

Abstract
Background: The aim of the study was to determine how tidal volumes may affect the lung and haemodynamics during mechanical ventilation. Materials and Methods: With the approval of the Ethics Committee, the study included a total of 24 healthy piglets, average weight 30 kg (range 28-33 kg). The animals were ventilated for 90 minutes under general anaesthesia with two different tidal volume strategies and allocated into three groups. Group A, animals were healthy controls, Group B, animals comprised 8 piglets with an abdominal aortic aneurysm and ventilated with a low tidal volume strategy (VTexp 7ml/kg). Group C comprised 8 animals seven days after kidney transplantation, ventilated with a high tidal volume strategy (VTexp 12 ml/kg). Changes in lung mechanics and hemodynamics were assessed at 30th and 90th minutes. Lung tissue samples were examined histologically. Results: Protective ventilation in Group A and B did not confer any haemodynamic and lung mechanic differences. Significant differences were only found in Group C at 90 minutes for increased preload of both heart ventricles (CVP; t-test 4.07, p<0.01 and PAoP; t-test 8.43, p<0.01), pulmonary vascular resistance (t-test 3.11, p<0.05), and decreased expiratory tidal volume (t-test 6.07, p<0.01), dynamic lung compliance (t-test 3.83, p<0.01) and cardiac output (t-test 2.07, p<0.01). Diffuse alveolar damage was detected histologically. Conclusion: Mechanical ventilation at high tidal volumes reaching 12 ml/kg caused functional changes in the lungs, diffuse alveolar damage and reduction of cardiac output within 90 minutes.
- Diffuse alveolar damage
- haemodynamics
- mechanical ventilation
The concept of the present study arose from routine clinical practice in paediatric intensive care medicine. The aim of the study was to establish how raised tidal volumes may cause complications. As it would not be ethical to knowingly expose critically ill children to inappropriate ventilation strategies, and hence unwanted complications, we decided on an experimental study (1). The cardiopulmonary anatomy and physiology of a medium-sized domestic pig is comparable to those of humans (2). Piglets with surgical imposed alterations in haemodynamics were deemed appropriate as a functional biomodel for the purposes of the study. Similar to critically ill children, these animals were burdened with increased systemic vascular resistance before mechanical lung ventilation was started (3).
The aim of the present study was to assess the effect of the different tidal volume strategies on lung damage and haemodynamics. Concurrently, we verified whether a high tidal volume ventilation strategy influences the lung mechanotransduction and inflammatory response of the organism. In this work, we compared the effects of low and high tidal volume on the selected indicators.
Materials and Methods
The study was conducted with the approval of a multidisciplinary institutional Ethics Committee in the Czech Republic and EU, with compliance to the rules of the Helsinki Declaration 1975 (revised in 2004) and the European Communities Council Directive of 24 November 1986 (86/609/EEC) at the accredited experimental laboratory of the Faculty of Medicine in Pilsen, Czech Republic.
Experimental model. Twenty four clinical healthy piglets (9 weeks old; breed stained black pig; mean weight 30 kg, range 28-33 kg; male to female ratio 1:2) were mechanically ventilated for 90 minutes under general anaesthesia and neuromuscular block in a conventional pressure-controlled regime, and allocated to three equal groups: A, B and C.
Control group A comprised eight piglets without previous surgery, ventilated with constantly adjusted parameters to maintain an expiratory tidal volume value of 7 ml/kg throughout the study. Initial ventilatory settings were: respiratory rate (RR) 25 breaths/min, inspiration time (Tinsp) 0.8 s, average inspiration pressure (Pinsp) 18 cmH2O, positive end-expiration pressure (PEEP) 5 cmH2O, fraction of inspired oxygen (FiO2) 0.3. Group B included eight animals with an experimental abdominal aortic aneurysm that was created by the tourniquet technique 3 weeks before induction into the study (3). Echocardiographic imaging confirmed a 20% reduction in left ventricular performance before commencement of the study. The piglets were ventilated with identically ‘protective’ settings to achieve an expiratory tidal volume of 7 ml/kg: RR=25 breaths/min, Tinsp=0.8s, Pinsp=18 cmH2O, PEEP=5 cmH2O, FiO2=0.3. As part of the study protocol, 8 animals forming Group C received cyclosporine A (Sandimmun Neoral, 10.0 mg/kg) and methylprednisolone (Solu-Medron, 4.0 mg/kg) intravenously prior to orthotopic transplantation (4, 5). Seven days after kidney transplantation these animals were ventilated with constantly adjusted ‘injured’ settings to achieve an expiratory tidal volume value of 12 ml/kg: RR= 25 breaths/min, Tinsp=1.2s, Pinsp=30 cmH2O, PEEP=5 cmH2O, FiO2=0.3.
Data obtained at time-1 and comparison of group B and C with group A (n=24).
Animal preparation, haemodynamic monitoring, and ventilator support. Premedications were performed via intramuscular administration of atropine 0.07 mg/kg and azaperone 5.0 mg/kg. General anaesthesia was induced by intravenous administration of thiopental 10 mg/kg and all animals were tracheally intubated. General anaesthesia was maintained with combination of ketamine 1.5-2.0 mg/kg, fentanyl 0.5-1.0 microg/kg, azaperone 3.0-4.0 mg/kg, and neuromuscular block by pancuronium 0.1-0.2 mg/kg intravenously (6). Cardiac output was measured by the intermittent thermodilution method using a pulmonary artery catheter. Under ultrasound guidance, a Swan-Ganz thermodilution catheter was positioned in the pulmonary artery. An average body core temperature of 38.5°C was measured in the pulmonary artery allowing for adequate thermal differences with the test solution (0.9M sodium chloride at 21°C). Standard techniques were used to assess cardiac output by rapid injection of test solution into the proximal port of the pulmonary artery catheter and subsequent temperature monitoring at the catheter tip (7). The femoral artery was used for direct arterial blood pressure monitoring via a percutaneous catheter. Calculated and recorded standard haemodynamic parameters measured were: heart rate (HR; beat/min), stroke volume (SV; ml), cardiac output (CO; l/min), cardiac index (CI; l/min/m2), and the mean value of pressures: systemic arterial (MAP; mmHg), central venous/right atrial (CVP/RAP; mmHg), the right ventricle (RVP; mmHg), pulmonary artery pressure (PAP; mmHg) and pulmonary artery occlusive pressure (PAoP; mmHg), pulmonary vascular resistance (PVR= [PAP–PAoP]×80/CO; dyn/cm5), and systemic vascular resistance (SVR=[MABP – CVP]×80/CO; dyn/cm5). Body surface area was calculated using the following formula: 0.087 × weight/0.66 (BSA; m2) (7-8). Each parameter was expressed as the mean value from 5 consecutive measurements at 30-second intervals.
Animals in all groups were ventilated using permanent positive pressure and pressure controlled mode (Siemens Elema 900C, Germany). Ventilator adjustment included: RR (breath/min), Tinsp (s), and Pinsp (cmH2O), positive end-expiration pressure (PEEP; cmH2O), and FiO2. Standard parameters of dynamic lung mechanics were always taken at the 30th (time-1) and 90th minute (time-2) of the study: peak inspiration pressure (PIP; cmH2O), mean airway pressure (Paw; cmH2O), inspiratory/ expiratory tidal volume (VTinsp/exp; ml/kg), minute respiratory volume (MV; l/min), and dynamic lungs compliance (Cdyn; ml/cmH2O).
For the purposes of the study and evaluation of lung mechanotransduction and systemic inflammatory reaction induction, the levels of intercellular activated lymphocytes cell adhesion molecules-1 (ICAM; ng/ml), and the cell adhesion molecule-1 activated by the vascular endothelium (VCAM; ng/ml) in plasma were selected. Animal blood samples were processed by staff blinded to the test subjects using the human serum kits (Human sICAM-1 Instant ELISA and Human sVCAM-1 Instant ELISA; Bender Med Systems, Vienna, Austria). Standard accepted reference values were taken as: ICAM-1 4.94±0.005 ng/ml, VCAM-1 8.49±0.05 ng/ml (4, 5).
Tissue samples were carefully obtained by surgical excision from both dorsobasal lung lobes of the animals. The sampled tissue was immediately fixed with a 10% buffered solution of formaldehyde, histologically processed, and dyed with eosine. Using a double-blind test method, the preparations were examined with an optical and electron microscope.
Protocol of the study. Following instrumentation of each animal, measurement of dynamic lung mechanics and haemodynamics were performed in each animal after a 30-minute recovery period (time-1) and again at the 90th minute (time-2). Blood samples were taken from all the piglets at time-1 and -2 to quantify cell adhesive molecules (CAMs) in plasma. Under continued general anaesthesia a thoracotomy was performed, photographic evidence taken, and samples of lung tissue for histological processing were obtained carefully by excision from the area of both dorsobasal lobes (3rd West's zones). In accordance with the Helsinki Declaration 2004, on completion of the study, the animals were euthanased with a bolus of cardioplegic potassium chloride solution (Thomas 10% sol.) at a dose of 30±10 ml intravenously. The animals were then disposed of according to EU legislation.
Data obtained at time-2 and comparison between groups B and C (n=16).
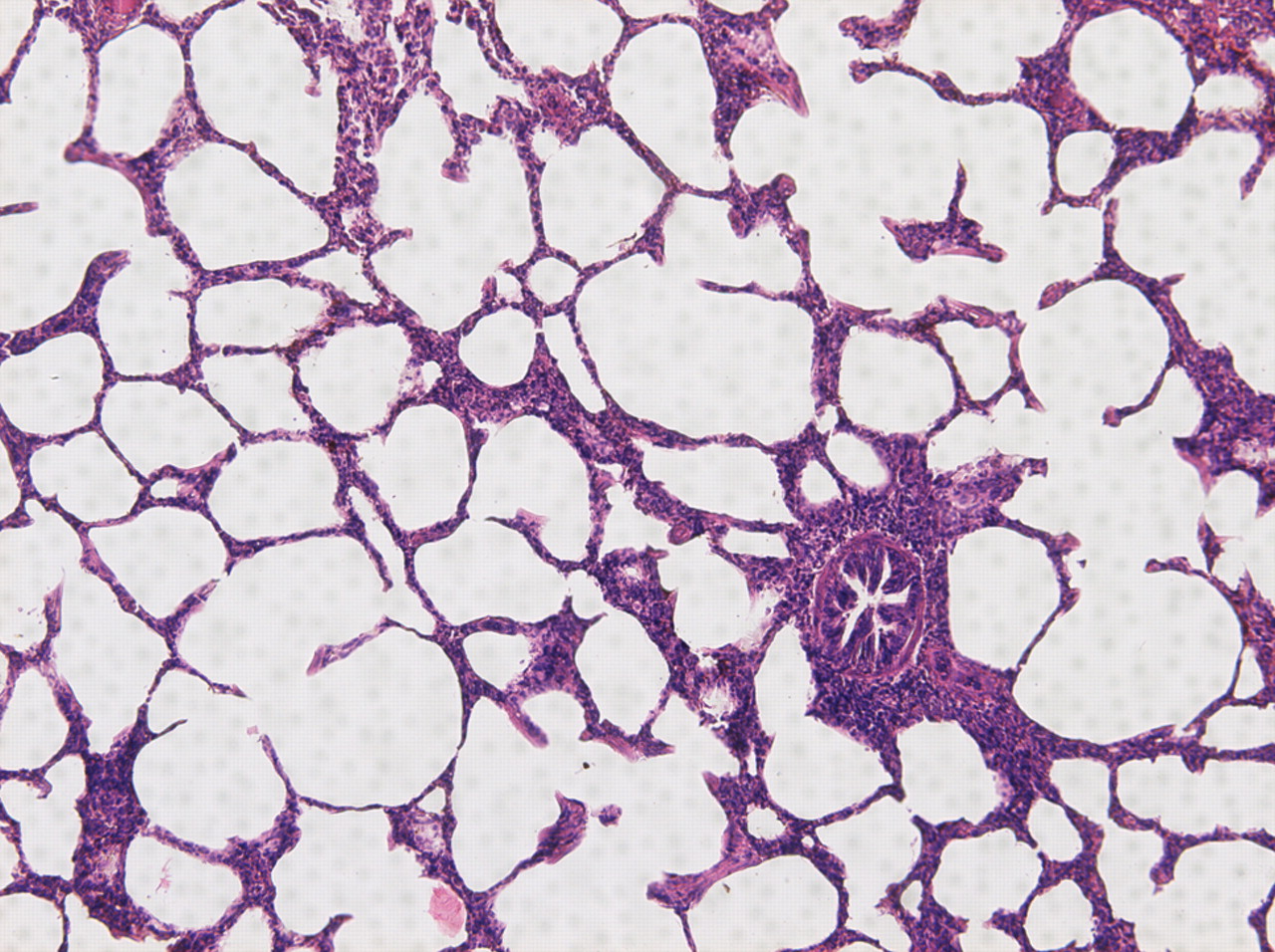
Optical microscopic image of mechanically ventilated lung tissue piglet (tidal volume 7 ml/kg). Normal alveolar architecture and aeration without pathological content. Alveolar septa were only minimally infiltrated, septal blood vessels mildly dilated, and small quantities of secretions apparent in the bronchioles.
Statistical analysis. All measurements and assessments were recorded continuously in our own PC database. Categorical data were compared using the Pearson's test, and for continuous data, the paired Student's and non-paired Wilcoxons tests were used. All statistical analyses were performed using ANOVA (PC software Analyse-i211 Software, Ltd., version 2008). All results in the text, tables and charts are expressed as the mean±SD) and 95% confidence interval (95% CI). A p-value less than 0.05 was considered to be significant.
Results
Data obtained for groups A, B and C at time-1 and comparisons between group A, B and C are listed in Table I. Already at time-1, differences were detected in group C when compared to data obtained for group B. In group C, higher values of CVP (t-test 6.44, p<0.01), RVP (t-test 4.72, p<0.01), PAoP (t-test 2.62, p<0.05), PVR (t-test 4.07, p<0.001), PIP (t-test 6.12, p<0.01), Paw (t-test 5.97, p<0.01), VTexp (t-test 10.17, p<0.01), MV (t-test 1.88, p<0.05), ICAM (t-test 8.10, p<0.01) were observed, and lower values for SV (t-test 2.04, p<0.05), CO (t-test 2.57, p<0.05), SVR (t-test 7.03, p<0.01), and Cdyn (t-test 9.61, p<0.01). Data obtained for groups B and C at time-2 and a comparison between these two groups is listed in Table II. When comparing the data obtained at time-1 and time-2 for each group, differences were only observed in group C with the rise of values CVP, PAoP, levels of ICAM (t-test 7.15, p<0.05) and VCAM (t-test 13.87, p<0.01), and conversely a decrease VTexp (t-test 6.07, p<0.01) and Cdyn (t-test 3.83, p<0.01) at time-2.
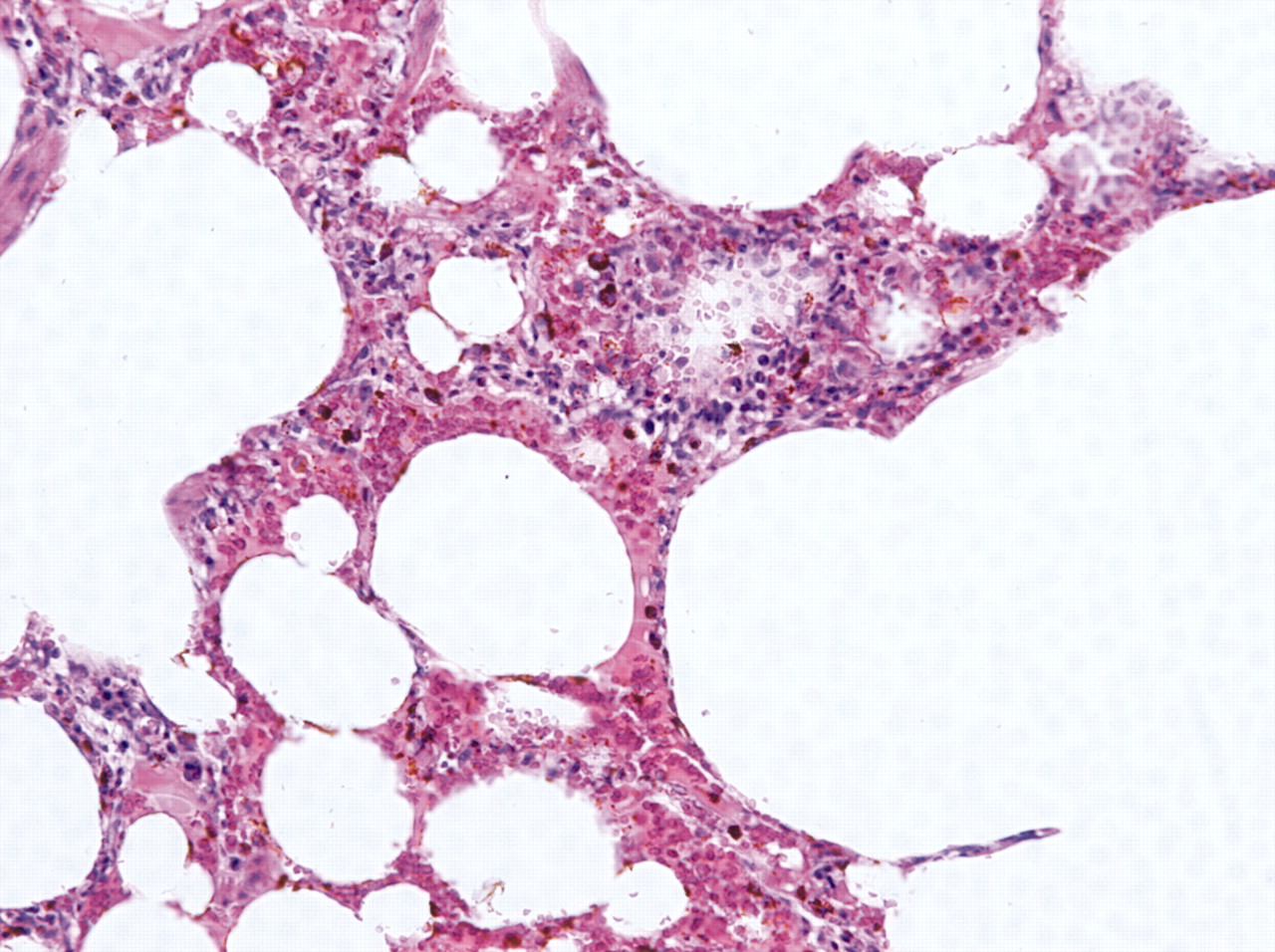
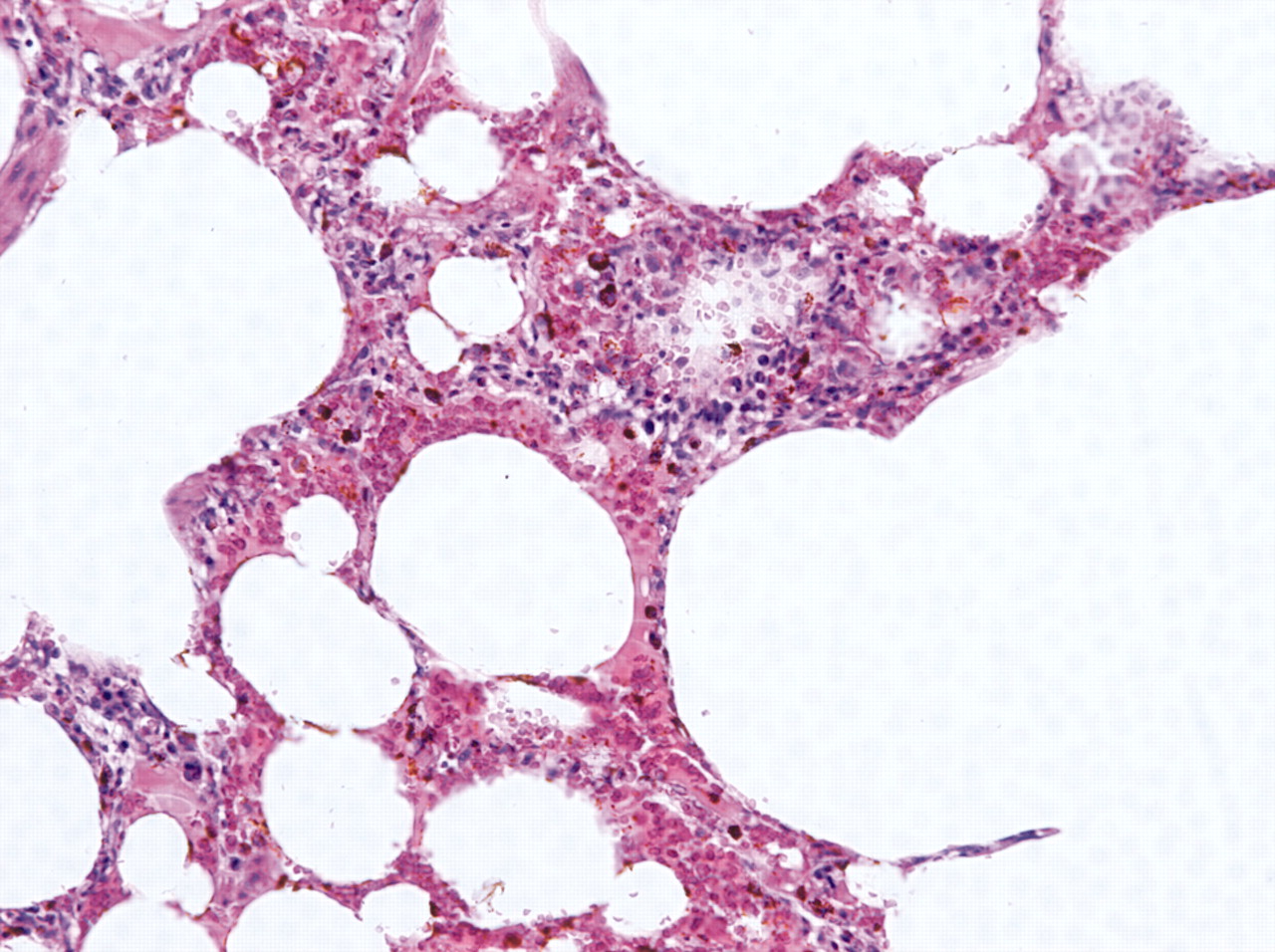
Optical microscopic image of mechanically ventilated lung tissue (tidal volume 12 ml/kg). Severe alveolar destruction, lumen narrowing and decreased aeration. Alveolar septal infiltration of macrophages around thrombosed venules.

{kind=link}
{kind=link}
{kind=link}
Electron microscopic image of the same lung tissue. Severe alveolar deconfiguration with damage to type-1 lung cells, increase in type-2 cell numbers, alveolar septal infiltration of macrophages and venule obliteration.
Changes in the morphology of lung tissue during the study, such as the severe alveolar destruction, lumen narrowing and decreased aeration during the study course are shown in Figures 1, 2 and 3.
The experiments were performed without any untimely death of the experimental animals. No animal was injured due to barotrauma.
Discussion
Mechanical ventilation is a non-physiological substitute for spontaneous breathing. An appropriate technique and setting must be selected in order to replace or support spontaneous breathing. A series of clinical and experimental studies have demonstrated that ‘protective’, low volume strategy mechanical ventilation respects the physiology of breathing and protects the parenchyma of lungs from more serious damage (9-11). Unsurprisingly, dynamic lung mechanics and haemodynamics data obtained during mechanical ventilation with an expiratory tidal volume of 7 ml/kg at the 30th and 90th minute of the study was comparable and corresponded with the accepted reference values for piglets (12). It is important to note that the global reduced function of the left ventricle in Group B animals did not significantly affect the results of this data (3). This valuable finding supports the hypothesis that a strategy of using low tidal volume during mechanical ventilation optimizes haemodynamics.
The ‘injured’, high tidal volume ventilation strategy was with an expiratory tidal volume of 12 ml/kg, on the other hand, an extremely non-physiological condition. Lung parenchyma was primarily damaged through physical effects. Excluding barotrauma as an extreme form of lung injury, diffuse alveolar damage was often the toll for hyperinflation of the lungs. If the damage occurs in association with mechanical ventilation, ventilator-induced or aggravated lung injury may be involved. Algorithms regarding the development of secondary damage to the lungs and extrapulmonary organs in relation to mechanical ventilation have been clarified in numerous studies (13, 14). Biophysical insult is the cause of a systemic lung decompartmentation and the induction of a systemic inflammatory reaction. The expression of cell adhesive molecules and the release of aggressive inflammatory cytokines take place. These then damage other extrapulmonary tissues, organs, and whole systems. Organs primed by cytokines are damaged both morphologically and functionally (15, 16). An integral part of the so-called multiorgan dysfunction syndrome is secondary lung injury and acute respiratory distress syndrome (17). Treatment of a developed affliction of the system is difficult, long-term, and very expensive. It is therefore prudent to prevent these disorders (18). Experimental and clinical experience, including the study preserved shows that lung hyperinflation during mechanical ventilation causes volume trauma which damages the lungs both morphologically and functionally (19, 20). Our surgical photographic documentation and histological examination of lung tissue samples demonstrate that morphological affliction of the lung parenchyma was not homogeneous. A reduction in airflow in some alveoli and an excessive distension of other alveoli with diffuse thickening of the septi through cellular infiltration were evident. In an open chest, it is possible to observe that during mechanical ventilation the sites of condensation and hyperinflation of lungs were alternating. Measurement of dynamic lung mechanics also confirmed negative functional effects. At the beginning of the experiment, the tidal volume was higher and dynamic compliance of the lungs was lower when compared with the control group. The differences increased significantly in the 90th minute of the experiment. There was a significant decrease in dynamic compliance and a reduction in the functional breathing capacity of the lungs.
Changes in lung mechanics and intrathoracic pressures during mechanical ventilation with high tidal volumes also have a significant influence on circulation and cardiac output (21, 22). In accordance with published work (23), the strategy of high tidal volume ventilation in our study increased the influence on heart–lung interaction that after 90 minutes caused a reduction in right ventricle performance, increased pressure in the pulmonary vascular bed and a decrease in cardiac output.
The expression of cell adhesion molecules is a sensitive indicator for the induction of a systemic inflammatory reaction (24-26). Non-physiological alveolar hyperinflation may be the cause of an intercellular interaction, a significant elevation in values of intercellular cell adhesive molecules in plasma, as well as a release (induced by the endothelium of the lung capillary bed) of vascular cell adhesion molecules (27-29). After surgery of the descending aorta and kidney transplantation, an induction of vascular cell adhesion molecules is presumed via the damaged vascular endothelium. Nevertheless, this study demonstrates that an inappropriate strategy of mechanical ventilation in transplanted animals after 90 minutes already significantly increases the expression of soluble cell adhesion molecules. These changes occurred within ninety minutes of mechanical ventilation at an expiratory tidal volume of about 12 ml/kg. We believe that this fact has not been shown in any of the published studies.
Conclusion
High tidal volume strategies in our experimental animals caused lung damage within ninety minutes. Pulmonary volume trauma resulted in serious complications, with primary morphological and functional lung injury, altered blood circulation and decreased cardiac output, and induction of a lung mechanotransduction and systemic inflammatory reaction within a short period of time. Strategies using low volume ventilation are unlikely to cause lung injury. Cardiac output may be influenced more easily by ventilator adjustment than pharmacological adjustment.
Acknowledgements
The study was supported by the Research intention of Charles University in Prague, Faculty of Medicine in Pilsen no. MSM 0021160819-6096, and grants by the Ministry of Health of the Czech Republic IGA no. NR/7909-3, and NR/8860-3.
- Received April 3, 2010.
- Revision received June 22, 2010.
- Accepted June 29, 2010.
- Copyright © 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved