

Abstract
Background: Morbid obesity is frequently accompanied by serious co-morbidity, enclosed obstructive sleep apnea and hypoventilation syndrome, and thus many morbidly obese patients require surgical interventions. The aim of this study was to evaluate the relationship between arterial oxygen (pO2) and carbon dioxide (pCO2) partial pressure, age, loss of excess weight, and body mass index (BMI) in obese patients scheduled to undergo bariatric surgery. Patients and Methods: A group of 11 patients (4 men, 7 women, median age 38 years, range 23-58 years) with extremely severe obesity (BMI>50 kg/m2) underwent laparoscopic Roux-en-Y gastric bypass. Preoperatively, BMI, pO2, and pCO2 were 52.7±2.4 kg/m2, and 70.9±5.3 and 43.1±6.5 mmHg, respectively. Hypoxemia (pO2<75 mmHg) was present in all patients, but no relationship between BMI and age (R=−0.24, p=0.44) or between BMI and pO2 (R=0.09, p=0.77) was found. Results: As expected, there was a significant correlation between age and both pO2 (R=−0.58, p=0.04) and pCO2 (R=0.85, p=0.0004), while no relationship between BMI and age (R=−0.24, p=0.44), nor between BMI and pO2 (R=0.09, p=0.77) was found. Finally, there was a significant correlation between pO2 and loss of excess weight (R=−0.69, p=0.02). No intra- or postoperative complications were observed, and 12 months after surgery BMI decreased to 32.5±2.7 kg/m2 (p<0.001) and pCO2 to 37.9±5.3 mmHg (p=0.05), while pO2 reached 85.8±6.8 (p<0.001) mmHg. Conclusions: In obese patients, the severity of hypoxemia is mainly related to age. The amount of weight reduction, rather than lower baseline BMI values, may justify the significant postoperative pO2 improvement.
- Obesity
- hypoxemia
- bariatric surgery
- gastric by-pass
- body mass index
- excess weight
Obesity is a multifactorial disorder which produces a number of complications and metabolic sequelae, including risk of severe cardiovascular diseases and respiratory diseases (1). The prevalence of obesity in Western countries is increasing. In the USA, one third of the population is obese, and two thirds are overweight (2). The term ‘morbid obesity’ has been used to emphasize the severe health risks of having a body weight above 150 kg (1). Morbid obesity is frequently accompanied by serious co-morbidity, enclosed obstructive sleep apnea and hypoventilation syndrome, and thus many morbidly obese patients require surgical interventions.
The aim of this study was to evaluate the relationship between arterial oxygen partial pressure (pO2) and carbon dioxide partial pressure (pCO2), age, loss of excess weight, and body mass index (BMI) in severe obese patients scheduled to undergo bariatric surgery.
Patients and Methods
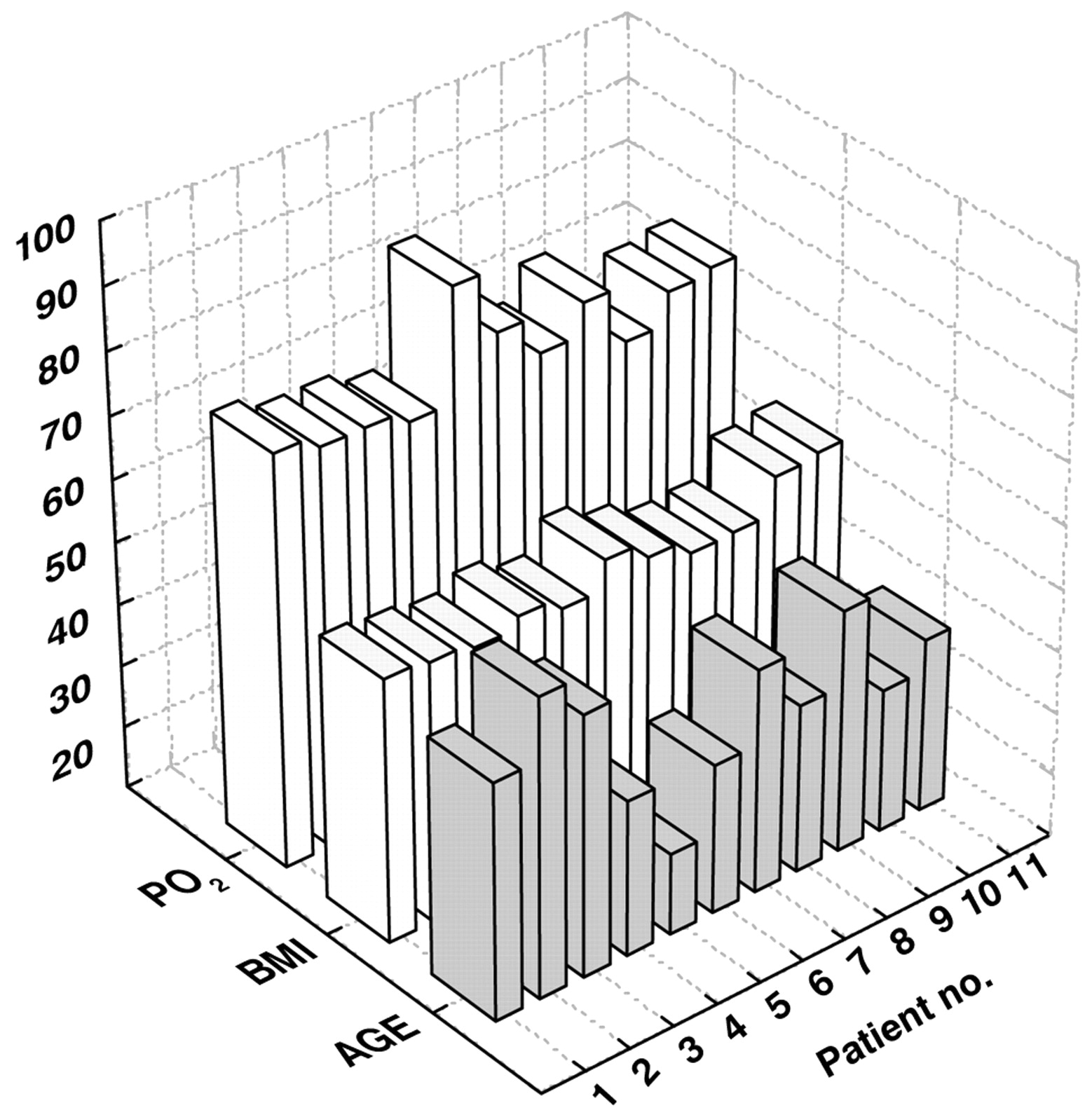
Study population. A group of 11 patients (4 men, 7 women, median age 38 years, range 23-58 years) with extremely severe obesity (BMI>50 kg/m2) underwent laparoscopic Roux-en-Y gastric bypass. This operation combines the creation of a small gastric pouch with bypassing a portion of the upper small intestine, stapling the upper stomach, and creating an outlet to the downstream small intestine (3, 4). Preoperatively, the mean BMI, pO2, and pCO2 were 52.7±2.4 kg/m2, 70.9±5.3 mmHg and 43.1±6.5 mmHg, respectively. Hypoxemia (pO2<75 mmHg) was present in all patients. Figure 1 shows the age baseline BMI and pO2 values of each patient. These parameters were measured 12 months after operation. Informed consent was obtained from all participants to review their clinical data, in accordance with the Institutional Review Board approval. There was no conflict of interest between the authors.
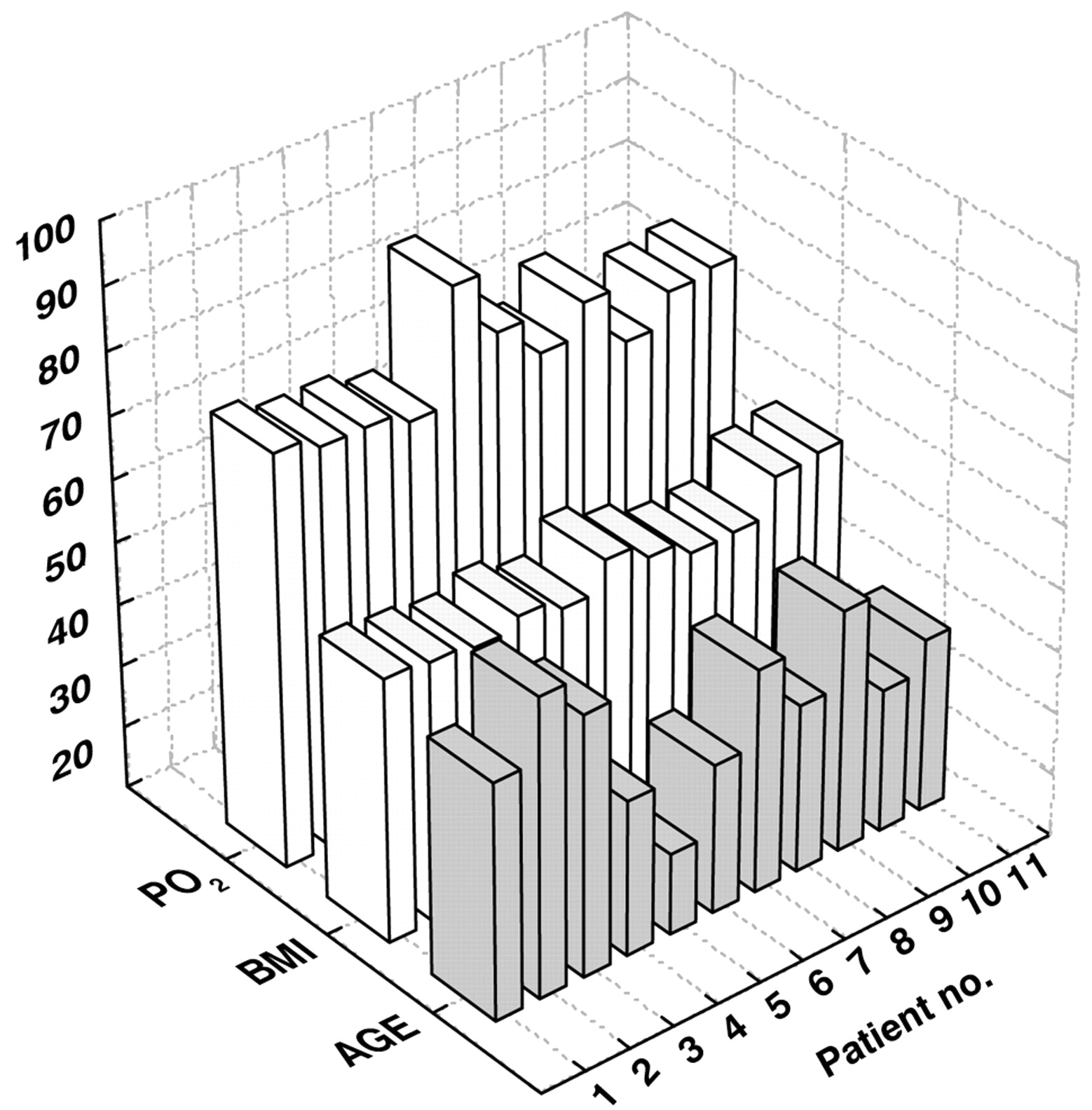
Age, and baseline body mass index (BMI) and pO2 value of the patients.
Statistical analysis. The reported data are expressed as the mean±standard deviation (SD). Comparisons between groups were performed using the Mann-Whitney U-test and Student's t-test. Pearson's correlation coefficient (R) calculation was used to evaluate the linear relationship between pairs of variables. A p-value <0.05 was considered statistically significant.
Results
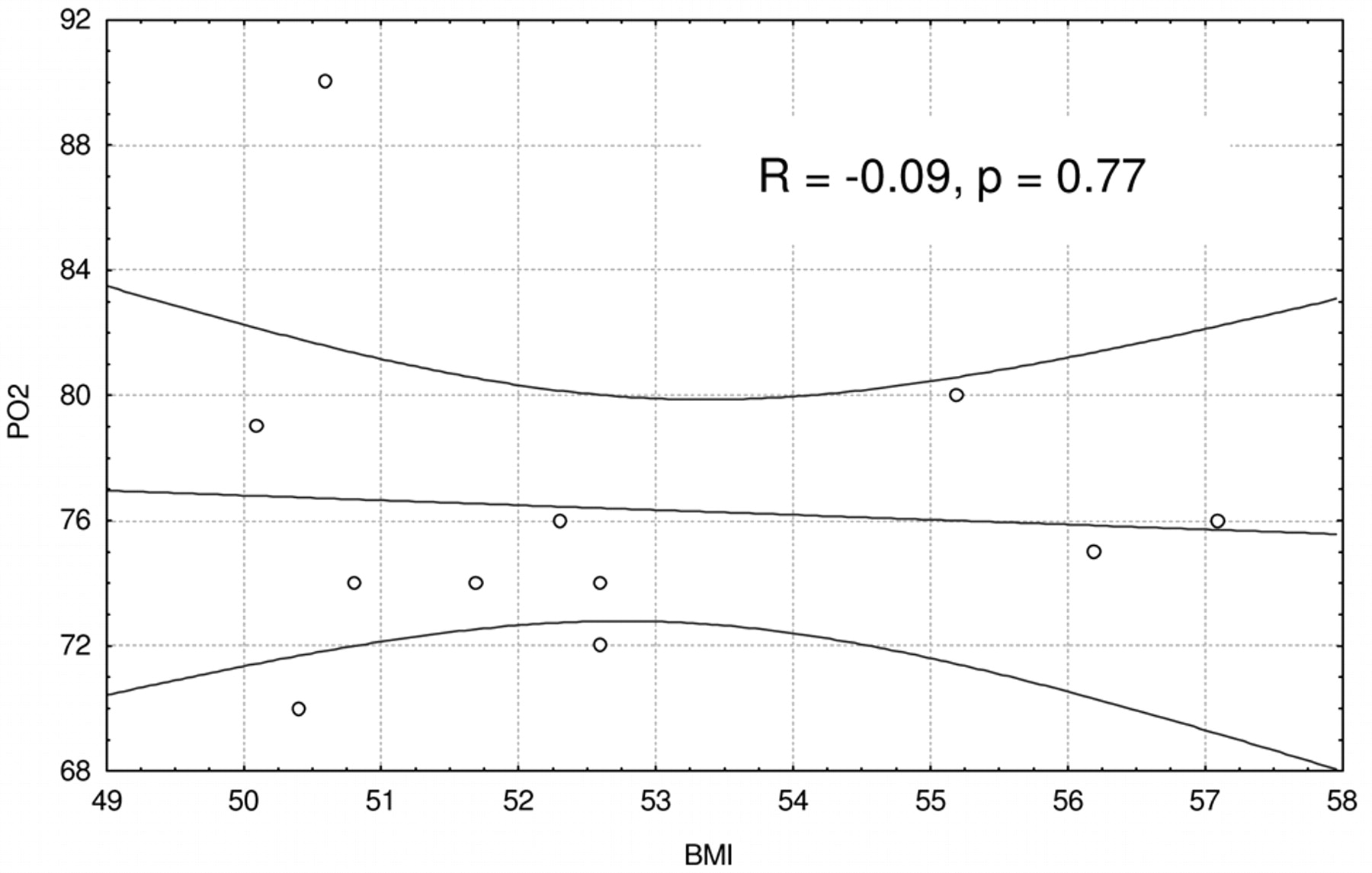
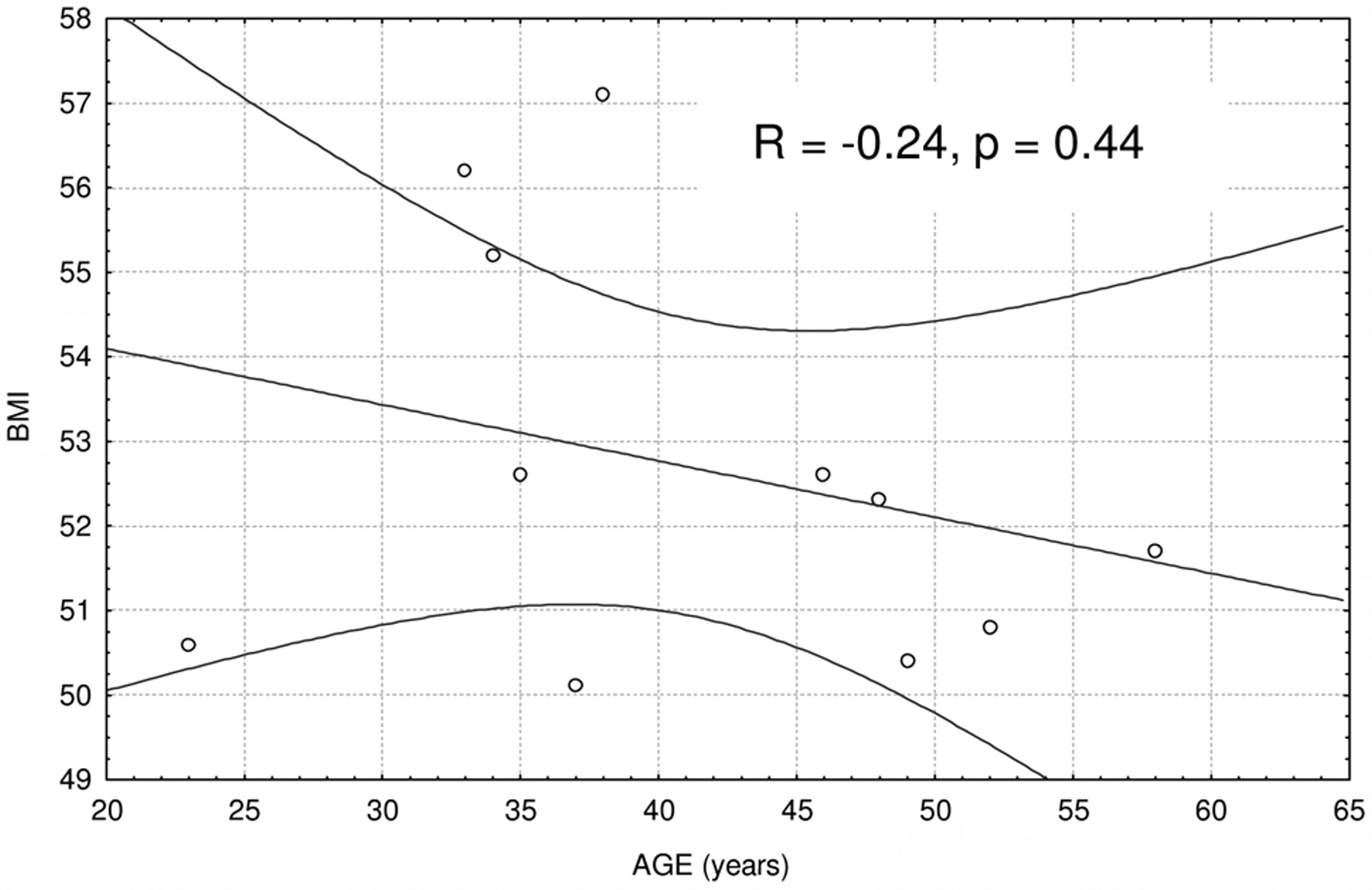
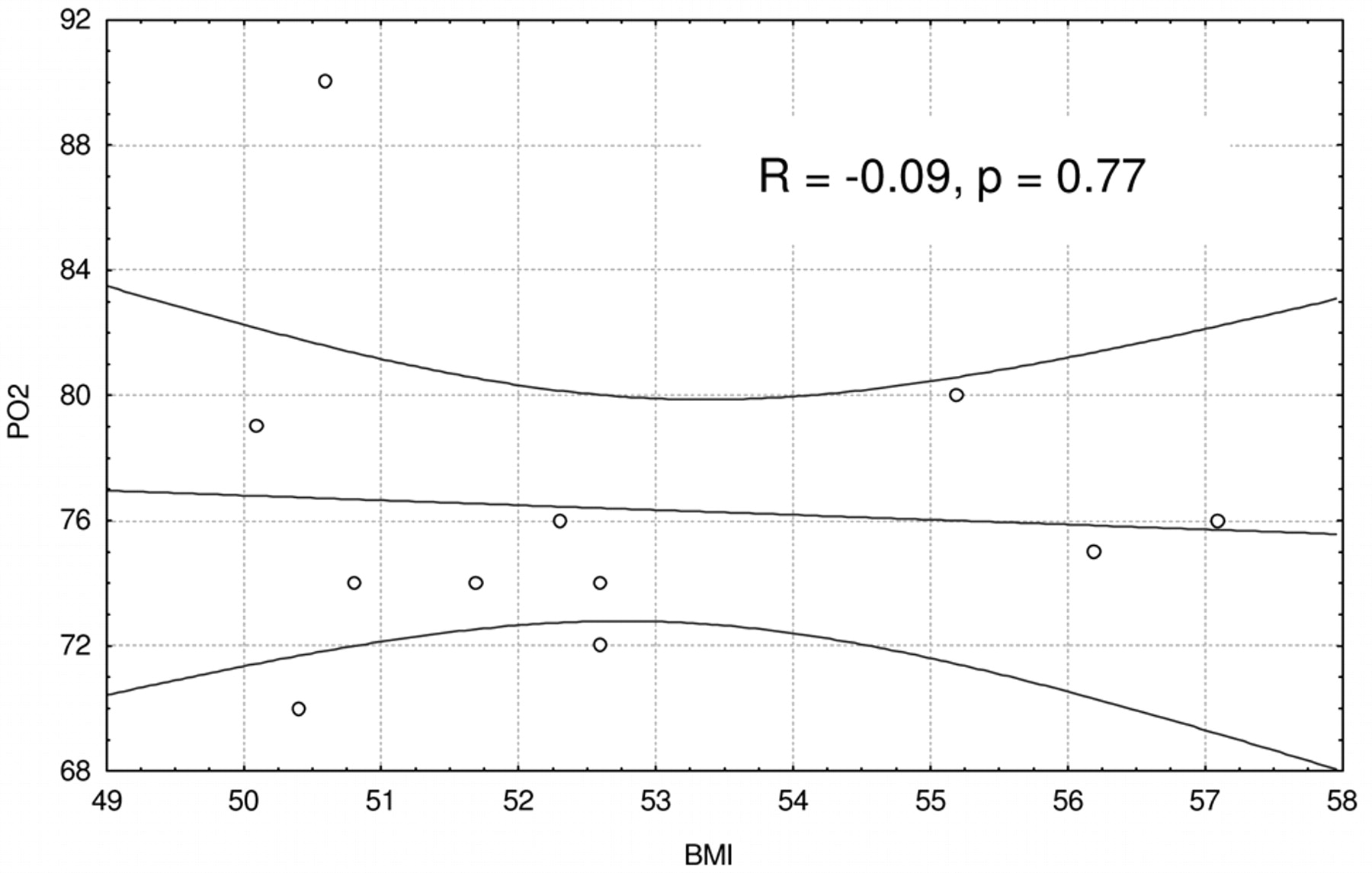
No intra- or postoperative complications were observed. As expected, there was a significant correlation between age and both pO2 (R=−0.58, p=0.04) and pCO2 (R=−0.85, p=0.0004). No relationship between BMI and age (R=−0.24, p=0.44), nor between BMI and pO2 (R=0.09, p=0.77) was found (Figures 2 and 3), while there was a significant correlation between pO2 and loss of excess weight (R=−0.69, p=0.02). Table I reports preoperative and postoperative (12 months) BMI, pO2, and pCO2 values. Both BMI and pO2 significantly (p<0.001) improved postoperatively, while at one-year follow-up a decrease of BMI of 38.3% was observed, and the reduction of pCO2 was not significant (p=0.053).
Discussion
The BMI is at present the recommended basis for classifying overweight and obesity (1). Other measures of obesity include waist circumference (a surrogate marker of visceral fat), skinfold thickness, bio-electric impedance, and body fat distribution by computed tomography (CT) or magnetic resonance imaging (MRI) scans. Comorbidities of morbid obesity (BMI>40 kg/m2) mainly consist of cardiovascular diseases, diabetes mellitus, respiratory diseases, and gastroesophageal reflux (5-7).

Relationship between age and body mass index (BMI).
{kind=link}
{kind=link}
{kind=link}
Relationship between body mass index (BMI) and pO2.
Obese patients with hypoventilation display blunted respiratory responses to hypoxia, developing hypoxemia due to decreased ventilation. Weight loss of 5% to 10% has been associated with marked reductions in the risk for these chronic diseases and with a reduced the incidence of diabetes (4).
The increased incidence of morbid obesity has resulted in an increase in bariatric surgical procedures (8). The gastric bypass, firstly described in 1967 by Mason and Ito (3), represents the most commonly performed weight loss procedure, and more than half of gastric bypasses are done laparoscopically (4, 9).
Roux-en-Y gastric bypass significantly improves BMI, and weight loss obtained by bariatric surgery is associated with significant long-term improvements in obstructive respiratory syndrome and oxygenation (10-14). In our patients with extremely severe obesity, both preoperative and postoperative hypoxemia was related to age. One year after the gastric bypass, a significant improvement of hypoxemia, together with a reduction of pCO2, were observed, and the results were independent of age.
Main clinical and biochemical data (mean±standard deviation).
It is well known that ventilatory responsiveness is attenuated in patients with obesity hypoventilation syndrome (15, 16). Moreover, several studies showed that weight loss was associated with marked improvement in pulmonary function, decreasing pCO2, and expanding lung volume (17-19). We did not find any relationship (p=NS) between pO2 and BMI nor between pCO2 and BMI.
Conclusion
In obese patients, the severity of hypoxemia is mainly related to age. In a previous report, we found that bariatric surgery significantly improves spirometric parameters (20), while the present study showed that the amount of weight reduction, rather than lower baseline BMI values, may justify the significant postoperative improvement in pO2.
Acknowledgements
This work was presented at the conference “Hypoxia and Consequences: From the Molecule to Malady”, held at the New York Academy of Sciences, New York, NY (USA), March 12-14, 2009.
Footnotes
-
* Presented at the conference “Hypoxia and Consequences: From the Molecule to Malady”, held at the New York Academy of Sciences, New York, NY (U.S.A.), March 12-14, 2009.
- Received March 31, 2010.
- Revision received June 18, 2010.
- Accepted August 28, 2010.
- Copyright © 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved