

Abstract
The relevance of an uncompromized immune system for the development and progress of breast cancer still is a matter of intensive research. The impact of chemo- and/or radiotherapy on peripheral blood immune cell counts and activity of breast cancer patients (n=660) was investigated by flow cytometry. Not only the absolute counts, but also the comparison of those counts with standard values were evaluated. Most studies do not consider this comparison. As compared to pre-treatment values, leukocytes, lymphocytes, B-lymphocytes, T-lymphocytes, helper T-cells and CD25+ T-cells (activated T-cells) were significantly reduced after chemo- and/or radiotherapy. However, mean cell counts remained within the normal range. Statistically non-significant down-regulation was detected for cytotoxic T-cells, suppressor T-cells and natural killer cells, which are of prime importance as far as tumor development and defence are concerned. The impact of the therapy is not predictable for individual cases. However, only less than 20% of the breast cancer patients were immunocompromized after chemo- and/or radiotherapy.
- Breast cancer
- guideline-based adjuvant treatment
- immunosuppression
- complementary treatment
Breast cancer is the most frequent malignancy in women in Germany and worldwide with rising incidence and falling mortality since 1980 (1). The multimodal treatment comprises secondary prevention, operation, chemo- and/or radiotherapy as well as hormone and immune therapy with antibodies against Her2/neu.
Beyond these evidence-based therapies, most patients want to improve the outcome and their quality of life with complementary medicine. The American Cancer Society defines complementary medicine or methods as those that are used along with regular medical care. If these treatments are carefully chosen and managed, they may enhance comfort and well being (2). Some complementary treatments have been tested, e.g. nutrition, sports, psycho-oncology, while others have not (3).
Treatment with immunomodulating mistletoe extract is the most frequently used complementary therapy in Germany. Its efficacy in terms of improving quality of life and stimulating the immune system has been shown (4-6), however, it still is controversially discussed.
Nothing is mentioned about complementary treatments and their indication in the recent S3 guideline for breast cancer. To make a scientifically based recommendation concerning complementary immunotherapy for patients, their cellular immune system should be measured six to eight weeks after chemo- and/or radiotherapy. During this time interval the cellular immune system usually recovers from therapy-induced suppression.
This investigation was performed to analyse the cellular immune system of breast cancer patients before and after guideline based chemo- and/or radiotherapy.
Patients and Methods
This investigation analyses the cellular immune system of 660 breast cancer patients who attended consultation concerning complementary treatment at the Institute of Naturopathy at the University of Cologne. The mean age of the patients varied statistically significantly among the four groups. However, the values were all within the sixth decade and therefore differences were negligible (7-9). Also negligible was the TNM status of the patients which was not considered important for this analysis of the impact of chemo- and/or radiotherapy on the cellular immune system. Data were collected before and 6-8 weeks after the patients had finished adjuvant treatment in accredited breast cancer centres in Cologne. Therefore the patients were divided into four groups: without adjuvant treatment (n=391); after chemotherapy (n=55); after radiotherapy (n=52); after chemo- and radiotherapy (n=162). Peripheral blood cells were measured by flow cytometry (FACSCalibur™; BD Biosciences, San Jose, USA) and analysed with the statistic software programme SPSS. The standard values used in the Institute of Naturopathy are presented in Table I (7).
The comparison of the individual cell counts with the standard values was a strictly descriptive data analysis.
Normal range of blood cell counts and activity as described (7).
Results
Peripheral blood cells of 660 breast cancer patients were analysed before and after (6-8 weeks) adjuvant chemo- and/or radiotherapy. For each cell type descriptive statistics, characterization in form of box plots and bar charts for the leukocytes were performed. As shown in Figures 1 and 2, chemo- and/or radiotherapy reduced leukocyte counts, however, mean values remained within the normal range.
As shown in Table II, counts of leukocytes, lymphocytes, B-lymphocytes, T-lymphocytes, helper T-cells and CD25+ T-cells (activated T-cells) were significantly reduced after chemo- and/or radiotherapy as compared to pre-treatment values. Most suppressed were helper T-cells and B-cells, with values about 30% below normal range. Cytotoxic T-cells, suppressor T-cells and NK cells, which are important for tumour development and progress were non-significantly reduced after chemo- and/or radiotherapy. Table II shows mean and standard deviation for all cell populations investigated.
Besides these observations concerning immune cell counts and activity in patients with or without chemo- and/or radiotherapy (n=660), a separate investigation was performed in 33 patients who had their cellular immune system intraindividually checked before and after adjuvant therapies. Results were comparable to those of the whole (interindividual) group. An observation in this patient group was that although absolute counts and arithmetic mean were lower after adjuvant treatment, some patients presented increased cell counts after treatment. This observation confirms that in the individual case results are not predictable.
Decreased counts of one cell type does not automatically mean a compromized immune system. Synergistic acting cells such as NK cells and cytotoxic T-cells can compensate the function of each other.
Mean and standard deviation for all cell populations investigated.
Discussion
The evaluation of counts and activity of peripheral blood immune cells is an important contribution to the aftercare of breast cancer patients who ask for immunostimulating complementtary treatments. Most patients take complementary medicine during and after the recommended standard therapies (3). The indication, however, has to be analysed to avoid useless or even harmful treatment, especially immunostimulating therapies. Therefore, analysis of the cellular immune system six to eight weeks after finishing tumordestructive treatments may be regarded a helpful instrument.
To evaluate peripheral blood leukocytes and their subpopulations it is important to be aware of possible confounders such as age, psychological constitution, additional medication and alimentation (7-13). Since all patients were treated in accordance with international guidelines optimized by recommendations for evidence-based complementary therapies, e.g. nutrition, sports and psychooncology, confounders were considered.
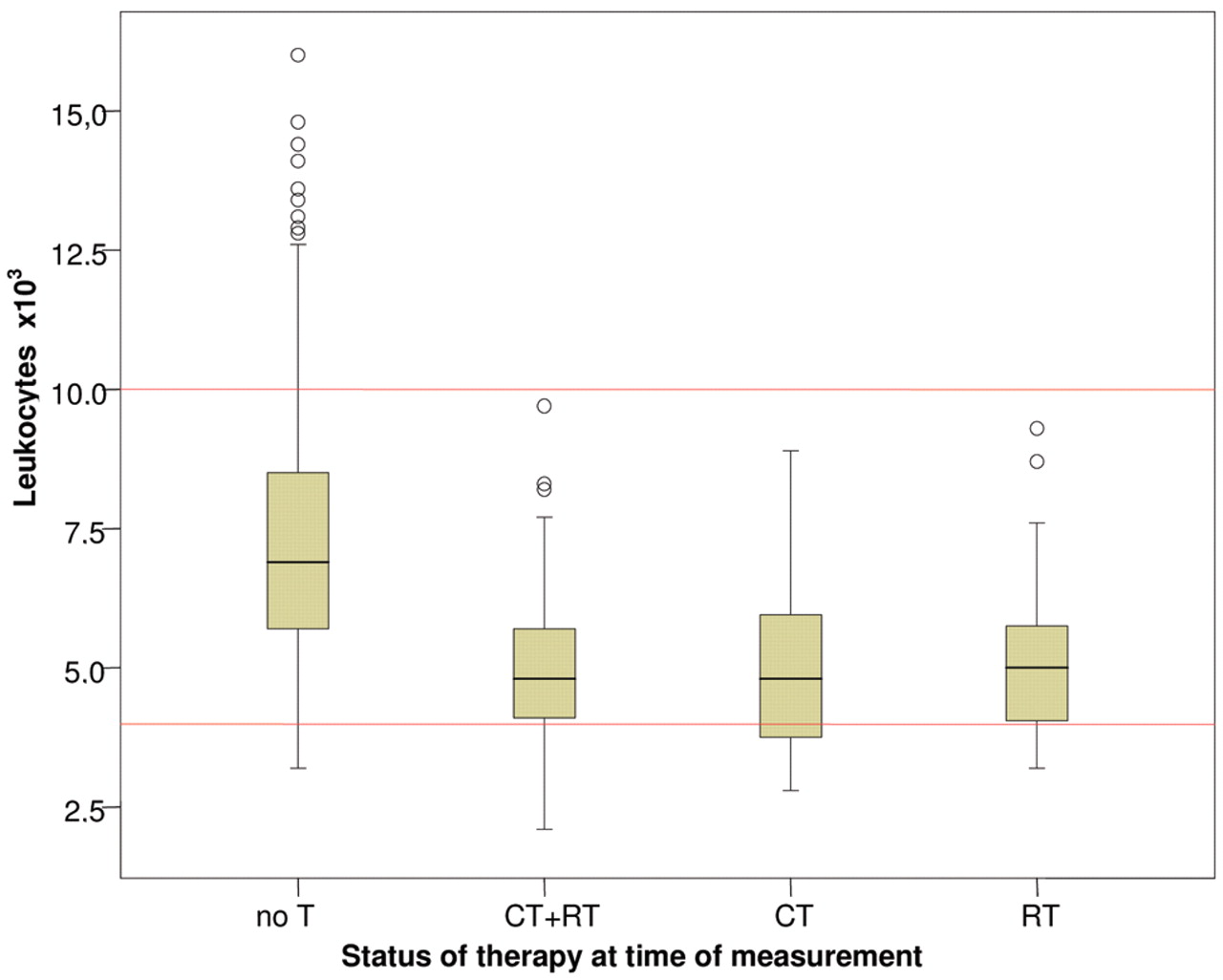
Median, interquartile range and upper and lower whisker. Absolute counts decreased 6-8 weeks after termination of the adjuvant therapies. Approximately 75% stayed within the normal range. No T: no adjuvant therapy; CT: adjuvant chemotherapy; RT: adjuvant radiotherapy.
Patients who are submitted to the “Disease Management Programme” for breast cancer receive an indication-based chemotherapy consisting of 5-fluorouracil, taxanes, anthracyclines and cyclophosphamide according to international guidelines. For these drugs depending on dose and application schedule, evidence was shown for immunosuppressing and immunostimulating effects (14-19). Given as combination therapy after surgery of breast cancer, the suppressing qualities are dominant. It has been frequently shown that chemo- and/or radiotherapy down-regulate the immune systems. But most studies concerning this topic are lacking the comparison with standard values, which are very important for judging the indication for stimulating therapies.
In the present investigation, this comparison revealed that fewer than 20% of the patients have absolute immune cell counts below standard that require attention and treatment. Accordingly, it contributes to a better understanding of the immunosuppressing activities of adjuvant therapy. Since more than 60% of cancer patients in Germany receive immunomodulating therapies (3), this investigation confirms that the cellular immune system should be evaluated before starting complementary immunotherapy.

{kind=link}
{kind=link}
Percentage of breast cancer patients with leukocyte counts within/below/above the normal range as shown in Table I. No T: no adjuvant therapy; CT: adjuvant chemotherapy; RT: adjuvant radiotherapy.
Footnotes
- Received December 2, 2009.
- Revision received February 4, 2010.
- Accepted February 9, 2010.
- Copyright © 2010 International Institute of Anticancer Research (Dr. John G. Delinassios), All rights reserved