

Abstract
Conchal cartilage or cartilage/ temporal fascia composite grafting (DC-F) used for rhinoplasty is applied by plastic surgeons for reconstructive purposes. Previous studies on experimental models such as mice or rabbits have elucidated on the late events following grafting, with tissue specimens being harvested two months after implantation. Early microscopic and molecular events following DC-F grafting are completely unknown. We designed a chick embryo chorioallantoic membrane model for human grafts study, regarding the dynamic observation of graft survival and its mutual interrelation with the chick embryo chorioallantoic membrane microenvironment. The DC-F graft preserved its cartilage component in a normal state compared to cartilage graft-only because of protective factors provided by temporal fascia. Its strong adherence to the cartilage, lack of angiogenic factors and high content of collagen IV-derived fragments with anti-angiogenic effects make the temporal fascia a good protective tissue to prevent implanted cartilage degeneration. The cartilage graft produced high inflammation, stromal fibrosis and activated angiogenic cascade through VEGF-mediated pathways followed by cartilage degeneration. Also, high content of podoplanin from conchal cartilage chondrocytes exerted a major role in inflammation accompanying cartilage graft. The presently employed experimental model allowed us to characterize the early histological and molecular events triggered by temporal fascia, cartilage or composite graft DC-F implanted on chick embryo chorioallantoic membrane. Our microscopic and molecular observations may help explain some post-surgical complications generated after using cartilage alone as biomaterial for nasal augmentation, supporting the use of DC-F composite graft, with the aim to reduce unwanted post-surgical events.
- Conchal cartilage
- temporal fascia
- chick embryo choriallantoic membrane
Nasal reconstruction remains one of the most common surgical techniques used for esthetic reasons or reconstruction following nasal tumor removal. Conchal cartilage or diced cartilage/temporal fascia composite graft (DC-F) used for rhinoplasty represents a relative new technique applied by plastic surgeons for reconstructive purposes.
In the past, conchal cartilage and temporal fascia were separately used both as materials for nasal reconstruction. Trimble (1), reported for the first time the use of nasal cartilage grafts in reconstrucitve rhinoplasties following malignant tumor removal from the facial region (2). Eight years later, Muenker (3) described the use of bilateral conchal cartilage for rhinoplasty, as an alternative for previous techniques. But the inesthetic appearance of cartilage grafts, with persistence of subcutaneous irregularities and the presence of a high rate of postoperative complications as cartilage graft resorbtion represented the main reason to start seeking other more conveninent solutions to improve viability of such grafts. Thus, Gurrerosantos proposed the use of human tissues as an easy material to re-model when used in nasal reconstructive techniques (4). Temporal fascia as a single tissue component did not show good results in nasal reconstructions.
Initially applied in malar augmentation technique (5), conchal cartilage/temporal fascia composite graft seems to be accepted by more and more plastic surgeons because of the obtained encouraging results (6-9). Although, in some cases, postoperative complications still remain an inconvenience for this technique.
Several artificial materials or human tissues were tested for such reconstructive methods. The use of artificial materials for these procedures produced a high rate of side-effects and increased postoperative complications. Some of them presented side-effects such as inflammation, necrosis or graft rejection. Lack of experimental data which could explain these events limited the knowledge regarding their triggering and, subsequently, the elucidation of pathogenic mechanisms responsible for them.
Morphological and molecular substrates of DC-F variable viability are less known. Lack of microscopic data concerning this subject are due, on one hand, to a limited collaboration between plastic surgeons and pathology Departments and, on the other to absence of experimental models designed for the study of dynamic changes of the implanted graft starting from the first day of implantation. At present there is only one article regarding microscopic characterization of the DC-F harvested from patients with post-surgical complications (10) and only one report on graft of DC-F in nude Rowlett rat subcutaneous pouch model (11). This experimental model highlighted the late events following grafting, tissue specimens being harvested two months after implantation. Early microscopic and molecular events following DC-F grafting are completely unknown.
Based on these evidence, we designed and characterized a chick embryo chorioallantoic membrane model for the study of DC-F composite grafting early events following implantation. The main advantage of this model was a dynamic observation of graft survival and mutual interrelation between DC-F composite graft and microenvironment of the chick embryo chorioallantoic membrane (CAM).
Materials and Methods
Tissue preparation. Conchal cartilage and temporal fascia were harvested from a 54-year-old male patient admitted to the Plastic Surgery Department for nasal reconstruction. A composite graft type DC-F was obtained and used as reconstructive biomaterial for nose augmentation. For the experimental model, three types of tissues were obtained: conchal cartilage (C), temporal fascia (F) and conchal cartilage wrapped in temporal fascia (DC-F), the last one being prepared and used by the plastic surgeon for nasal reconstruction. A signed consent was obtained from the patient after an accurate information about all procedures. The Ethics Committee of Victor Babes University of Medicine and Pharmacy approved the study protocol according to the World Medical Association Declaration of Helsinki. All three types of human tissue samples were placed in 9% saline solution, and to the experimental department within 15 min from their initial removal. Tissue pieces prepared for implantation were 0.3-0.5 mm in size and were placed on chick embryo chorioallantoic membrane previously prepared for implantation.
Chick embryo chorioallantoic membrane (CAM) was chosen as the experimental model for the present study because of several advantages: low cost, quick preparation, high facilities for daily macroscopic and microscopic direct observations and samples monitoring (12, 13).
Briefly, twenty White Leghorn eggs were carefully selected and incubated for 72 h at 37°C in a humidified medium. After removal of 3 ml of albumin, incubation was continued one more day and then, a shell window was performed on the upper part of the egg and CAM direct visualization was obtained. Incubation period continued until day 7 when, a silicon ring was applied on the surface of the CAM (Figure 1, a-c). We organized four groups including five CAMs each. For the control group we applied silicon rings only. Other three groups were labelled with C (from conchal cartilage), F (from fascia) and DC-F (diced cartilage-fascia composite graft) (Figure 1, d-f). Correspondent samples of cartilage, temporal fascia and composite graft were applied inside the silicon ring on CAM surface after non-traumatic, non-hemorrhagic CAM scratch. The specimens were monitored during 7 days from implantation. Macroscopically parameters as graft viability, vascular response to implants, presence or absence of inflammation were dynamically evaluated. The experiment was stopped on day 15 of incubation (day 8 after tissues implantation). Macroscopic observations were confirmed by histology, immunohistochemistry and in situ hybridization techniques.
Primary processing and microscopic evaluation. Tissue grafts were initially fixed in ovo by adding 10% buffered formalin for 60 min. Then, we removed the CAM implants from the egg, arranged them on a watch glass and microscopically evaluated before their paraffin embedding. Routine paraffin embedding process was followed by obtaining 3-micrometer thick serial sections from each paraffin block. Initial evaluation was performed on haematoxylin and eosin-stained slides. Additional sections were selected for immunohistochemistry and in situ hybridization techniques.
Immunohistochemistry. Immunohistochemistry was performed in a fully-automated manner with Bond Max Autostainer (Leica Microsystems, UK). Slides were loaded into the autostainer and processed by using standardized kits for this procedures. Several pro-angiogenic and anti-angiogenic markers were evaluated: VEGF (clone VG1, Dako, Carpinteria USA, dilution 1:25), FGF and PDGF (Reliatech, Germany), D2-40 (Dako, Carpinteria, USA), Prox1 (Reliatech, Germany), Endostatin (Reliatech, Germany), colagen IV (Dako, Carpinteria, USA), F VIII-related antigen (Dako, Carpinteria, USA).
RNAscope method. To validate the immunohistochemical results and assess cellular RNA content as single-molecule visualisation in individual cells on paraffin-embeded specimens a novel probe design strategy was used in addition to a hybridization-based signal amplification system to simultaneously amplify signals and suppress background. HRP-conjugated double Z probes for VEGF, FGF and podoplanin, complementary for the target RNA were designed by Advanced Cell Diagnostics (Hayward, CA, USA). We used RNAscope 2.0 High Definition Kit (Advanced Cell Diagnostics, Hayward, CA, USA) for signal amplification followed by visualisation of amplified signals with diaminobenzidine as chromogen.
Briefly, to prepare FFPE specimens for the RNAscope procedure, the tissues were fixed and permeabilized to allow for target probe access. A 2-h hybridisation step performed at 40°C was followed by multi-step signal amplification done by applying reagants from RNAscope High Definition Kit (Advanced Cell Diagnostics, Inc., Hayward, California, USA) followed by RNA visualisation as brown dotted spots with diaminobenzidine. The working protocol was similar with those described by Wang et al. (14). The detection sensitivity of RNAscope method was proved by using positive (POLR2A) and negative (probes against the bacterial gene dapB) controls assessed in the same manner with our specimens.
Results
Chorioallantoic membrane implants were monitorized daily concerning their viability and structural changes. The first macroscopic changes started to become evident from day 3 post-implantation (ID7), the effects being maximal on day 15 post-implantation. Chick embryo chorioallantoic membrane vascular network was reactive to all three implant types but specific for each of them.
An intense angiogenic effect was observed for the cartilage implant (C) characterized by the development of a rich network of small neovessels with a specific “spoke-wheel”-like arrangement around (C) implant (Figure 2a). Cartilage tissue implant became vascularized, being invaded by small blood vessels (Figure 2b). An unexpected inhibition of CAM vascular network was obtained following temporal fascia implantation on chick CAM surface. Vascular microvessels density decreased around the temporal fascia implant and an avascular area could be observed around it (Figure 2c). Moreover, this inhibitory effect was observed far from the implant also. (Figure 2d, e and f). A strong adherence of the temporal fascia to the chick CAM was noticed.
A stereomicroscopic analysis was performed after implants were harvested and before their fixation in bufferred formalin. Stereomicroscopy confirmed the previous macroscopic observations and, moreover, demonstrated a high density of small blood neovessels that can be seen invading the cartilage. They were irregular in shape with a tortuous appearance inside all cartilage tissue implant.
The third step in the evaluation of cartilage and temporal fascia behaviour was represented by the implants of composite graft DC–F on chick CAM (Figure 2g). This graft was composed by conchal cartilage which had a face covered by temporal fascia and an opposite face without fascia coverage. DC-F implantation was performed in such manner as both sides of the graft to have contact with chick CAM. Eight days after implantation, significant differences concerning the vascular network were noticed for both sides (covered and uncovered by temporal fascia) of the graft implanted on CAM. The cartilage side without temporal fascia coverage generated an intense angiogenic response characterized by several small blood vessels converging to the implant. The other side of the cartilage, covered by temporal fascia inhibited CAM blood vessels (Figure 2h).
Macroscopic and stereomicroscopic observations requires confirmation by histology, immunohistochemistry and molecular assessement of collected samples.
These complementary tests were performed on the same three types of specimens previously evaluated. The main purpose was to identify pro-angiogenic and anti-angiogenic factors responsible for different effects of cartilage and temporal fascia implants effects on the CAM vascular networks.
First evidence were observed on haematoxylin and eosin-stained specimens concerning CAM stroma surrounding implants (Figure 3a). Hypercellular stroma rich in fibroblast-like cells and inflammatory cells was detected around cartilage grafts while the DC-F side protected by temporal fascia produced no microscopic evident stromal changes (Figure 3b).
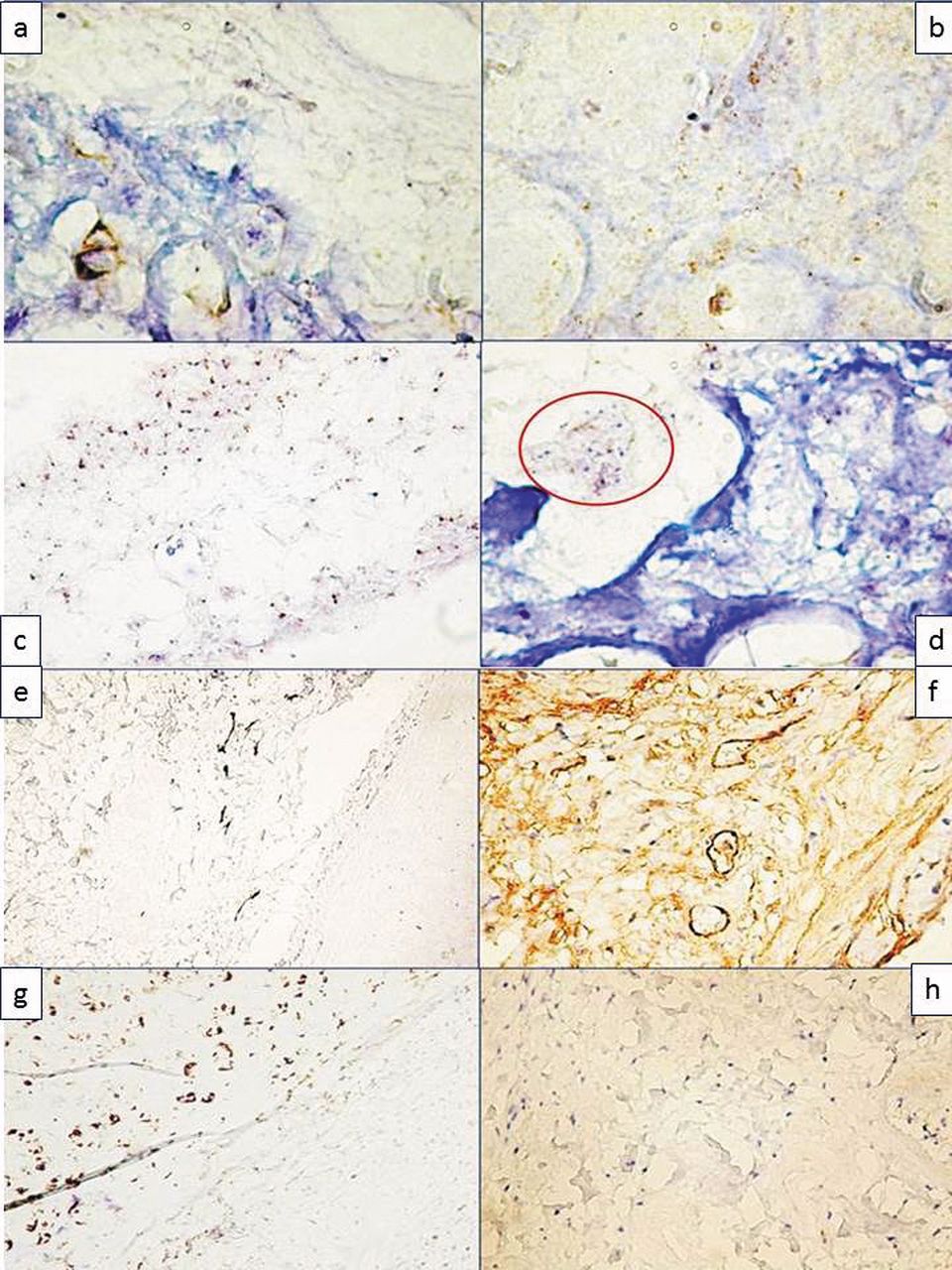
Degenerative changes of the cartilage implants were reported. Implanted cartilage tissue presented several canals -similar with cartilaginous canals from the embryonic development of the cartilage- located both at the peryphery and in the central part of the cartilage and filled with small perfused blood vessels (Figure 3c and 3d). Inside these blood vessels we were able to detect nucleated red blood cells specific for birds and absent in humans and also an increased number of inflammatory cells (Figure 3e). Nucleated red blood cells in the lumen of the blood vessels inside the cartilage confirmed that these blood vessels arised from pre-existing vascular network of the CAM through their aquisition induced by degenerative changes of the cartilage and, perhaps, under the influence of proangiogenic factors secretion, stimulated by this process. The lumen of this canal-like structure inside the unprotected cartilage implant was lined by elongated endothelial cells with flattened nucleus (Figure 3f and 3g) positive for F VIII-related antigen. Presence of high levels of proangiogenic factors was then certified by RNAscope in situ hybridization which detected condrocytes with high amplification levels of VEGF mRNA (Figure 4a and b). Focal loss of chondrocytes and invasion of the cartilage lacunae by the blood vessels and inflammatory infiltrate sustained degeneration of the implanted cartilage (Figure 4c and 4d).
Composite DC-F graft, protected by temporal fascia did not induce any histological changes in the chick CAM, this structure being similar with a normal chorioallantoic membrane with distinct epithelial and connective tissue components. No stromal changes were observed. Temporal fascia inhibited vascular network of the CAM and, also seemed to exert a protective effect on conchal cartilage. No blood vessels or inflammatory cells has been observed inside the cartilage from DC-F composite graft after 8 days post-implantation and, a positive reaction for D2/40 was strongly detected in the chondrocytes of DC-F composite grafts, certifying their viability, knowing that D2-40 is usually expressed in normal mature and functional chondrocytes.

Preliminary steps for chick embryo chorioallantoic membrane preparation for future cartilage and temporal fascia implants. By cutting the egg shell (a), we visualized the chick embryo viable CAM vessels (b) and continue to incubate until day 7 without any implant (c). Cartilage (d), temporal fascia (e), and composite graft DC-F (f) were removed from the saline solution and cut to obtain small pieces for CAM implants. On day 8 of incubation cartilage (g), temporal fascia (h) and composite graft DC-F were implanted on CAM as presented here.
Through immunohistochemistry we evaluated the presence and positive reaction for vascular, pro-angiogenic and anti-angiogenic markers. FVIII-positive small blood vessels were detected inside the chorioallantoic membrane, the outer part of temporal fascia and denudated cartilage and were absent in the cartilage tissue of the DC-F composite graft. No positive reaction for lymphatic markers Prox1 and D2-40 was observed for FGF nor for PDGF. A particular immunohistochemical aspect was observed for the expression of type IV collagen inside the temporal fascia. Its presence was detected both on the blood vessels basal membrane and also on dense connective tissue as a strong positive brown signal.
Discussion
Composite graft including diced cartilage wrapped in temporal fascia seems to be one of the best options for nasal augmentation or nasal reconstruction following tumor removal. Several types of cartilage (costal, nasal or conchal) have been proposed over the years for use as implants for nasal reconstruction combined or not with temporal fascia or fascia lata (15-17). The use of conchal cartilage-temporal fascia composite graft represents a relative new technique applied in nasal augmentation in our country (18). Despite the fact that post-surgical complications are rare, these events are often diagnosed as degenerative changes of the cartilage followed by its resorption or inflammation.

Cartilage implant produced an intense angiogenic effect macroscopically translated as “spoke wheel”, an arrangement of newly-recruited small blood vessels around the implant (a). These findings were confirmed by stereomicroscopy (b), showing small irregular and tortuous blood vessels being able to invade the cartilage. Macroscopic (c, d) and stereomicroscopic (e, f) view of temporal fascia inhibitory effects of CAM vascular network, 8 days after its graft. Note the lack of blood vessels compared to cartilage implant. Composite graft DC-F implant on CAM on first day (g) and 8 days after initial grafting (h). Note the evident differences between fascial side (h, red star) showing the inhibition of the CAM vessels and the right side of the implant (h, yellow star) with a well-defined vascular network rich in convergent small blood vessels. The same differences were confirmed by stereomicroscopy (i). At higher magnification, small blood vessels were found to invade the cartilage component of the composite graft (j).
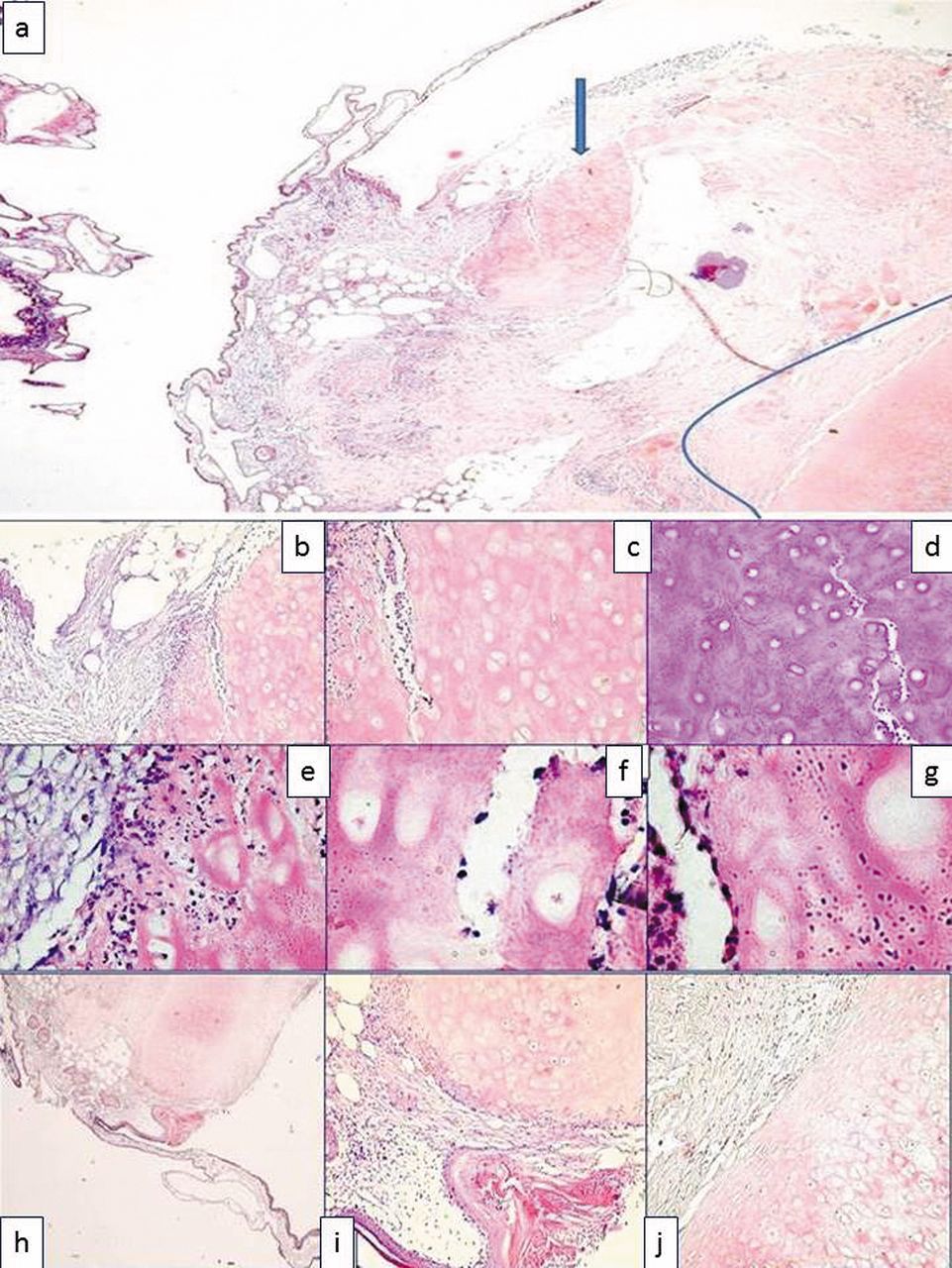
Histologic assessement of CAM implants. Cartilage implant (blue arrow) and composite graft DC-F implant (limited by blue line) on chick CAM (a). Detail from the periphery of the of cartilage implant (b) showing a dense stroma around it and invasion of the cartilage by the inflammatory cells and nucleated red blood cells inside the degenerated cartilage (c, d). Degenerated cartilage invaded by stromal components (e), and characterized by the presence of canal-like structures lined by endothelial cells (f, g). Composite graft DC-F implanted on CAM (h) did not produce inflammatory effects or stromal histologic changes, temporal fascia remained intact around the cartilage (i) and the cartilage kept its normal structure avoided by degenerative morphological changes (j).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Immunohistochemical and in situ hybridization evaluation of the implanted samples. High VEGF mRNA amplification was observed inside the chondrocytes (a) and to a lesser extent into the matrix (b) of degenerated cartilage invading also by CAM chorion (c, d) also with high amplification for VEGF mRNA. Scattered FVII-positive collapsed blood vessels on the outer layer of temporal fascia (e) and strong collagen IV-positive reaction for both vascular basal membrane and temporal fascia stroma are shown (f). D2-40 intensely stained chondrocytes (g, h) and was absent inside temporal fascia.
Histopathological features and molecular substrates of these post-operative unwanted events are even less characterized. Previous experimental models in mice and rabbits were used as hosts for composite graft implantation. Microscopic analysis of such grafts were usually performed after 2 to 6 month post-implantation and lacked monitoring of the dynamic early changes appeared immediately after implants (19-22).
A chick embryo chorioallantoic membrane model has not been previously used to study the behavior of implanted cartilage, temporal fascia and composite graft. Becasue of the direct visualization of the graft on the surface of chick embryo chorioallantoic we were able to observe and monitorize the early events following implantation of the cartilage, temporal fascia and composite graft DC-F.
Stromal-graft interaction was also evaluated with a high accuracy by using chick embryo CAM and we thus consider this experimental model to be superior compared to previously used mouse or rabbit models. The different morphological and molecular behaviour observed for the three types of implants in the present study could represent evidence explaining, in part, the failure of a small amount of nasal reconstructions using cartilage, temporal fascia or composite grafts DC-F.
The most common complication following rhinoplasties performed with cartilage grafts (associated or not with temporal fascia) is represented by cartilage resorption. One of the most accepted histopathological events concerning this complication is explained by chondrocyte degeneration followed by inflammatory cell invasion into cartilage tissue (23). Enhancement of inflammation around the cartilage implant not protected with temporal fascia can be explained by the presence of high content of podoplanin inside the chondrocytes, highlighted as an intense immunohistochemical reaction for D2-40 (24).
The results of the present study confirmed these previous findings and also enriched them by the description of an intense angiogenic process induced by cartilage implants not protected with temporal fascia. Aquisition of blood vessels by implanted conchal cartilage (known to be avascular in its normal, mature state) enhances cartilage degeneration being an important keyplayer of cartilage resorption pathogenesis observed for post-surgical complication following rhinoplasty. Similar aspects were previously described for degenerative events of inter-vertebral discs fibrous cartilage (25). VEGF seems to be the main trigger molecule for this angiogenic process as confirmed by our findings of high amplification levels for VEGF mRNA inside chondrocytes and matrix of cartilage implants non-protected by temporal fascia. VEGF expression in condrocytes and cartilage matrix still remains a controversial issue. Its presence in the developing cartilage from embryonic life (known to be highly vascularized) and its overexpression in osteoarthritic cartilage has been demonstrated (26). In the human mature cartilage VEGF is expressed in few condrocytes while VEGF-positive chondrocytes are grouped immediately below the perichondrum of a damaged portion from osteoarthritic cartilage (27).
We presented here first experimental evidence on conchal cartilage behavior after its harvesting for nasal reconstruction. High content of VEGF mRNA found in chondrocytes from the perypheric portion of implanted conchal cartilage without temporal fascia sustained condrocytes activation followed by VEGF overexpression and induction of the angiogenic cascade and cartilage vascularization. The angiogenic effect of VEGF is mainly supported by the absence of immunohistochemical positive reaction or lack of in situ hybridization amplification for other angiogenic factors, such as FGF or PDGF tested in the present study.
Plastic surgeons use blurring of the subcutaneous irregularities caused by diced cartilage used for this procedure, as the main argument for using temporal fascia in nasal reconstruction. Temporal fascia was initially used for face contour augmentation and then for composite grafts in rhinoplasty (28, 29) and tympanoplasty (30).
Temporal fascia histology includes two layers: the external one, less vascularized by blood vessels exclusively and the inner one, avascular with a high ability to adhere to any biological surface including conchal cartilage and favouring composite graft achivement (31). Except for scattered histological descriptions of temporal, no molecular aspects regarding this structure have been discussed before. Thus, no data regarding factors involved in the absence of blood vessels from the deep portion of temporal fascia have been reported.
Temporal fascia grafted on chick CAM did not aquire blood vessels from the host and, moreover, inhibited pre-existing vessels of the CAM. This preliminary finding represented the start-point to study angiogenic growth factors inside the deep portion of the temporal fascia implant. No positive reaction or mRNA amplification has been found for any angiogenic growth factor studied herein. This fact suggested the presence inside the fascia of a potential strong inhibitor of blood vessels and/or angiogenic process able to also diffuse and inhibit the vascular network of the CAM.
Lack of evidence for endostatin associated with a strong positive reaction for collagen IV inside the matrix of temporal fascia implanted on CAM, suggested a high content of tumstatin probably (Col IV α3 fragment of Col IV) known to have a high anti-angiogenic, pro-apoptotic and anti-inflammatory properties (32-35). This hypothesis is supported by the absence of inflammation around DC-F composite graft implanted on CAM and also by maintaining the cartilage surrounded by temporal fascia in an avascular state.
Several conclusions with a direct clinical impact on reducing post-surgical complications can be derived from the present study. The use of conchal cartilage protected by temporal fascia, such as DC-F composite graft represents, is in our opinion, the best choice to avoid degenerative changes of the cartilage following rhinoplasty. This is based on the anti-angiogenic protective effect exerted by termporal fascia as shown in our study. Also its anti-inflammatory properties enhance its protective role and reduce the rate of graft rejection. Absence or discontinuities of temporal fascia surrounding the conchal cartilage can activate the inflammatory and angiogenic cascade followed by stromal fibrosis, cartilage degeneration and failure of the nasal reconstruction.
Acknowledgements
First, second and the last Author had the same scientific contribution to the present work and can be considered all as principal authors of this article. We thank to Diana Tătucu for her excellent technical support.
- Received January 8, 2014.
- Revision received March 6, 2014.
- Accepted March 7, 2014.
- Copyright © 2014 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved