

Abstract
Aim: Strong evidence implicates chronic intraamniotic inflammation in the etiology of preterm delivery. The purpose of this study was to determine whether amniotic fluid IL-1β, IL-10 and IL-18 concentrations in women undergoing mid-trimester amniocentesis can identify those at risk for preterm labor or preterm rupture of membranes. Patients and Methods: A case-control study was conducted to compare mid-trimester concentrations of amniotic fluid IL-1β, IL-10 and IL-18 in women delivering at term or preterm. Out of 362 women included in the study, 38 presented with preterm labor. Thirty-eight women with term delivery, matched for chronological and gestational age served as controls. Women with abnormal fetal karyotypes or major anomalies were excluded. IL-1β, IL-10 and IL-18 concentrations were determined by ELISA. Conditional logistic regression was applied in the statistical analysis. Results: IL-1β was found to be positively and significantly associated with preterm delivery. Specifically, for every unit increase in IL-1β, women were on average 7.2 (OR: 7.2, CI: 1.94-26.77, p=0.003) times more likely to deliver preterm. IL-18 levels as well as gender were significantly associated with preterm delivery. Specifically, for every unit increase in IL-18, women were on average 1% less likely to have a preterm delivery (OR: 0.99, CI: 0.98-0.99, p=0.04). On the other hand, IL-10 was not significantly associated with preterm delivery. Conclusion: Mid-trimester IL-1β concentrations are positively associated with preterm delivery. Therefore, IL-1β, determined on the occasion of mid-trimester amniocentesis could possibly serve as a marker of preterm delivery. In contrast, IL-10 and IL-18 concentrations are not elevated in mid-trimester amniotic fluid and probably cannot serve this purpose.
- Preterm labor
- premature rupture of membranes
- cytokines
- prediction
- interleukins
- amniotic fluid
The incidence of preterm labor varies from 7-12.8% of deliveries (1, 2) and accounts for 75% of perinatal mortality and morbidity (e.g. blindness, deafness, developmental delay, cerebral palsy and chronic lung disease (3, 4). Although the etiology of preterm birth is multifactorial (5), the impact of intrauterine inflammation/infection is pronounced, being implicated in nearly 30% of cases (6). Inflammation/infection-associated preterm delivery is characterized by increased amniotic fluid concentrations of various cytokines (including IL-6, TNFα, ITAC, ADAM-8, beta-defensins) (7-11).
Interleukin 1-β (IL-1β) is a 17 kDa cytokine (12), produced by macrophages, monocytes and dendritic cells as a rapid response to bacterial antigen stimuli, and is a characteristic mediator of inflammation (13). IL-10 is an 18-kDa cytokine (14), capable of inhibiting the production of cytokines by activated Th2 cells (15). IL-18 shows structural homology with the IL-1 family of cytokines (16) and is synthesized by macrophages, monocytes, keratinocytes, and epithelial cells (17).
In this study, it was hypothesized that IL-1β, IL-10 and IL-18 might be implicated in the preterm delivery pathway and therefore, they could serve as possible predictors of the former. In this respect, their amniotic fluid concentrations were determined on the occasion of genetic amniocentesis and correlated them with preterm labor and/or premature rupture of membranes.
Patients and Methods
This was a prospective matched case-control study, performed in collaboration of the Second Department of Obstetrics and Gynecology, University of Athens and the Department of Fetal Medicine of ‘LITO’ Maternity Hospital in Athens, during the period September 2005 - December 2006. The study population consisted of Greek women with singleton pregnancies who presented for genetic amniocentesis. Women with twin pregnancies and women with known history of uterine abnormalities, cone biopsy, significant vaginal bleeding and fetal malformations were excluded from the study.
Preterm labor was defined as labor before 37 weeks of gestation with regular uterine contractions (at least two uterine contractions at a 10-minute interval during a 30-minute period) in combination with characteristic cervical changes (18). Preterm premature rupture of the fetal membranes was defined as the rupture of the amniotic membranes with amniotic fluid release more than one hour before the onset of preterm labor (19).
Gestational age was calculated from the date of last menstruation and was confirmed by routine ultrasound in the second trimester (16-19 weeks of gestation). Microbial invasion was defined as growth of any bacteria (aerobic or anaerobic) in the amniotic fluid cultures except for coagulase-negative Staphylococcus, (which was considered skin contamination) and/or positive PCR for Mycoplasma hominis and Chlamydia trachomatis. All patients were followed until delivery for the occurrence of pregnancy complications by their doctors. An independent investigator kept the medical records and entered maternal and perinatal data into a database. The Ethics Committee of the host teaching hospital approved the study. Each woman gave informed consent before enrolment in the study and completed a questionnaire regarding personal and family data.
Ultrasound-guided transabdominal amniocentesis with a 21-gauge needle was performed under aseptic conditions in 362 women during genetic amniocentesis. Amniocentesis was performed for advanced maternal age, and/or increased risk for aneuploidy during nuchal translucency ultrasound. The first 0.5 ml of collected amniotic fluid was discarded to avoid maternal contamination. A volume of 20 ml of amniotic fluid was aspirated from each woman (15 ml was used for genetic diagnosis). One ml of the uncentrifuged amniotic fluid was then transported immediately to the laboratory and cultured for aerobic and anaerobic bacteria. Another 1 ml of the uncentrifuged amniotic fluid was also tested by polymerase chain reaction (PCR) for Mycoplasma hominis and/or Chlamydia trachomatis detection. The remaining 3 ml of amniotic fluid were placed immediately in a refrigerator (+4°C) and were centrifuged within the next six hours at 3000 g and +4°C for 10 min. The supernatant was stored in polypropylene tubes at −80°C until analysis. Amniotic fluid IL-1β and IL-10 concentrations were determined by an enzyme-linked immunosorbent assay (ELISA) (IL-1β, IL-10 and IL-18 by Bender MedSystems GmBH, A-1030Vienna, Austria) while IL-18 concentrations were determined by an enzyme-linked immunosorbent assay (ELISA) (MBL, Naka-ku Nagoya, Japan) (sandwich ELISA technique). The amniotic fluid samples ran in duplicates. For IL-β, the intra-assay coefficient of variation (CV) was 6.7%, the inter-assay CV 8.1% and the detection limit 0.05 pg/ml. For IL-1β, the intra-assay CV was 5.61%, the inter-assay CV 6.25% and the detection limit 125 pg/ml. For IL-10, the intra-assay CV was 3.2%, the inter-assay CV 5.6% and the detection limit 1 pg/ml. (Intra- and inter-assay coefficients of CV refer to the laboratory characteristics of each kit used). Laboratory personnel were blinded to the clinical history of the women involved.
Statistical analysis. All data, except for age, gestational age at delivery and gestational age at amniocentesis, followed a normal distribution (Kolmogorov-Smirnov test). Independent samples t-test was applied to detect differences between groups where continuous variables were normally distributed. Otherwise, the Mann-Whitney U-test was applied. Pearson's χ2 test was used to detect differences between categorical variables.
Conditional logistic regression analysis was used to examine the possible associations of human IL-1β, IL-10 and IL-18 with preterm labor. Women with a preterm labor were defined as cases (N=38), while for each case a woman matched for age who delivered at term served as control (N=38).
Furthermore, subgroup analysis was conducted in order to examine any possible association of human IL-1β, IL-10, and IL-18 in women with preterm labor who delivered before 32 weeks of gestation (N=8 in each group). Finally, a subgroup of women who had preterm labor and premature rupture of membranes were evaluated (n=18 in each group). Results are presented as odds ratios (OR) and 95% confidence intervals (CI). Statistical analysis was performed by using SPSS 11.5 edition. A p-value of <0.05 was considered to be statistically significant.
Results
Out of the 360 women included in the study, 38 presented with spontaneous preterm delivery (incidence:10.56%), and out of that 38, 18 delivered after premature rupture of membranes (incidence: 5%). Ten women were excluded after amniocentesis because of fetal chromosomal abnormalities (two with trisomy 18, two with trisomy 21, one with Turner syndrome, one with Klinefelter syndrome and four with less common pathological karyotypes). Ten women were lost to follow-up. Four infants were delivered by caesarean section before the onset of labor for maternal (severe preeclampsia) or fetal reasons (compromised fetal growth or umbilical Doppler flow abnormalities). Two women who delivered within 30 days following amniocentesis were excluded from the study, as their delivery was considered related to the procedure of amniocentesis (20, 21).
The demographic data of the study population are presented in Tables I and II. No statistical significant differences were found in mean maternal age, gestational age at amniotic fluid sampling and parity between the groups of women delivering preterm and at term. Amniotic fluid cultures for common bacteria in the participating mothers were negative, while Mycoplasma hominis and Chlamydia trachomatis were identified in 2/338 and 2/338, respectively. However, one of the two women with Mycoplasma hominis and one of the two women with Chlamydia trachomatis delivered preterm. No correlation was found between PCR detection of Mycoplasma hominis and/or Chlamydia trachomatis with preterm labor prediction.
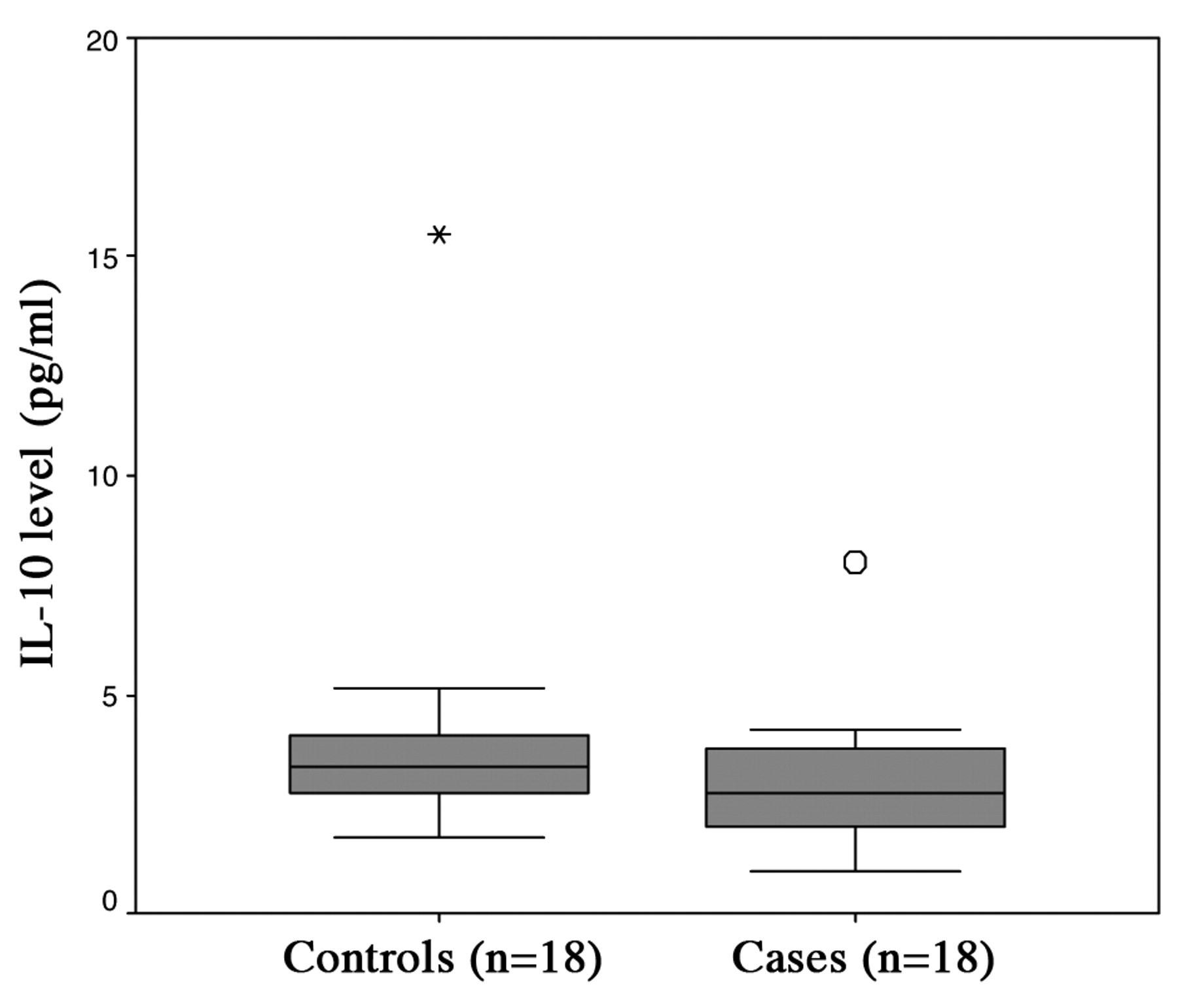
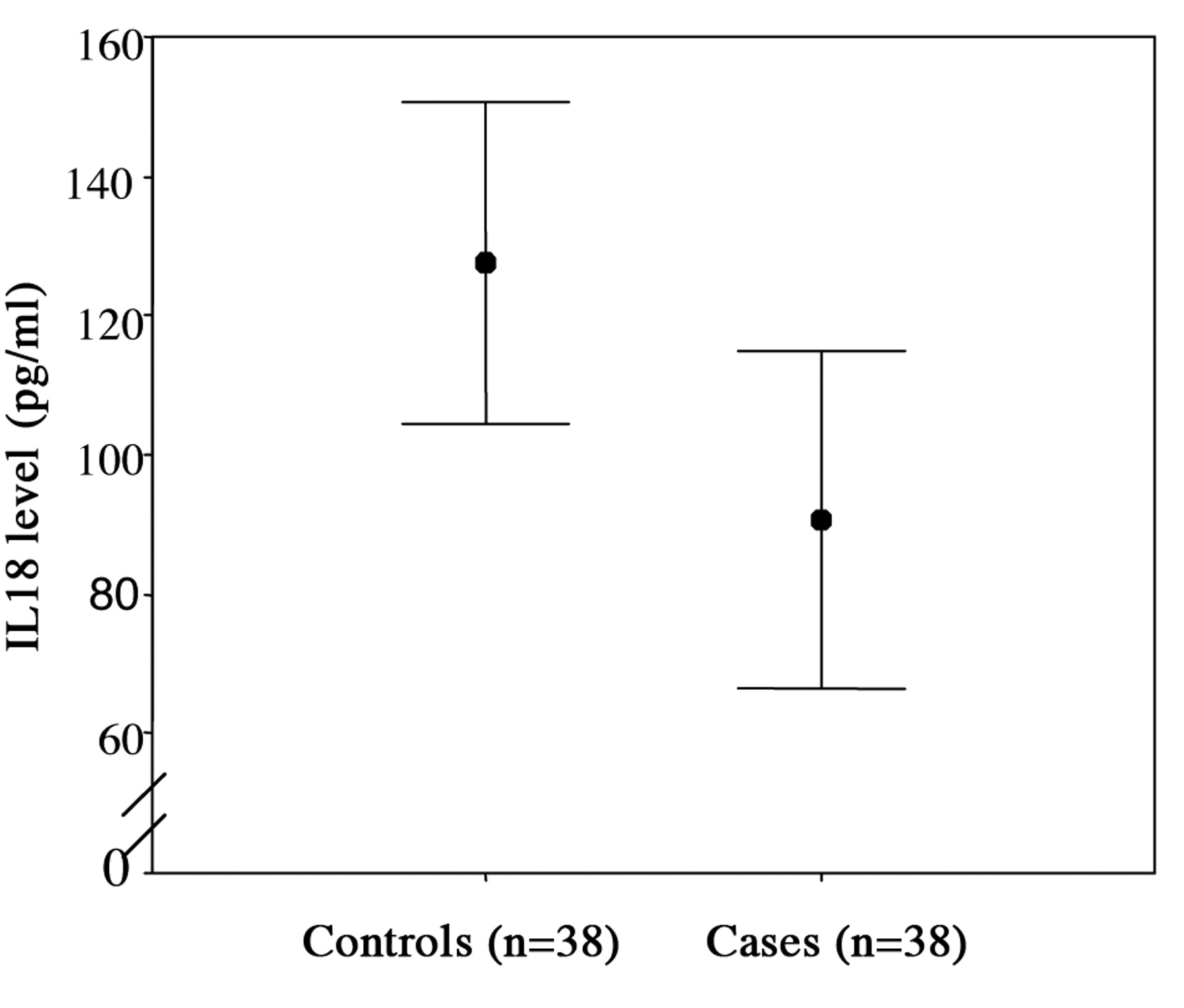
IL-1β, IL-10, IL-18 concentrations in cases of preterm delivery (n=38) and controls (n=38), as well as in cases of premature rupture of membranes (n=18) and controls (n=18) are presented in Tables III and IV, respectively. IL-1β was found to be positively associated with preterm delivery and this association was statistically significant. Specifically, for every unit increase in IL-1β women were on average 7.2 times more likely to have a preterm delivery (OR: 7.2, CI: 1.94-26.77, p=0.003) (Figure 1). IL-18 levels, as well as gender, were significantly associated with preterm delivery. Specifically, for every unit increase in IL-18 women were on average 1% less likely to have a preterm delivery (OR: 0.99, CI: 0.98-0.99, p=0.04) (Figure 2). Furthermore, women who delivered female neonates were 84% less likely to have a preterm delivery as compared to women who delivered males (OR: 0.16, CI: 0.40-0.71, p=0.016). IL-10 was not found to be significantly associated with preterm delivery (Figure 3).
Demographic data for women with preterm labor who delivered before 37 weeks of gestation (cases, n=38) and women delivering at term (controls, n=38).
Demographic data for women with preterm labor and premature rupture of membranes (cases, n=18) and women delivering at term (controls, n=18).
IL-1β, IL-10, IL-18 concentrations in cases of preterm delivery (n=38) and controls (n=38).
IL-1β, IL-10, IL-18 concentrations in cases with premature rupture membranes (n=18) and controls (n=18).
In the subgroup of women with preterm labor who delivered before 32 weeks of gestation, IL-1β, IL-10 and IL-18 were not found to be significantly associated with preterm delivery. IL-10 and IL-18 were not found to be significantly associated with preterm delivery in this sub-analysis.
Discussion
The results of this study indicate that amniotic fluid IL-1β concentrations are positively associated with preterm delivery, as well as preterm premature rupture of membranes. It has been previously documented that IL-1β is produced by epithelial cells of the amnion, chorion, syncytiotrophoblast and decidua (22) as a procytokine molecule, cleaved by caspase-1 into its active form (23). Moreover, it has been shown that high levels of IL-1β are present in amniotic fluid samples with detectable bacteria (24). For the participating mothers in the current study, amniotic fluid cultures for common bacteria were negative, while Mycoplasma hominis and Chlamydia hominis were only identified in 2/338 and 2/338, respectively.
IL-1β is an important regulator of myometrial CRH-receptor-1 gene expression, a fact that might play a role in the uterine change from quiescence to contractility and labor (25, 26). It also indirectly increases oxytocin secretion in primary cultures of human deciduas through the cyclo-oxygenase-2 pathway (27) and modulates calcium mobilization from intracellular stores preparing the pregnant uterus for labor (28). IL-1β also enhances MMP-1 and MMP-3 expression in decidual cells, possibly leading to premature membrane rupture (29).

Box and whisker plots of the concentrations of IL-1β from women with spontaneous preterm delivery who delivered before 37 weeks of gestation (cases) and women with full-term deliveries. Each box represents the median concentration with the interquartile range (25th and 75th percentiles).
It has been shown that the major source of IL-10 is activated Th2 cells (30). However, other cells have also been implicated in IL-10 production, including Th1 (31), stimulated B-cells (32), LPS-activated monocytes (33), macrophages (34), dendritic cells (34, 35) and regulatory T-cells (36). Gestational tissues such as cytotrophoblast (37), syncytiotrophoblast (37), chorion (38) and decidua (39, 40), express IL-10 mRNA (41, 42) and produce IL-10. IL-10 is a pleiotropic anti-inflammatory cytokine (30, 43) acting in the down-regulation of the immune response (23) by inhibiting the IL-1β, IL-6 and PGE2 production by choriodecidua (44). Nevertheless, IL-10 enhances production of cytokines and matrix metalloproteinases within the amnion (45). IL-10 also acts as an anti-inflammatory cytokine in the placenta (42, 46) by inhibiting the production of inflammatory cytokines such as IFN-γ, IL-1α, IL-1b, GM-CSF, G-CSF, TNFα, IL-6, IL-8 and IL-12 β (34). More specifically, the effects of IL-10 in fetal membranes depend on the precise tissue site. It inhibits cytokine production and matrix metalloproteinase expression in the choriodecidua (47). Furthermore, in rats, exogenously administered IL-10 attenuates fetal loss and growth restriction induced by LPS (48), whereas exogenous IL-10 has been shown to block intrauterine contractions in monkeys (49). Moreover, IL-10 has been shown to prolong gestation and to diminish fetal demise in a rat model when administered alone or in combination with antibiotics (50). For this reason IL-10 administration has been proposed as an anti-inflammatory agent in the treatment of preterm labor (49, 51).

Mean concentrations of IL-18 from women with spontaneous preterm delivery who delivered before 37 weeks of gestation (cases) and women with full-term deliveries. Error bars represent the 95% CI.
IL-10 has been detected in the amniotic fluid during the second trimester of pregnancy (23), however, controversial findings relating to its concentrations throughout pregnancy have been reported (52). Gotsch et al. (23) showed that IL-10 is detectable in amniotic fluid and that its median levels do not change throughout pregnancy from mid-trimester to term. In contrast, Grieg et al. showed that amniotic fluid IL-10 concentrations increase throughout pregnancy and are elevated in patients with preterm labor associated with intrauterine infection (53). However, no differences in IL-10 concentrations have been documented in cases with preterm or term labor, or in cases with chorioamnionitis (54). Jones et al., using monolayer decidual cultures, reported that basal decidual IL-10 production rates did not change significantly with the onset of labor (55). In contrast, Simpson et al. (56) showed that the basal production of IL-10 by choriodecidual explants decreases after labor onset. This finding might be associated with the increase in the production of IL-6 and PGE2 (56). To the Authors' knowledge the current study is the third investigating the role of mid-trimester amniotic fluid IL-10 concentrations as a possible predictor of preterm labor. No statistically significant association with preterm delivery was found in this study.
IL-18 is a physiological constituent of amniotic fluid, maternal plasma and cord blood and its levels increase with advancing gestational age (57). Sources of IL-18 during pregnancy include the chorion and the decidua, as IL-18 mRNA is expressed in the choriodecidual interface, but not the amnion (58). IL-18 has a critical role in host defense by providing a cervical/decidual barrier against microbial invasion of the amniotic fluid (59). Its proinflammatory properties are based on the promotion of nuclear translocation of NFκB (58), the production of TNF-α, IFN-γ and IL-1β (17, 60) and the induction of both Th1 and Th2 response (61). IL-18 acts on macrophages and induces a response in order to enhance the immune response of the chorioamniotic membranes (62). More specifically, IL-18 activates the Th1 response by inducing IFN-γ production in T-cells, as well as NK cells (63). Moreover, IL-18 is a pro-apoptotic cytokine. IL-18 can increase cell membrane associated Fas expression and induce FasL, which will bind to Fas. This leads to intracellular signaling which facilitates procaspase-8 to its active form. This active caspase-8 is an effector for other caspases and leads to proteolysis and programmed cell death or apoptosis (58).
{kind=link}
{kind=link}
{kind=link}
Box and whisker plots of the concentrations of IL-10 from women with spontaneous preterm delivery who delivered before 37 weeks of gestation (cases) and had premature rupture of membranes and women with full-term deliveries. Each box represents the median concentration with the interquartile range (25th and 75th percentiles).
Amniotic fluid IL-18 was found to be significantly associated with histological chorioamnionitis in patients with preterm labor, whereas in premature rupture of membranes the results are controversial (58, 64). In animal models, the enhanced preterm labor rate was associated with decreased IL-18 (16). Moreover, it has been shown that there is a correlation between low levels of IL-18 in maternal serum and preterm labor. It has also been shown that cervical and amniotic fluid IL-18 levels are significantly higher in women in preterm labor when compared with women at term who are not in labor (59). The levels of IL-18 were higher in cases with microbial invasion (59). In the current study, no statistically significant association of IL-18 with preterm delivery was identified.
In conclusion, elevated amniotic fluid IL-1β levels at the time of mid-trimester genetic amniocentesis might possibly serve as a predictive factor for preterm labor, with or without premature rupture of membranes. Future studies should further elucidate the possible roles of IL-1β, IL-10, IL-18 in the preterm labor pathway.
- Received September 28, 2010.
- Revision received October 26, 2010.
- Accepted October 28, 2010.
- Copyright © 2011 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved