment of eight patients with CSOM with cholesteatoma extending to the cranial fossa.
Patients and Methods
A retrospective review was carried-out in an electronic patient database of 1,010 mastoidectomy cases for CSOM with cholesteatoma, performed at our tertiary otolaryngologic care Centers between November 2000 and December 2012. Preoperative imaging of the temporal bone was obtained for all patients and included computed tomography or magnetic resonance imaging. The size of the bony destruction of the cranial fossa in CT was detected and the diameter was measured. The operative reports on all patients were reviewed and included specific information on the sites of cholesteatoma involvement and surgical approach. The criterion for inclusion in the study was surgically-documented evidence of CSOM with cholesteatoma extending into the middle or posterior cranial fossa. A complete otological history was obtained for all patients and included specific information on chief complaint, hearing loss, aural discharge, better hearing ear, vertigo, family history, prior otological surgery, hearing amplification, general health, and medications. Otomicroscopy, head and neck examination, neurological examination, and audiological evaluation were performed on all patients.
Patient's data.
Results
The bony destruction of the mid or posterior cranial fossa was detected in 20 patients (1.9%) out of an electronic patient database of 1,010 mastoidectomy cases for CSOM with cholesteatoma. Preoperative temporal bone MRI with Gd enhancement was performed in 20 patients. Of the 1,010 patients, eight cases (0.79 %) were identified as extradural granulation on MRI and surgery (Table I). Two patients were women and six were men. Their are ranged from age from 11 to 69 years, with a mean of 42.5 years. Five patients had a chief complaint of chronic purulent otorrhea, one presented with intermittent dizziness, and one presented with intermittent headache. One patient had a history of recurrent infection in the operated ear. The mean age at the onset of ear infection was 11 years. Audiometry showed a conductive hearing loss in two patients and a mixed-type hearing loss in six patients. Axial enhanced T1-weighted MRI showed a non-enhancing cholesteatoma surrounded by a ring of abnormally-enhancing granulation tissue. The enhancement pattern was linear in seven patients, and a combination of linear and nodular in one. The middle cranial fossa was involved in three patients, whereas the posterior fossa was involved in two patients. The other three patients exhibited combined involvement of both cranial fossa. None of the eight patients exhibited meningeal signs. All patients had used ototopical ciprofloxacin solution before the operation. All patients underwent canal wall-down mastoidectomy mastoid obliteration. Extradural granulation was peeled from the dura without removal of neighboring bone. The condition of all of these patients improved considerably soon after surgery. Two cases whose cultures showed methicillin-resistant Staphylococcus aureus, were treated by vancomycin before and after mastoidectomy. One patient whose culture revealed Pseudomonas aeruginosa was treated by ceftazidime. There was no evidence of recurrent cholesteatoma during the follow-up period, which ranged between six months and seven years. Further details of treatment are presented for two patient cases in particular.
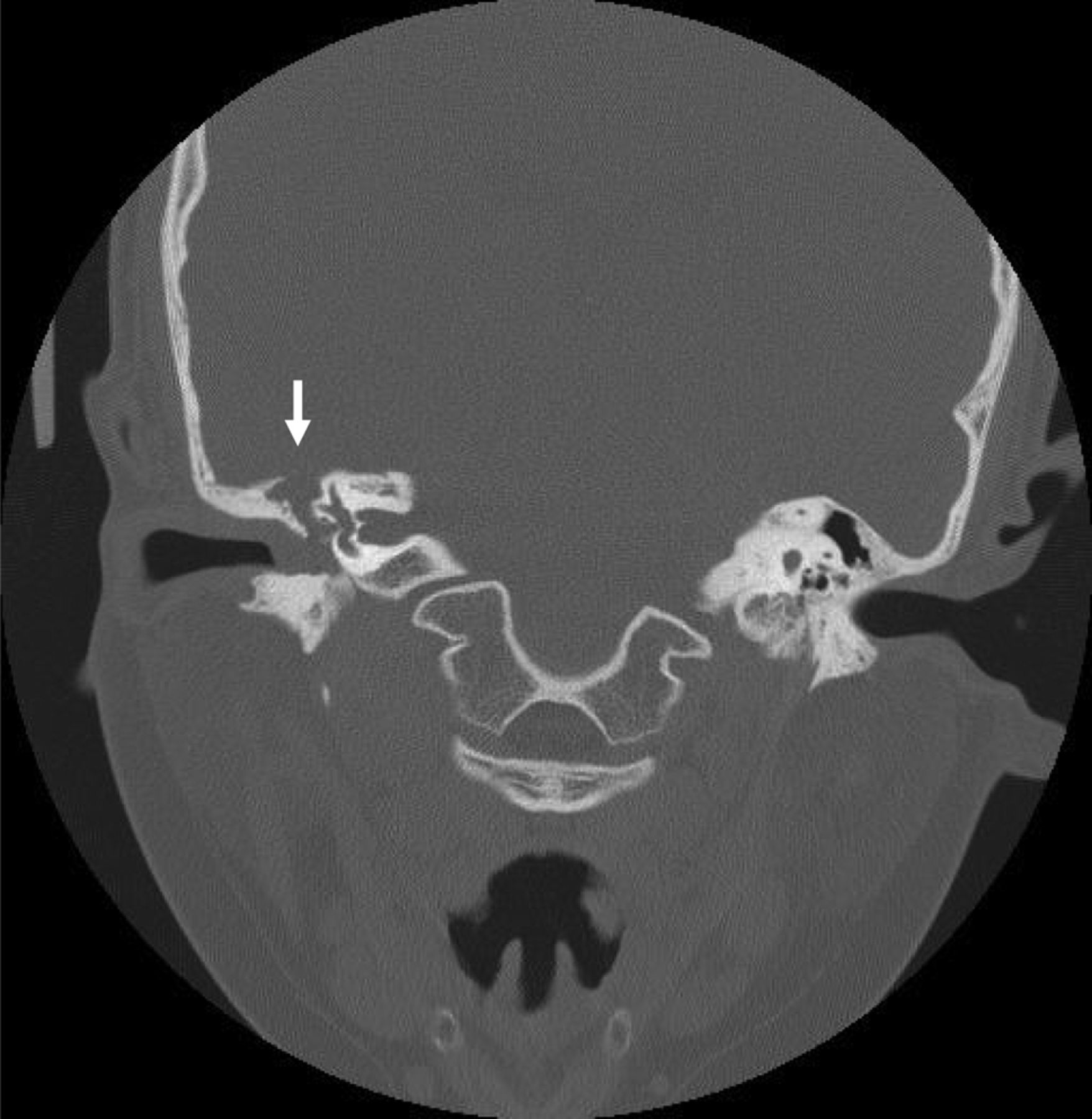
Temporal bone shows a bony destruction (arrow indicates) at the tegmen.
Case 1. An 11-year-old boy was referred to our clinic complaining of hearing loss in the right ear and otorrhea. He presented with hearing loss with non-whirling type dizziness. He had no nystagmus and fever, but complained of an intermittent headache. A neurotological examination was unremarkable. An otoendoscopic examination revealed an aural polyp with pulsating discharge in the right ear and a normal tympanic membrane of the left ear. An otomicroscopic examination revealed aural polyp with keratin debris from the attic in the right ear and a normal left ear. Audiometry revealed a moderate conductive hearing loss (mean 50 dB) in the right ear. An unenhanced temporal bone CT demonstrated soft tissue density in the external auditory canal and within the mastoid on the right side. Clear evidence of bony defect at the tegmen was noted (Figure 1). A temporal bone MRI with Gd-diethylenetriaminepenta acetic acid administration showed CSOM with cholesteatoma, extending to the middle cranial fossa in the right ear. A markedly enhanced dura was noted in the right ear (Figure 2A). The patient received oral antibiotics (100 mg/day of cefixime) for three weeks as an outpatient. Irrigation with diluted vinegar solution was carried-out, following ototopical ciprofloxacin (Ciprobay®; Alcon, Korea). Two weeks later, the discharge had stopped and was coincident with the spontaneous loss of the aural polyp. A follow-up MRI revealed the loss of the enhanced dura of the middle fossa (Figure 2B). The patient underwent canal wall-down tympanomastoidectomy (type III) using cartilage columella on the stapes. Mastoid obliteration was performed by autologous bone pate with fibrin glue. A cholesteatoma was found filling the mastoid cavity and epitympanum which had invaded into the middle cranial fossa. All cholesteatoma matrix and granulation tissue were peeled from the dura by a blunt instrument. The dehiscent dura appeared mildly swollen. The mastoid cavity was obliterated using bone pate and cartilage chips. There was no evidence of recurrent cholesteatoma during the follow-up period of five years. Postoperative audiometry showed a closed air-bone gap compared to the preoperative state (Figure 3).
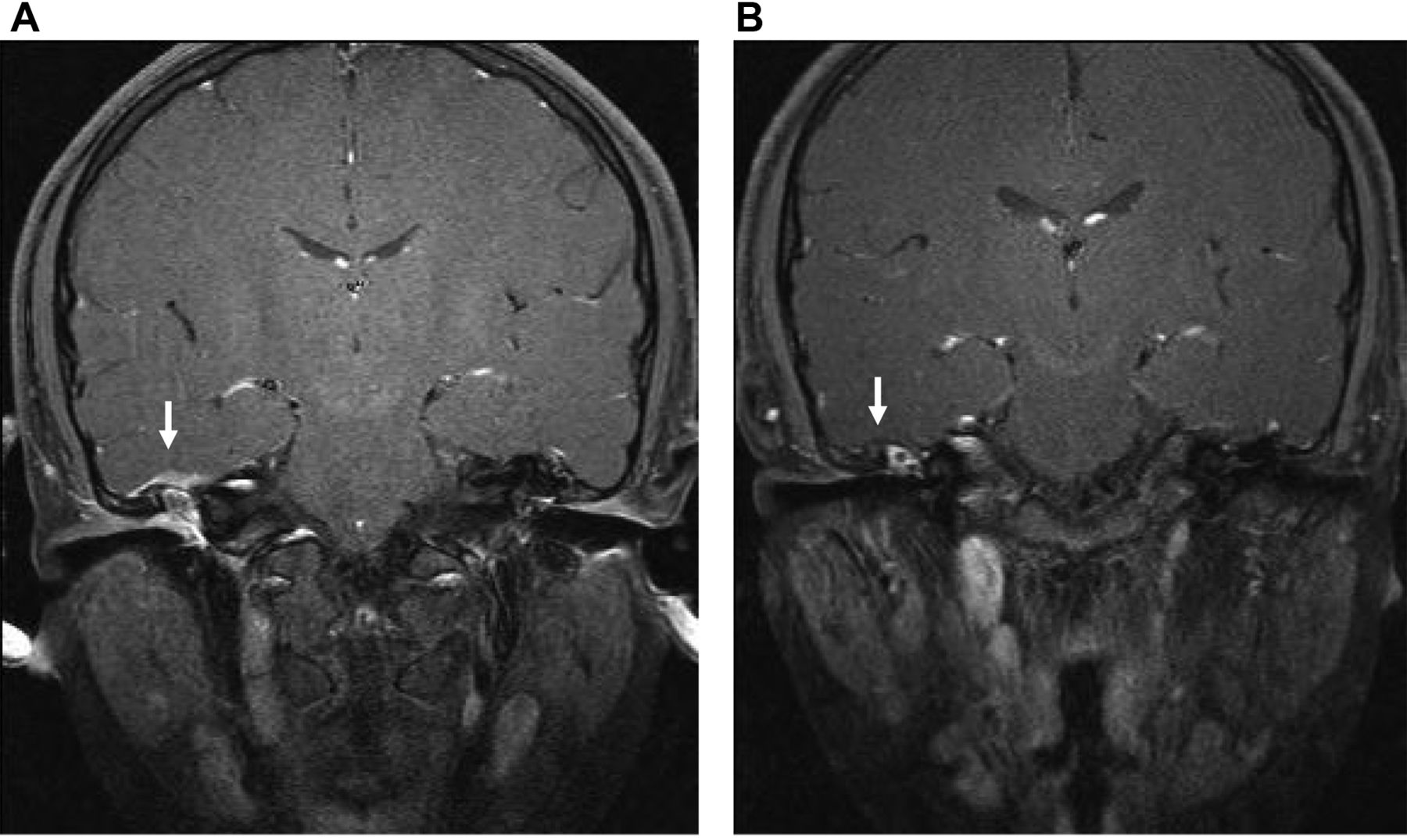
Preoperative MRI shows a marginal enhancement of extradural area (arrow indicates, A). After antibiotic treatment, previoius extradural enhancement was disappeared (B).
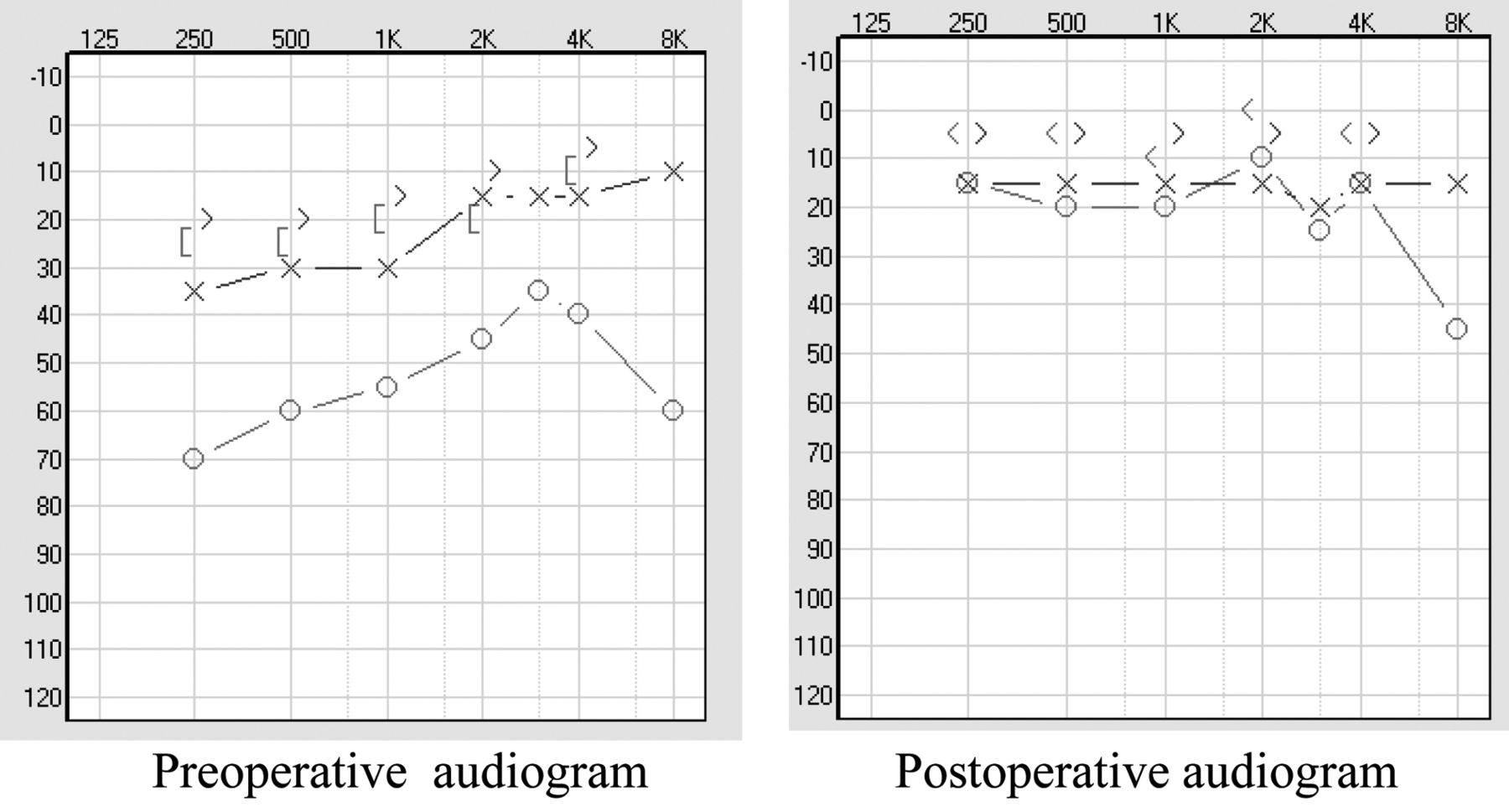
Postoperative pure tone audiogram reveals a closed air bone gap compared to preoperative audiogram.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
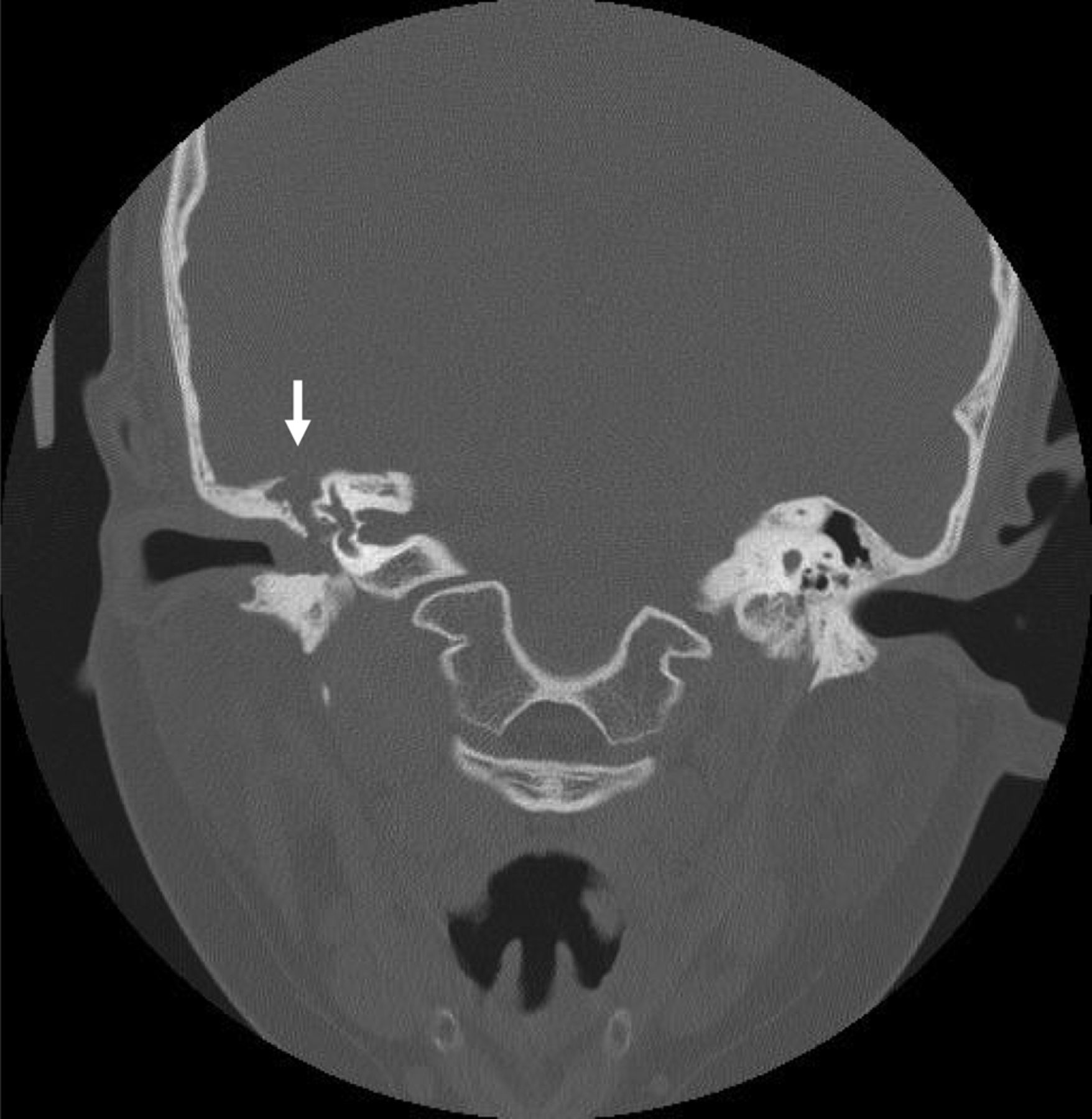
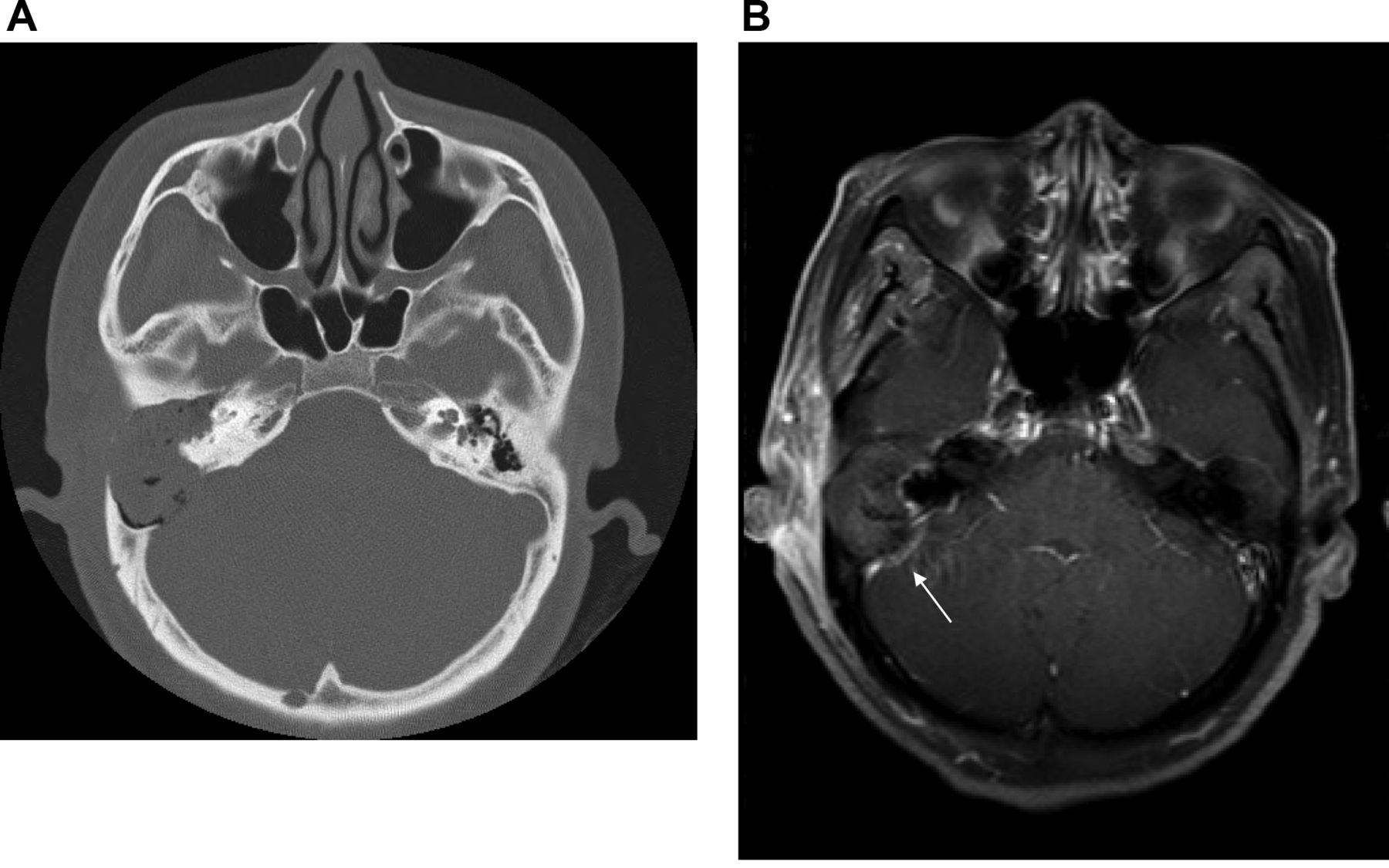
Preoperative temporal bone CT shows bone destruction at the posterior cranial fossa (A). Preoperative MRI shows a extradural enhancement at the posterior cranial fossa (arrow indicates, B).
Case 5. A 36-year-old woman was referred to our clinic complaining of hearing loss in the right ear. The external auditory canal was obstructed by a soft mass. Retroauricular area showed subperiosteal abscess-like appearance. Her audiogram revealed a profound hearing loss on the right and normal range on the left. TBCT showed a middle ear and mastoid cavity mass with clear bony destruction of the posterior cranial fossa (Figure 4A). Superior and posterior semi-circular canal destruction was noted. MRI showed an enhancement of the posterior cranial fossa without cerebellar abscess or labyrinthitis (Figure 4B). Right canal wall mastoidectomy was performed. The mastoid showed extensive central destruction and was in direct communication with the posterior superior part of the external auditory canal by cholesteatoma. There was a destruction of a wide area of the posterior cranial fossa and over the lateral venous sinus. The dura mater of the posterior cranial fossa showed granulomatous thickening. The cholesteatoma sac and extradural granulation were peeled carefully by a blunt instrument. There was no evidence of recurrent cholesteatoma during the follow-up period of seven years.
Discussion
Widespread use of anti-microbial drugs in the management of otitis media has significantly reduced the incidence of extradural abscess nowadays (1, 2). However, complicated extradural granulation still remains. These cases result from destruction of bone in coalescent mastoiditis and petrositis, and in chronic otomastoditis complicated by cholesteatoma. Extradural granulation may occur in the middle cranial fossa when there is destruction of the tegmen of the middle ear and mastoid. Posterior cranial fossa extradural granulation occurs when there is destruction of the bone in Trautman's triangle, over the sigmoid sinus plate. MRI is the study of choice for locating otogenic intracranial complications. CT may be limited in differentiating soft tissue density in acute infection. In cases of intracranial infection, MRI may improve the diagnostic accuracy, with increased sensitivity and specificity (6).
In general, cholesteatoma have nonspecific signal intensity on T1 weighted MRIs with some rim enhancement after contrast administration. They are moderately hyperintense on T2 weighted images. Extradural granulation tissue, associated with cholesteatoma, cannot be differentiated from a cholesteatoma on a noncontrast CT. However, this differentiation can be made with a Gd contrast MRI examination because granulation tissue will enhance, whereas a cholesteatoma will not. Temporal bone high-resolution CT allows identification of bone defects over the tegmen, sigmoid sinus and the bony facial canal in the extensive cholesteatoma. The extent of the soft tissue mass and commonly associated complications can be easily visualized. Temporal bone MRI plays a valuable role when a cholesteatoma is suspected of extending outside the temporal bone. In the present study, extradural enhancement was identified by MRI.
Management of CSOM with extradural granulation tissue is performed by tympanomastoidectomy. During the operation, the dura should be properly inspected by thinning the bone carefully. The bone does not need to be removed to identify normal or abnormal dura. If the dura appears normal in these areas, no additional work is necessary. It is not necessary to remove the bone completely to see whether the dura is normal or abnormal (7). If the dura is abnormal, the bone should be removed over the abnormal dura until the normal dura is encountered. If an abscess is encountered, exposure satisfactorily drains the abscess (8, 9). In the present study, extradural abscess was not found in any case during surgery. Excess granulation tissue should be removed with a blunt instrument, scraping parallel with the plane of the dura. Care must be taken not to perforate the dura. In the present study, excess granulation tissue was removed in all cases. The bony defect was sealed by bone pate using fibrin glue. Mastoid obliteration was performed in all cases using bone pate or rib cartilages.
Conclusion
In the past 13 years, we experienced complicated extradural granulations in only eight cases among the 1,010 cases of cholesteatoma (0.79 %). There were no extradural abscesses. MRI is superior to CT in showing extradural granulation. Extradural granulation complicated by CSOM with cholesteatoma was treated by canal wall-down tympanomastoidectomy in all cases.
- Received January 18, 2014.
- Revision received March 19, 2014.
- Accepted March 20, 2014.
- Copyright © 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved