

Abstract
We studied radioprotection and mitigation by mitochondrial-targeted Tempol (GS-nitroxide, JP4-039), in a mouse injury/irradiation model of combined injury (fracture/irradiation). Right hind legs of control C57BL/6NHsd female mice, mice pretreated with MnSOD-PL, JP4-039, or with amifostine were irradiated with single and fractionated doses of 0 to 20 Gy. Twenty-four hours later, unicortical holes were drilled into the tibiae of both hind legs; at intervals, tibias were excised, radiographed, and processed for histology. Bone wounds irradiated to 20 or 30 Gy showed delayed healing at 21 to 28 days. Treatment with JP4-039 MnSOD-PL or amifostine, before or after single fraction 20 Gy or during fractionated irradiation followed by drilling accelerated wound healing at days 21 and 28. Orthotopic 3LL tumors were not protected by JP4-039 or amifostine. In nonirradiated mice, pretreatment with JP4-039 accelerated bone wound healing. This test system should be useful for the development of new small molecule radioprotectors.
- Radioprotectors
- antioxidants
- nitroxides
- bone
The toxic effects of ionizing radiation on bone are of continued interest in radiation oncology. Pediatric oncology patients are at particular risk of long-term side-effects from irradiation of immature bone, including abnormal skeletal maturation, growth retardation, and fracture (1-7). The higher threshold dose for bone injury in adults is manifested primarily by osteoradionecrosis and fracture (5, 8).
Irradiation of bone leads to depression of mineral metabolism, structural weakness, alteration of bone remodeling, and decreased vascularity (9). In children, growth deformities occur particularly when active growth plates are encompassed within radiation fields such as in the treatment of extremity sarcomas (7, 10-11). Prior studies in bone fracture models demonstrated that radiation significantly delays bone wound healing, hypothesized as attributable to damage to bone-regenerating osteoblast precursors in the bone marrow and periosteum (12, 13).
Some radioprotectors including amifostine (14-17) and (MnSOD-PL) (18-20) have been reported, and neither of the latter protects tumors (14, 20). Amifostine has been demonstrated in murine models to protect bone from irradiation-induced injury (7, 10-11, 14-17). Of recent interest is the drug tempol (4-hydroxy-2,2,6,6-tetramethylpiperidine-N-oxyl) which is a stable, free-radical scavenging nitroxide that demonstrates in vivo radioprotective properties, in part by blocking mitochondrial mechanisms of apoptosis (21-24). By coupling 4-amino TEMPOL to a segment of the cyclopeptide antibiotic gramicidin S (GS), the nitroxide is targeted to the mitochondria, where scavenging of reactive oxygen species (ROS) is increased, thus preventing cell death (24). The alkene peptide isostere GS-segment derived JP4-039 (hemigramicidin S-segment-conjugated 4-amino-2,2,6,6-tetramethyl-piperindine-N-oxyl) represents a unique mitochondrial-targeted small molecule GS-nitroxide.
In the present report, we utilized a novel murine combined bone wound-irradiation injury model to assess the effect of JP4-039 on irradiation-induced delay in bone wound healing compared to amifostine and MnSOD-PL.
Materials and Methods
Mice. Six- to eight-week-old female C57BL/6NHsd mice (20 to 22 g; Harlan Laboratories, Indianapolis, IN, USA) were housed according to IACUC protocols at the Hillman Cancer Center – University of Pittsburgh Cancer Institute. All protocols were approved by the IACUC of the University of Pittsburgh. Veterinary care was provided by the Division of Laboratory Animal Research of the University of Pittsburgh.
Experimental framework. The first phase of the study examined the effect of single fraction irradiation on bone wound healing. Right hind limbs of mice were irradiated with a single fraction dose of 0, 10, 20, 30, 40, or 50 Gy. The left hind limbs of all mice were non-irradiated. Twenty-four hours after irradiation, unicortical wounds were created in the proximal tibiae of both hind limbs. Healing of the unicortical wounds was assessed by x-ray at intervals up to 35 days. A full description of irradiation technique, creation of bone wounds, and assessment of bone wound healing is detailed in further sections below.
The second phase of the study examined the roles of amifostine, MnSOD-PL, and JP4-039 as radioprotectors and radiomitigators in the bone wound/irradiation model. Subgroups of mice were injected intravenously (i.v.) with 100 μl MnSOD-PL (100 μg of plasmid DNA in 100 μl water) or 100 μl empty plasmid liposome 24 hours before irradiation, injected intraperitoneally (i.p.) with 100 μl of amifostine (250 mg/kg as described below) 10 min prior to or immediately after irradiation of the right hind limb, or injected i.p. with 100 μl JP4-039 (10 mg/kg as described below) 10 min prior to or immediately after irradiation of the right hind limb. Irradiation was delivered as a single fraction of 20 Gy.
In a fractionation study, mice were treated with amifostine, MnSOD-PL, or JP4-039 prior to 20 Gy delivered in 4 daily fractions of 5 Gy. In this study, amifostine and JP4-039 were given prior to each fraction in the same manner as above and MnSOD-PL was given prior to the first and third fractions respectively. Twenty-four hours after completion of 20 Gy irradiation, bone wounds were created and healing was assessed. Groups of control mice were treated with each of the test drugs and bone wounds were created without irradiation. Assessment of bone wounds was carried out at a single time point 21 days after irradiation in mice treated with amifostine either before or after irradiation and in those mice given fractionated irradiation.
Another study was designed to assess whether JP4-039 would differentially protect normal tissue and not tumor tissue from irradiation-induced damage using an orthotopic Lewis lung carcinoma, described below.
Tibial bone wounds/bone drilling. This mouse model is based upon a model of tibial wound repair in rats (25). Mice were anesthetized by i.p. injection of phenobarbital (220-250 μl, 1:10 dilution in water, 70 mg/kg). Anesthetized mice were placed supine. Each hind limb was cleaned with alcohol (Kendall, Mansfield, MA, USA), and a 15 mm incision of the skin lateral to the anterior tibial crest was created with surgical scissors. The lateral aspect of each tibia was exposed and carefully cleared of overlying soft tissue. A unicortical osseous wound was created 5 mm below the proximal epiphyseal cartilage plate with a handheld engraving drill (Dremel, Racine, WI, USA) and a 1.6 mm engraving cutter drill bit (Dremel, #113; Racine, WI, USA). Evidence of unicortical osseous wounding was indicated by exposure of the marrow cavity. Irrigation with cold phosphate-buffered saline (PBS, 1x, Mediatech, Herndon, VA, USA) was used to remove bone dust and fragments. The soft tissue envelope was reapproximated and the skin was closed with 9 mm stainless steel wound clips (Becton Dickinson, Sparks, MD, USA).
Radiographs and measurements. Groups of mice were sacrificed at serial 7-day intervals following drilling (i.e. days 7, 14, 21, 28, and 35 post-drilling) or at 21 days following drilling alone. Radiographs of mice limbs were taken with a 35 kV X-ray machine (MX-20; Faxitron X-ray LLC., Lincolnshire, IL, USA) at ×1.5 magnification. Limbs were positioned with the lateral surface facing the beam. Radiographs (Kodak BioMax XAR, Rochester, NY, USA) were scanned, digitized, and imported into Adobe Photoshop CS3 (Adobe Systems Inc., San Jose, CA, USA). The diameter of each wound was measured in triplicate in units of pixels with a ruler tool provided in the software package. Pixels were converted to millimeters (one pixel having been determined to be 1/100 of a millimeter). The triplicate values for each bone were averaged for statistical analysis. Measurement data for the non-irradiated left limbs of mice with irradiated right limbs were included in the non-irradiated groups for analysis.
Drug delivery. MnSOD-PL was injected i.v. as 100 μl of MnSOD plasmid/liposome complex or control blank plasmid/liposome complex containing 100 μg of plasmid DNA (empty plasmid liposome control). JP4-039 was dissolved at a concentration of 2 mg/50 μl cremphor el or 50 μl of ethanol. A volume of 100 μl of the JP4-039 stock solution was diluted 1:9 with water (900 μl). Mice were treated with 100 μl of JP4-039 at a dose of 10 mg/kg via i.p. injection. Amifostine 500 mg per vial was reconstituted with 10 ml of saline and injected at 100 μl per mouse i.p. for a dose of 250 mg/kg.
Irradiation. Radiation was delivered by 6-MV linear accelerator (Varian Corporation, Palo Alto, CA, USA). Mice were anesthetized with phenobarbital and right hind limbs immobilized with paper tape within the confines of a 38×2 cm irradiation field. One centimeter of tissue-equivalent bolus was added to ensure full dose to the limbs. Initial single fraction experiments used doses of 10-50 Gy prescribed to 100 cm source to bolus distance (SBD) to measure the effect of radiation dose on bone healing. Subsequent phases of the study used 20 Gy (single fraction or fractionated) to the right limb. After irradiation, 24 hours elapsed before tibial drilling, according to IACUC protocols to minimize stress on the animals.
Orthotopic tumors. Orthotopic Lewis lung carcinoma (20) cells were grown in culture and a suspension of 1×106 cells was injected subcutaneously adjacent to the site of planned drilling within the planned irradiation field of the right leg. When tumors achieved a diameter of 2 mm, randomized subgroups of mice were treated with JP4-039, amifostine, or no drug prior to 10 Gy irradiation to the right hind limb. Twenty-four hours after irradiation, holes were drilled in the proximal tibiae of both hind limbs. Another control group of mice had the orthotopic Lewis tumor placed without being irradiated, wounded, or given any drug. Tumor growth was observed and the fold increase in tumor volume was calculated as final tumor volume (day 5) divided by initial tumor volume (day 1, in relation to wound creation).
Histological examination. Excised tibiae were trimmed, fixed with 2% paraformaldehyde in 0.1 M cacodylate buffer (pH 7.4) for approximately one week at 4°C, rinsed in 0.1 M cacodylate buffer, and decalcified in ethylenediamine tetraacetate (EDTA 7.5% 0.1 M cacodylate buffer) for at least 5 weeks with solutions changed every two days the first week, and twice per week thereafter. The bones were embedded in glycol-methacrylate (JB-4; Polysciences, Warrington, PA, USA). Five-μm cross-sections were mounted on Super-Frost slides (Fisher Scientific, Pittsburgh, PA, USA) and were stained with toluidine blue (TB) and for tartrate-resistant acid phosphatase enzyme activity (TRAP) in osteoclasts.
Statistical analysis. For the first phase of the study, two-sided two-sample t-tests were used to compare drilled hole size for mice in each radiation dose group (10 Gy, 20 Gy, 30 Gy, 40 Gy, and 50 Gy) with that of the size of the drilled holes in mice in the 0 Gy group at day 7, 14, 21, 28, and 35 timepoints. For the second phase of the study, one-way ANOVA was performed to test whether the size of drilled holes was statistically the same at day 7, 14, 21, 28, and 35 timepoints in each of the following treatment groups: 0 Gy, 0 Gy-MnSOD-PL, 0 Gy-JP4-039, 0 Gy-empty liposome, 20 Gy, 20 Gy-MnSOD-PL, 20 Gy-JP4-039, 20 Gy-empty liposome. Following ANOVA, Tukey's test, which tests for significant differences between groups, was used to determine the significance of differences between treatment groups.
Results were obtained at 21 days following drilling for groups in a fractionation experiment treated with JP4-039 or amifostine before or after single fraction irradiation and for groups given JP4-039, MnSOD-PL, and amifostine after fractionated irradiation. One-way ANOVA followed by the two-sided two-sample t-test with Bonferroni adjustment was used to analyze these data.
Results
Ionizing irradiation delays tibial bone wound healing. We observed a dose-dependent effect of irradiation over the range of 10-30 Gy in delaying unicortical tibial bone wound healing. The 10 Gy, 20 Gy, and 30 Gy groups were evaluated and compared with non-irradiated controls (Table I). Groups of mice also received doses of 40 Gy or 50 Gy. Those mice had significant soft tissue damage by day 21 such that they were euthanized according to IACUC regulations. At 7 and 14 days post drilling, no significant differences in sizes of the wounds were observed between the 0 Gy group and any of the irradiated groups. At 21 days post-drilling, significant differences were detected for the 20 Gy and 30 Gy groups (mean±SEM, 0.93±0.37 mm, p=0.008 and 1.07±0.19 mm, p=0.0002, respectively) compared with the 0 Gy group (0.68±0.27 mm). There were significant differences at 28 days post-drilling between the 10 Gy (0.76±0.15 mm, p=0.0003), 20 Gy (0.86±0.34 mm, p=0.04), and 30 Gy (0.76±0.15 mm, p=0.02) groups and the 0 Gy group (0.31±0.33 mm). By day 35, the size of drilled holes in all groups was reduced below the sensitivity for analysis of wound size differences.
JP4-039 ameliorates irradiation-induced delay in bone wound healing. The effects of antioxidants JP4-039 and MnSOD-PL on bone wound healing were evaluated when administered prior to irradiation (Table II). Comparison of the groups exposed to 20 Gy, 20 Gy-MnSOD, and 20 Gy-JP4-039 revealed no differences in hole size at days 7 or 14 post drilling. Significant amelioration of irradiation delay of bone wound healing was observed at day 21 post drilling in both the 20 Gy-JP4-039 group (mean±SEM, 0.51±0.05 mm, p<0.05) and the 20 Gy-MnSOD-PL (0.68±0.07 mm, p<0.05) group, compared with the 20 Gy group (1.01±0.10 mm). At 28 days post-drilling, significant differences in hole diameter were detected for the 20 Gy-JP4-039 group (0.37±0.04 mm, p<0.05) and 20 Gy-MnSOD-PL group (0.49±0.02 mm, p<0.05), compared with the 20 Gy group (0.76±0.13 mm).
JP4-039 Stimulates bone wound healing in the absence of irradiation. Comparison of the non-irradiated groups (0 Gy alone, 0 Gy-MnSOD-PL, 0 Gy-JP4-039) revealed no significant differences in hole diameters at day 7 following drilling. At day 14, significant differences were detected in comparisons between either the 0 Gy-JP4-039 (0.55±0.03 mm, p<0.05) or 0 Gy-MnSOD-PL (0.49±0.05 mm, p<0.05) and the 0 Gy alone group (0.84±0.05 mm) (Table II). At 21 days post-drilling, a therapeutic effect of MnSOD-PL and JP4-039 was detected (0 Gy-MnSOD-PL: 0.41±0.04 mm, JP4-039: 0.47±0.04 mm, versus 0 Gy alone: 0.64±0.05 mm, p<0.05). No significant differences were observed between MnSOD-PL or JP4-039 treatment compared with control irradiation groups at 28 days post drilling.
JP4-039 Mitigates irradiation induced delay in bone wound healing. Mice treated with JP4-039 or amifostine after irradiation showed a statistically significant improvement in bone wound healing (Table III). Bone wound healing in this cohort was assessed at 21 days post drilling. When treated prior to 20 Gy irradiation, mice given JP4-039 (0.57±0.04 mm, p<0.001) or amifostine (0.73±0.01 mm, p<0.001) both demonstrated statistically significant decreases in bone wound size compared with controls (1.06±0.02 mm). Statistically significant radiomitigation was demonstrated for groups given JP4-039 (0.52±0.01 mm, p<0.001) or amifostine (0.79±0.02 mm, p<0.001) after irradiation, compared with the control irradiated group (1.06±0.02 mm). JP4-039 improved bone healing to a greater extent than amifostine when administration prior to or following irradiation (Table III).
JP4-039 Ameliorates fractionated irradiation-induced delay in bone wound healing. Effects of treatments were similar for mice given fractionated irradiation (Table IV). At day 21 post-drilling, both the irradiated and non-irradiated limbs in the three treatment subgroups (JP4-039, MnSOD-PL, and amifostine) had significant reduction in tibial wound size compared with the respective control limbs.
Irradiation-induced delay in healing of unicortical osseous wounds in mouse tibiae. Unicortical osseous wounds were created by drilling of anesthetized mice and limbs were irradiated to each dose as described in the Methods (n=5 mice in each group).
Small molecule GS-nitroxide JP4-039 or MnSOD-PL ameliorate irradiation-induced delay in unicortical osseous murine tibiae wound healing.
Orthotopic tumors are not protected from irradiation by JP4-039 or amifostine. Neither JP4-039 nor amifostine altered the effect of irradiation to reduce growth of orthotopic Lewis lung carcinoma (Figure 4). For the irradiated hind limb, the fold increase in tumor volume was significantly reduced in all treatment groups compared with non-irradiated controls (Figure 4A). For the non-irradiated hind limb, only the group that received JP4-039 followed by 10 Gy irradiation of the other leg showed significant reduction in tumor growth compared with controls; however, all treatment groups showed a reduction in increase of tumor volume compared with the control group (Figure 4B).
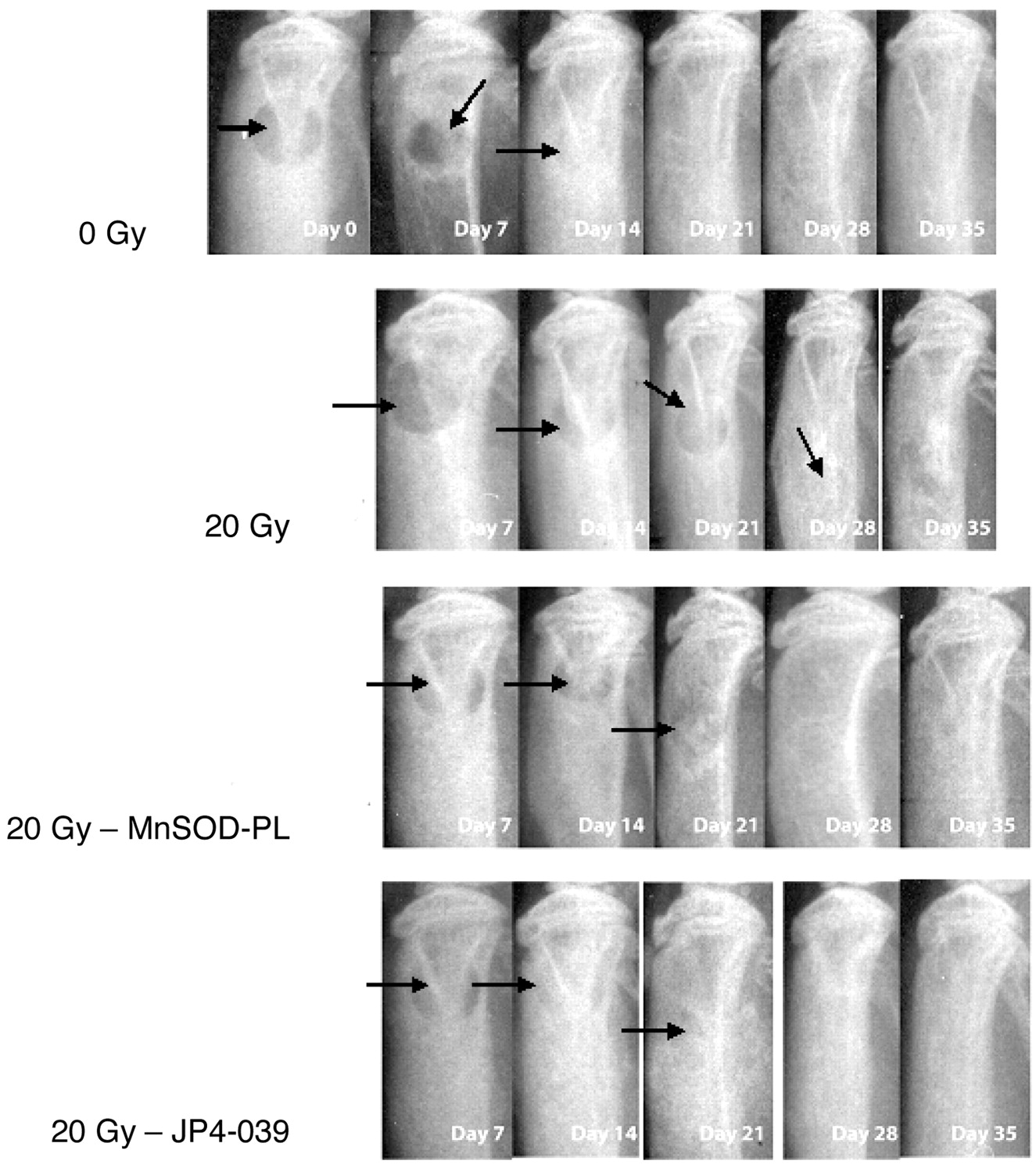
Radiographic and histologic evidence of bone wound healing. Representative radiographs of proximal tibiae from the 0 Gy, 20 Gy, 20 Gy-MnSOD-PL, and 20 Gy-JP4-039 groups reveal the effects of time and treatment on bone wound healing (Figure 1). Radiographs in the 0 Gy group demonstrated a decrease in wound size. In contrast, wounds in 20 Gy irradiated bones remained radiolucent through 28 days. Radiographs of bones from 20 Gy irradiated mice which had been pre-treated with MnSOD-PL or JP4-039 demonstrated persistence of holes though day 21, with healing by day 28.
JP4-039 and amifostine are effective mitigators of irradiation-induced delay in bone wound healing.
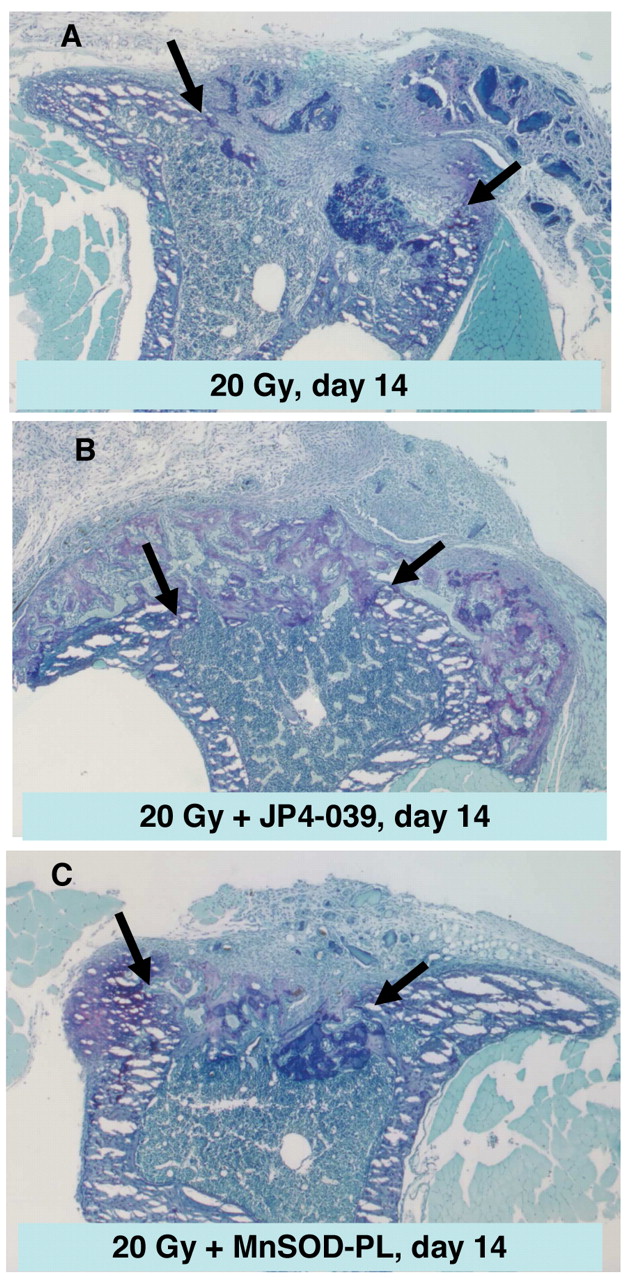
Histopathological evaluation of controls indicated that tibial wounds spontaneously healed, with complete bridging with new bone by 35 days (Figure 2). Specimens from mice with irradiation of limbs prior to wounding revealed more fibrous tissue than reactive bone in the wounds (Figure 3). Specimens from animals that were pre-treated with JP4-039 or MnSOD-PL revealed new bone formation compared with specimens from irradiated mice (Figure 3). These histological findings confirm the irradiation-induced delay in bone wound healing and the ameliorating effect of JP4-039.
Discussion
The pathophysiology of fracture healing and the effects of irradiation on the process are complex. A hematoma/fibrinous clot first forms, followed by ischemia and inflammation (26-27). Local growth factors recruit polymorphonuclear cells, macrophages, mast cells, and mesenchymal stem cells to the fracture site. Osteoblastic precursors are also systemically mobilized through the peripheral circulation and home to the fracture site, where they undergo migration, proliferation, and differentiation (28-32). Subsequent stages in fracture healing include cartilage formation, calcification, angiogenesis, bone formation, and bone remodeling (26). Irradiation alters the process of bone repair (33-35) including loss of osteocytes and osteoblasts, hyaline necrosis of blood vessels, and replacement of bone marrow by fibrous connective tissue (12). Irradiation may also impair bone healing by reducing the proliferation of bone-regenerating precursor cells located in the bone marrow (8). Vascular injury from irradiation may impair bone healing by reducing angiogenesis at sites of new bone formation (8), because endochondrial ossification is known to be dependent on adequate vascularity (30). Pediatric oncology patients carry a great risk of irradiation-induced bone toxicity and the severity is dependent on dose, volume irradiated, location, and age (6, 7).
JP4-039, MnSOD-PL, and amifostine are effective as protectors against irradiation damage to tibial wound healing during fractionated irradiation.
The generation of ROS in the bone environment leads to the formation and activation of osteoclasts and to subsequent bone resorption (31, 32). The oxidative stress produced by fracture not only occurs in the immediate inflammatory period, but rather endures for at least one month following fracture (32). Irradiation also increases osteoclast numbers in vivo and in vitro (31, 32). The combination of fracture and irradiation creates a pool of free radicals that inhibit proliferation of osteoblast progenitors and that stimulate osteoclast proliferation, which can further impair bone wound healing.

Radiographs of drilled tibia at various time points for the 0 Gy, 20 Gy, 20 Gy-MnSOD, and 20 Gy-JP4-039 groups. Photographs of representative tibiae at each time point are presented (magnification ×1.5). Arrows show persistent visible holes at day 21 and day 28 in the 20 Gy irradiation compared to nonirradiated controls (0 Gy) or irradiated MnSOD-PL- or JP4-039-treated irradiated mice.
Radioprotectors of bone have been described in the literature. Recombinant human bone morphogenic protein-2 led to more rapid healing of bone defects in rat calvaria irradiated with 12 Gy prior to creation of the defect (33). Amifostine at 300 mg/kg 20 minutes prior to 35 Gy delivered as a single fraction to the right orbitozygomatic complex improved bone healing (34). Reduction in radiation toxicity for craniofacial bone was seen when amifostine preceded fractionated radiation to the same dose of 35Gy (35), as well as for long bones (16-17). Beneficial effects of other antioxidants and ROS scavengers in fracture healing have been reported. Daily injections of vitamin C mitigated the damaging effect of 5 days of i.p. injections of zymosan on fracture healing (36) and more rapid bone healing was observed in dogs given vitamin E daily for one week following radial diaphysis fracture (37).

Photomicrographs of A: intact tibia, B: tibia after creation of unicortical tibial wound, and C: tibia 35 days after creation of tibial wound. Decalcified bones were embedded in glycol-methacrylate, cross-sectioned at 10 μm, and stained with toluidine blue. Arrows indicate margins of the wound. Complete wound healing is evidenced by osseous bridging at day 35 (magnification ×28).
We have developed a novel model to assess the effectiveness of new radioprotectors and mitigators on the radiation-induced bone healing delay. Use of the model showed that a new GS-derived nitroxide drug (JP4-039), as well as MnSOD-PL and amifostine, were effective radioprotectors and radiomitigators of bone wound healing in both single fraction and fractionated irradiation protocols. It is clinically important that JP4-039 did not protect orthotopic Lewis lung carcinoma tumors from irradiation-induced suppression of growth. Furthermore, there was apparent stimulation of bone wound healing by JP4-039, MnSOD-PL, and amifostine, even in the absence of irradiation. Because both irradiation and bone wounding result in the production of ROS, scavenging of these free radicals by the antioxidant drugs presumably resulted in improved bone healing in the presence or absence of irradiation.
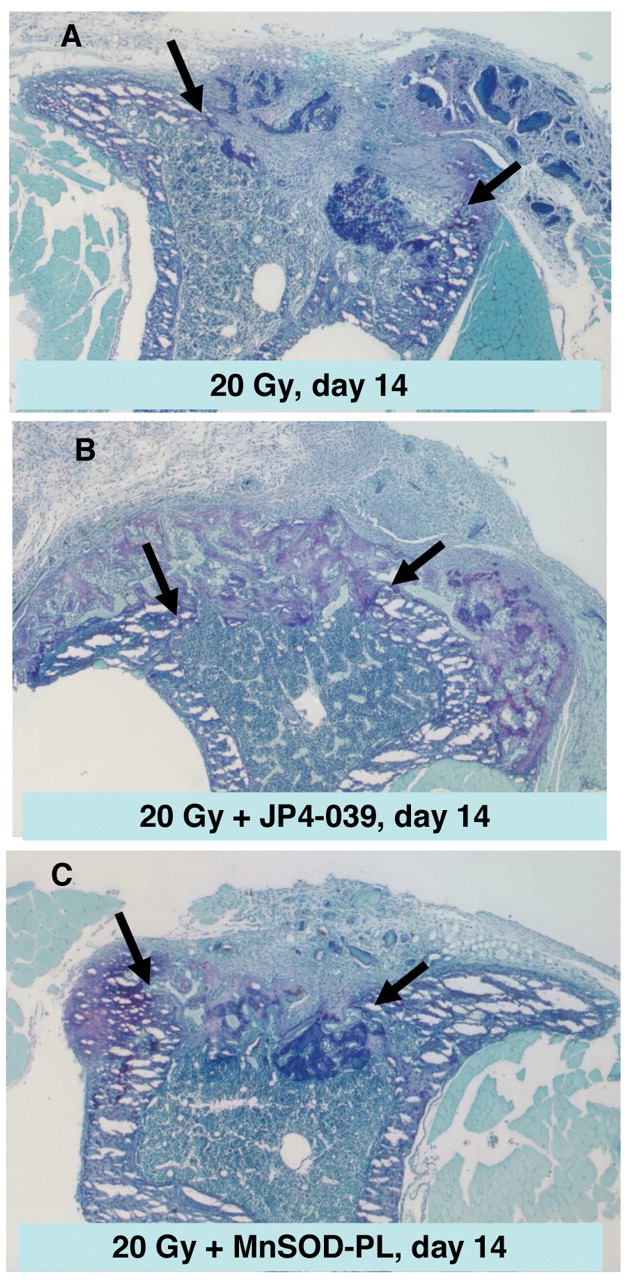
Photomicrographs of tibiae 14 days after creation of wounds in mice with A: 20 Gy irradiation; B: 20 Gy irradiation and pretreatment with JP4-039; and C: 20 Gy irradiation and pretreatment with MnSOD-PL. Decalcified bones were embedded in glycol-methacrylate, cross-sectioned at 10 μm, and stained with toluidine blue. Arrows indicate margins of the wound. The wound from a mouse with limb irradiated to 20 Gy was filled with fibrous connective tissue and robust neo-osteogenesis is visible in wounds from mice that were irradiated and pretreated with either JP4-039 or MnSOD (magnification ×28).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Absence of protection of orthotopic tumor by JP4-039 treatment of irradiated mouse tibial wound. (A): For the irradiated right hind limb, all treatment groups showed significant reduction in tumor fold increase compared to the control group (B) For the non-irradiated left hind limb, all groups showed less tumor volume fold increase than the control group with only the JP4-039 plus 10Gy irradiation showing a significant reduction in tumor volume fold increase.
Using a novel murine model of combined bone wound/irradiation injury, we report amelioration of irradiation-induced delay of bone wound healing by a novel GS-derived-nitroxide peptide isostere JP4-039, amifostine, and MnSOD-PL. These antioxidants and intracellular ROS scavengers also stimulated bone wound healing in the absence of irradiation. This murine model should be of value in testing new small molecule radioprotectors and radiomitigators in the setting of bone injury.
Acknowledgements
This study was supported by NIAID/NIH Grant U19A1068021 and BARDA Contract HHSO10200800062C.
Footnotes
-
* Presented at the 51st Annual Meeting of the American Society of Radiation Oncology.
- Received January 27, 2010.
- Revision received April 8, 2010.
- Accepted April 16, 2010.
- Copyright © 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved